Early High-Grade Transformation of IDH-Mutant Central Nervous System WHO Grade 2 Astrocytoma: A Case Report
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea
- 2Department of Pathology, National Cancer Center, Goyang, Korea
- 3Department of Neurological Surgery, Asan Hospital, University of Ulsan College of Medicine, Seoul, Korea
- 4Department of Cancer Control, Graduate School of Cancer Science and Policy, National Cancer Center, Goyang, Korea
- KMID: 2558437
- DOI: http://doi.org/10.14791/btrt.2024.0022
Abstract
- High-grade transformation of low-grade gliomas has long been a poor prognostic factor during therapy. In 2016, the World Health Organization (WHO) Classification of Tumors of the Central Nervous System (CNS) adopted isocitrate dehydrogenase (IDH) mutation status in the classification of diffuse astrocytomas. The 2021 classification denoted glioblastomas as IDH-wildtype and graded IDH-mutant astrocytomas as 2, 3, or 4. Gemistocytic morphology, a large proportion of residual tumor, the patient’s age, and recurrence after radiotherapy were previously mentioned as risk factors for high-grade transformation of low-grade gliomas. We report a 34-year-old male patient initially diagnosed with IDH-mutant grade 2 astrocytoma according to the 2021 WHO classification of CNS tumors. As the first surgical resection achieved gross total resection on postoperative MRI, no adjuvant therapy was given and regular follow-up was planned. On 1-year follow-up MRI, two new enhancing nodular lesions appeared at the ipsilateral brain parenchyma abutting the surgical resection cavity. Salvage craniotomy achieved gross total resection, and the pathologic diagnosis was IDH-mutant WHO grade 4 astrocytoma. We describe this tumor in terms of the previous WHO classification to evaluate the risk of high-grade transformation and discuss possible risk factors leading to high-grade transformation of low-grade astrocytoma.
Keyword
Figure
-
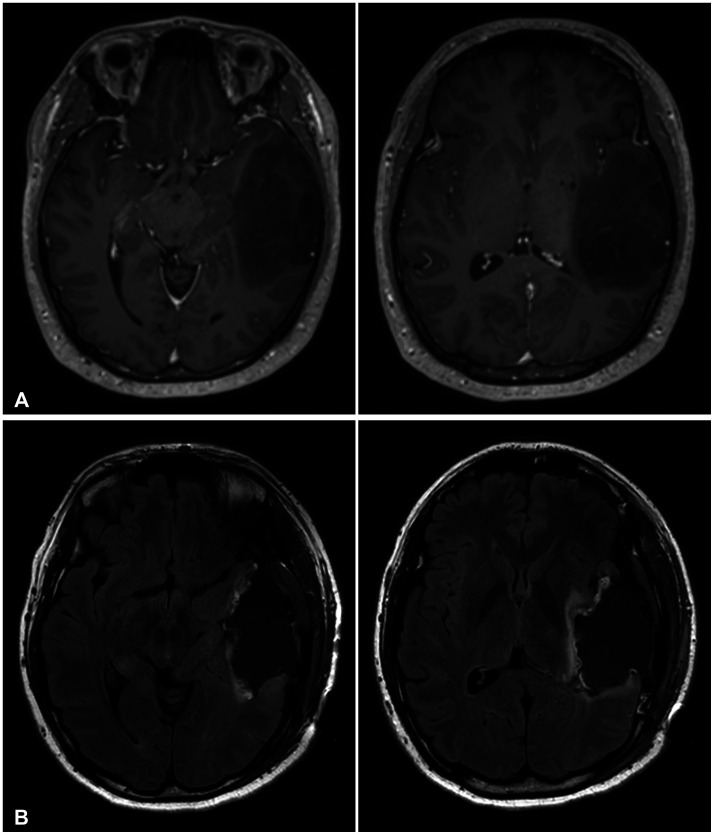
Fig. 1 Pre- and postoperative MRI findings of the first operation. A: Initial T1 contrast-enhanced MRI showing an approximately 8-cm diffuse, infiltrative, non-enhancing mass lesion in the left temporal lobe. B: Postoperative T1 contrast-enhanced MRI showing gross total resection with clear margins.
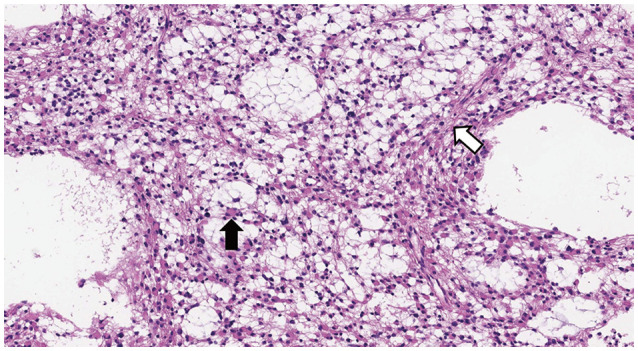
Fig. 2 Histopathological examination of the first operation (×200 magnification). Hematoxylin and eosin–stained tissue section showing gemistocytic features, with large eosinophilic cytoplasm with nuclei displaced to the periphery (black arrow). Other neoplastic fibrillary astrocytes show mild nuclear atypia on the background of a loosely structured tumor matrix with microcyst formation (white arrow).
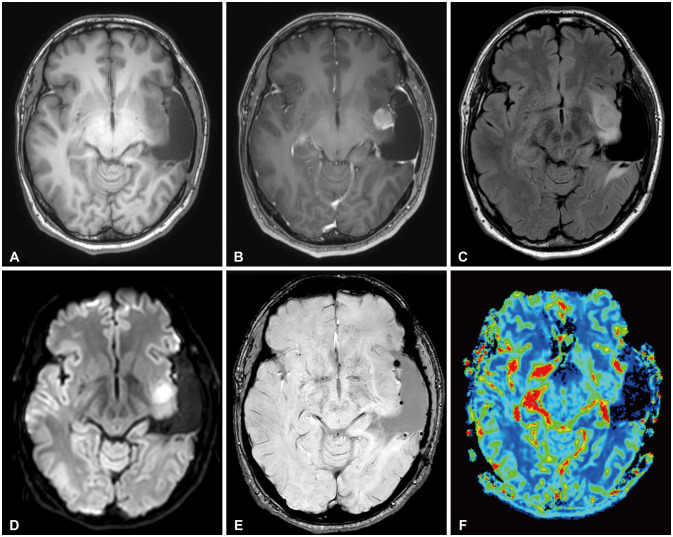
Fig. 3 Follow-up MRI 1 year after surgery showing a newly appeared, approximately 2-cm mass in the left insula. T1 non-enhanced (A), T1 contrast-enhanced (B), T2 fluid-attenuated inversion recovery (C), diffusion-weighted (D), susceptibility-weighted (E), and cerebral blood volume (F) images.
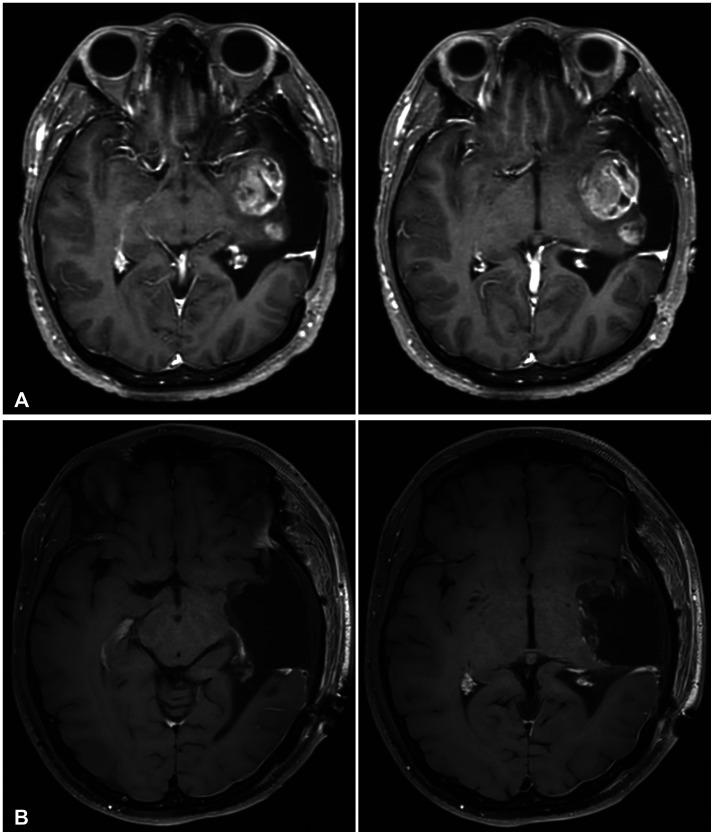
Fig. 4 Pre- and postoperative MRI findings of the second operation. A: T1 contrast-enhanced MRI showing marked growth of the left insular mass, with a newly appeared daughter mass in the posterior aspect. B: Postoperative T1 contrast-enhanced MRI showing gross total resection of both mass lesions.

Fig. 5 Histopathological examination of the second operation (×200 magnification). A: Hematoxylin and eosin–stained tissue section showing microvascular proliferation. B: Same hematoxylin and eosin-stain showing bizarre, monstrous, multinucleated tumor cells with high cellularity (black arrows). The nuclei varied in size, and some cells showed atypical mitoses (white arrow). C: Immunohistochemical staining positive for IDH mutation (using IDH1 R132H monoclonal antibody).
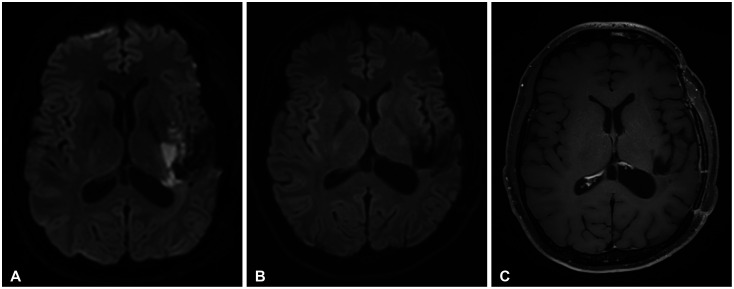
Fig. 6 Unexpected postoperative cerebral infarction and follow-up MRI. A: Diffusion-weighted MRI 4 days after surgery revealed multifocal diffusion restriction at the left internal capsule posterior limb, posterior thalamus, and corona radiata, indicative of acute infarction. Diffusion-weighted (B) and T1 contrast-enhanced (C) MRI before standard concurrent chemoradiation therapy showed minimal cerebromalacia at the infarction site without any enhancing lesions.
Reference
-
1. Jaeckle KA, Decker PA, Ballman KV, Flynn PJ, Giannini C, Scheithauer BW, et al. Transformation of low grade glioma and correlation with outcome: an NCCTG database analysis. J Neurooncol. 2011; 104:253–259. PMID: 21153680.2. Murphy ES, Leyrer CM, Parsons M, Suh JH, Chao ST, Yu JS, et al. Risk factors for malignant transformation of low-grade glioma. Int J Radiat Oncol Biol Phys. 2018; 100:965–971. PMID: 29485076.3. Johnson BE, Mazor T, Hong C, Barnes M, Aihara K, McLean CY, et al. Mutational analysis reveals the origin and therapy-driven evolution of recurrent glioma. Science. 2014; 343:189–193. PMID: 24336570.4. Park CK, Park I, Lee S, Sun CH, Koh Y, Park SH, et al. Genomic dynamics associated with malignant transformation in IDH1 mutated gliomas. Oncotarget. 2015; 6:43653–43666. PMID: 26524630.5. Jung TY, Jung S, Moon JH, Kim IY, Moon KS, Jang WY. Early prognostic factors related to progression and malignant transformation of low-grade gliomas. Clin Neurol Neurosurg. 2011; 113:752–757. PMID: 21889256.6. Babu R, Bagley JH, Park JG, Friedman AH, Adamson C. Low-grade astrocytomas: the prognostic value of fibrillary, gemistocytic, and protoplasmic tumor histology. J Neurosurg. 2013; 119:434–441. PMID: 23662821.7. Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol. 2021; 23:1231–1251. PMID: 34185076.8. Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, et al. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. 2016; 131:803–820. PMID: 27157931.9. Ohgaki H, Kleihues P. The definition of primary and secondary glioblastoma. Clin Cancer Res. 2013; 19:764–772. PMID: 23209033.10. Yan H, Parsons DW, Jin G, McLendon R, Rasheed BA, Yuan W, et al. IDH1 and IDH2 mutations in gliomas. N Engl J Med. 2009; 360:765–773. PMID: 19228619.11. Gorovets D, Kannan K, Shen R, Kastenhuber ER, Islamdoust N, Campos C, et al. IDH mutation and neuroglial developmental features define clinically distinct subclasses of lower grade diffuse astrocytic glioma. Clin Cancer Res. 2012; 18:2490–2501. PMID: 22415316.12. Eckel-Passow JE, Lachance DH, Molinaro AM, Walsh KM, Decker PA, Sicotte H, et al. Glioma groups based on 1p/19q, IDH, and TERT promoter mutations in tumors. N Engl J Med. 2015; 372:2499–2508. PMID: 26061753.13. Kim YZ, Kim CY, Lim DH. The overview of practical guidelines for gliomas by KSNO, NCCN, and EANO. Brain Tumor Res Treat. 2022; 10:83–93. PMID: 35545827.14. Weller M, van den Bent M, Preusser M, Le Rhun E, Tonn JC, Minniti G, et al. EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat Rev Clin Oncol. 2021; 18:170–186. PMID: 33293629.15. Liu V, Wetzel EA, Eldred BSC, Zapanta Rinonos S, Prins TJ, Khanlou N, et al. A single-institution retrospective analysis of pathologically determined malignant transformation in IDH mutant glioma patients. Neurooncol Adv. 2023; 5:vdad036. PMID: 37152809.16. Okamoto Y, Di Patre PL, Burkhard C, Horstmann S, Jourde B, Fahey M, et al. Population-based study on incidence, survival rates, and genetic alterations of low-grade diffuse astrocytomas and oligodendrogliomas. Acta Neuropathol. 2004; 108:49–56. PMID: 15118874.17. Tihan T, Vohra P, Berger MS, Keles GE. Definition and diagnostic implications of gemistocytic astrocytomas: a pathological perspective. J Neurooncol. 2006; 76:175–183. PMID: 16132490.18. Watanabe K, Tachibana O, Yonekawa Y, Kleihues P, Ohgaki H. Role of gemistocytes in astrocytoma progression. Lab Invest. 1997; 76:277–284. PMID: 9042164.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hemorrhagic Recurrence in Diffuse Astrocytoma without Malignant Transformation
- Molecular Testing of Brain Tumor
- Intracranial Metastases of Cervical Intramedullary Low-Grade Astrocytoma without Malignant Transformation in Adult
- Malignant Transformation of Meningioma With TERT Promoter Mutation: A Case Report
- The prognostic significance of p16 expression pattern in diffuse gliomas
