Elemental characteristics of sialoliths extracted from a patient with recurrent sialolithiasis
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, Dental Research Institute, School of Dentistry, Seoul National University, Seoul, Korea
- KMID: 2555739
- DOI: http://doi.org/10.5125/jkaoms.2024.50.2.94
Abstract
- The exact mechanism of sialolith formation has yet to be determined. Recurrence of sialolithiasis is rare, affecting only 1%-10% of patients. The current study presents a case of recurrent stones that occurred twice on the right submandibular gland 6 months postoperative and 7 months after reoperation in a 48-year-old female patient. The stones were analyzed using histology, scanning electron microscopy, energy dispersive spectroscopy, and transmission electron microscopy (TEM). The first stone showed a three-layered structure with a poorly mineralized peripheral multilayered zone, highly mineralized middle layer, and the central nidus. The stones were composed of Ca, C, O, Cu, F, N, P, Si, Zn, and Zr. In TEM, compact bi-layered bacterial cell membrane was found on the peripheral layer and the central nidus of the stone as well as exosomes in the central nidus. The results demonstrated the essential components of sialolith formation, including bacteria, inflammatory exosomes, and exfoliated salivary epithelial cells that cooperatively underwent the pathogenetic progresses of central nidus formation, induction of compact zone calcification of the middle layer, and repeated subsequent deposition in the peripheral multilayer zone. The rapid recurrence could have resulted from residual pieces of a sialolith acting as the nidus of bacterial infection.
Keyword
Figure
-
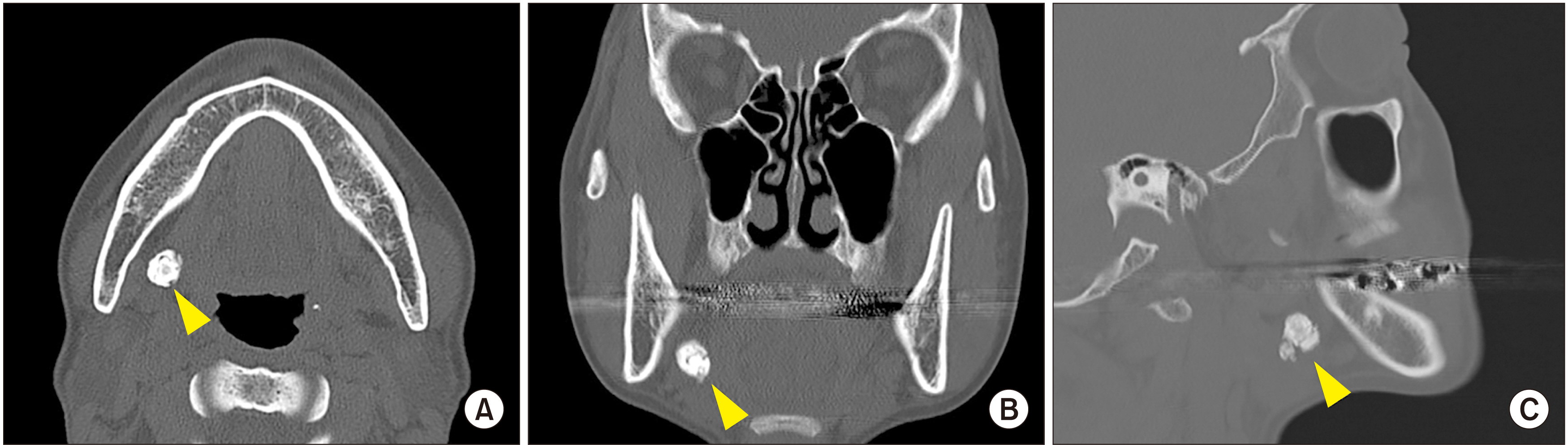
Fig. 1 Preoperative computed tomography images showing a 13-mm round radiopaque mass (arrowheads) on the hilar portion of the right submandibular glands in the axial (A), coronal (B), and sagittal view (C).

Fig. 2 A. Panoramic view revealed the presence of a stone in the submandibular gland area (arrowheads). B. During the first sialolithotomy operation, the stone was identified after access opening through a transoral approach. C. A 1.4 cm×0.7 cm×1.1 cm stone was retrieved. D. The panoramic radiograph showed signs of recurrence (arrowheads). E. The second surgery consisting of ductoplasty-sialendoscopy was performed 6 months later after signs of recurrence were observed. F. The retrieved stone. G. The panoramic radiograph showed the presence of a recurrent stone in the same area of the submandibular gland with a higher radiopacity compared with the previous radiograph (arrowheads). H. For the third sialolithotomy, the stone was identified in the same site as in the previous surgery. I. A 0.6 cm×0.4 cm×0.3 cm stone was retrieved.

Fig. 3 A. Histological findings of the second stone showing no distinct core (H&E staining, 4×; scale bar=500 μm). B. Highly mineralized globular structures found in the center of the sialolith (black arrows; H&E staining, 20×; scale bar=50 μm). C. Details of alternating layers of mineralized globular structures (black arrows; H&E staining, 20×; scale bar=50 μm). D. Amorphous basophilic materials with mineralized nodules (black arrowhead; H&E staining, 20×; scale bar=50 μm). E. Histological findings of the third stone showing no distinct core (H&E staining, 4×; scale bar=500 μm). F. A nodule with a highly mineralized outer layer (black asterisk; H&E staining, 20×; scale bar=50 μm). G. Alternating layers of mineralized and less mineralized globular structures (H&E staining, 20×; scale bar=50 μm). H. Globular structures in the outer layer (black arrows; H&E staining, 20×; scale bar=50 μm).

Fig. 4 Combined scanning electron microscopy images of the third stone with 14 points of interest. A long rod-shaped bacterial biofilm cave (yellow arrowheads) was observed with calcium nanoparticles at point 01. Points 02, 03, and 04 exhibited dense hydroxyapatite aggregation with empty bacterial casts (blue arrowheads). Fibrous and irregularly shaped hydroxyapatite crystals were randomly orientated at point 05. Point 06 showed irregularly shaped hydroxyapatite occurring in cluster masses or individual crystals (black arrowheads). Points 07, 09, and 11 revealed coarser hydroxyapatite crystal aggregation. Points 08 and 14 showed a densely aggregated layer of microscopic mineral masses compatible with octacalcium phosphate. Carbonate apatite with different orientations was observed at point 10 (red arrowheads). Calcite-like crystals were noted at point 13 (blue arrows).

Fig. 5 Energy dispersive spectroscopy (EDS) results of the third stone with five representative points of interest on the peripheral (P), middle (M), and core (C) layers. (SEM: scanning electron microscopy)

Fig. 6 A, B. Representative transmission electron microscopy images of the first sialolith. Bacteria with double membranes are observed on the peripheral layer of the stone (yellow arrowheads; A: 2,000×, B: 10,000×). C, D. A homogenous structure of exosome (blue arrowheads; C: 2,000×, D: 1,000×). E, F. Two epithelial cells (marked with black arrows) and a desmosome (white arrow; E: 2,000×, F: 10,000×). G. The nucleus and the endoplasmic reticulum of the epithelial cell (asterisk; 6,000×). H. The desmosome of the cell at higher magnification (20,000×).

Fig. 7 A, B. In the peripheral lamella of the second stone, exosomes (blue arrowheads; 3,000×) and a homogenous layer of organic compounds was found (yellow arrowheads; 20,000×). C, D. Exosomes (C: 3,000×, D: 10,000×). E, F. Deposition of inorganic matter in the inner side of the cell (white arrows; E: 3,000×, F: 20,000×). G, H. Clusters of prismatic and hexagonal hydroxyapatite crystals (G: 3,000×, H: 20,000×).
Reference
-
References
1. Barry R, Schaitkin BM, Walvekar RR. Gillespie MB, Walvekar RR, Schaitkin BM, Eisele DW, editors. 2018. Submandibular stones. Gland-preserving salivary surgery: a problem-based approach. Springer;p. 57–68. DOI: 10.1007/978-3-319-58335-8_6. PMCID: PMC6702475.
Article2. Lim HK, Kim SM, Kim MJ, Lee JH. 2012; Clinical, statistical and chemical study of sialolithiasis. J Korean Assoc Oral Maxillofac Surg. 38:44–9. https://doi.org/10.5125/jkaoms.2012.38.1.44. DOI: 10.5125/jkaoms.2012.38.1.44.
Article3. Koch M, Schapher M, Mantsopoulos K, Goncalves M, Iro H. 2019; Intraductal pneumatic lithotripsy after extended transoral duct surgery in submandibular sialolithiasis. Otolaryngol Head Neck Surg. 160:63–9. https://doi.org/10.1177/0194599818802224. DOI: 10.1177/0194599818802224. PMID: 30296893.
Article4. Nolasco P, Anjos AJ, Marques JM, Cabrita F, da Costa EC, Maurício A, et al. 2013; Structure and growth of sialoliths: computed microtomography and electron microscopy investigation of 30 specimens. Microsc Microanal. 19:1190–203. https://doi.org/10.1017/s1431927613001694. DOI: 10.1017/S1431927613001694. PMID: 24001782.
Article5. Austin T, Davis J, Chan T. 2004; Sialolithiasis of submandibular gland. J Emerg Med. 26:221–3. https://doi.org/10.1016/j.jemermed.2003.07.007. DOI: 10.1016/j.jemermed.2003.07.007. PMID: 14980352.
Article6. Schapher M, Koch M, Weidner D, Scholz M, Wirtz S, Mahajan A, et al. 2020; Neutrophil extracellular traps promote the development and growth of human salivary stones. Cells. 9:2139. https://doi.org/10.3390/cells9092139. DOI: 10.3390/cells9092139. PMID: 32971767. PMCID: PMC7564068.
Article7. Trujillo O, Drusin MA, Rahmati R. 2017; Rapid recurrent sialolithiasis: altered stone composition and potential factors for recurrence. Laryngoscope. 127:1365–8. https://doi.org/10.1002/lary.26357. DOI: 10.1002/lary.26357. PMID: 27753112.
Article8. Kraaij S, Karagozoglu KH, Forouzanfar T, Veerman EC, Brand HS. 2014; Salivary stones: symptoms, aetiology, biochemical composition and treatment. Br Dent J. 217:E23. https://doi.org/10.1038/sj.bdj.2014.1054. DOI: 10.1038/sj.bdj.2014.1054. PMID: 25476659.
Article9. Duong LT, Kakiche T, Ferré F, Nawrocki L, Bouattour A. 2019; Management of anterior submandibular sialolithiasis. J Oral Med Oral Surg. 25:16. https://doi.org/10.1051/mbcb/2018039. DOI: 10.1051/mbcb/2018039.
Article10. Galli P, Ceva A, Foletti JM, Iline N, Giorgi R, Chossegros C, et al. 2021; Salivary gland lithiasis recurrence after minimally-invasive surgery: incidence, risk factors and prevention. Laryngoscope. 131:794–9. https://doi.org/10.1002/lary.28991. DOI: 10.1002/lary.28991. PMID: 32786079.
Article11. Kim JK, Shin SM, Lee H, Lee S. 2016; Factors affecting long-term outcome of transoral surgery for submandibular stones: a follow-up study of 125 patients. Clin Otolaryngol. 41:365–70. https://doi.org/10.1111/coa.12523. DOI: 10.1111/coa.12523. PMID: 26292653.
Article12. Avishai G, Ben-Zvi Y, Ghanaiem O, Chaushu G, Gilat H. 2020; Sialolithiasis-do early diagnosis and removal minimize post-operative morbidity? Medicina (Kaunas). 56:332. https://doi.org/10.3390/medicina56070332. DOI: 10.3390/medicina56070332. PMID: 32630773. PMCID: PMC7404452.
Article13. Koch M, Mantsopoulos K, Müller S, Sievert M, Iro H. 2021; Treatment of sialolithiasis: what has changed? An update of the treatment algorithms and a review of the literature. J Clin Med. 11:231. https://doi.org/10.3390/jcm11010231. DOI: 10.3390/jcm11010231. PMID: 35011971. PMCID: PMC8746135.
Article14. Gerni M, Foletti JM, Collet C, Chossegros C. 2017; Evaluation of the prevalence of residual sialolith fragments after transoral approach of Wharton's duct. J Craniomaxillofac Surg. 45:167–70. https://doi.org/10.1016/j.jcms.2016.04.011. DOI: 10.1016/j.jcms.2016.04.011. PMID: 28040303.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Giant sialolithiasis of the submandibular gland: a case report
- A Case of Multiple Sialoliths in Sublingual Gland Misdiagnosed as Sialoliths in Submandibular Gland
- Histopathology and ultrastructural findings of pediatric sialolithiasis: a brief communication
- Sialolithiasis in children: Three case reports
- Submandibular sialolithiasis with CT and scintigraphy: CT values and salivary gland excretion in the submandibular glands
