Single puncture combined lumbar erector spinae plane and quadratus lumborum block (SEQ block) in acetabular fracture surgeries: randomized clinical trial
- Affiliations
-
- 1Department of Anesthesia and Surgical Intensive Care, Faculty of Medicine, Alexandria University, Alexandria, Egypt
- KMID: 2550920
- DOI: http://doi.org/10.17085/apm.23011
Abstract
- Background
Acetabular fracture surgery can cause severe postoperative pain. A combined lumbar erector spinae plane block and paraspinous sagittal shift quadratus lumborum block may augment analgesia. Methods: Fifty two patients undergoing posterior column acetabular surgery were divided into: Group Single puncture combined lumbar Erector spinae and Quadratus lumborum block (SEQ), patients who received SEQ block before anesthesia; and Group morphine (MOR), those who received general anesthesia (GA) and morphine. Results: Demographic characteristics were comparable. The heart rate and mean arterial blood pressure were significantly lower in the SEQ group than in the MOR group between 60 and 180 min intraoperatively (P < 0.001). Postoperative resting and dynamic visual analogue scale scores in the SEQ group were significantly lower than those in the MOR group at all studied periods (P = 0.022-0.001), except at 20 and 24 h postoperatively. Fentanyl was required in all MOR group patients at a mean dose of 110.0 ± 28.42 µg while 18 patients required fentanyl in SEQ group at a mean dose of 60.55 ± 25.54 µg. Postoperative morphine consumption was significantly less in SEQ group (6.33 ± 2.37 mg) than MOR group (17.0 ± 2.55 mg). Postoperative nausea and vomiting were recorded in eight and four patients in MOR and SEQ group, respectively. No complications associated with the block technique were observed. Conclusions: The SEQ block reduces the postoperative opioid consumption and provides stable intra and postoperative hemodynamics without observed complications in posterior column acetabular surgery.
Keyword
Figure
-

Fig. 1. Consort flow diagram. SEQ: Single puncture combined lumbar Erector spinae and Quadratus lumborum block, MOR: morphine.

Fig. 2. Probe position during SEQ block technique. (A) Probe in the parasagittal plane about 4 cm lateral to the lumbar vertebrae spinous processes with needle entry point at the cephalic end of the probe; (B) caudal end of the probe has been rotated medially towards the lumbar spine until the hypoechoic shadow of the transverse process of L4 appears in the ultrasound image; (C) probe position corresponding to (A); (D) probe position corresponding to (B). SEQ, Single puncture combined lumbar Erector spinae and Quadratus lumborum block.

Fig. 3. Real ultrasound image of the steps of SEQ block. (A) Probe position about 4 cm parallel to lumbar vertebrae with transverse processes appearing in view; (B) characteristic sonographic image of three muscle layers from posterior to anterior: erector spinae, quadratus lumborum and psoas major muscle: (C) PSSS QL block, red arrow represents needle path to the endpoint of injection into the plane between QL and PM muscles in a craniocaudal direction with LA spreading caudally; (D) lumbar ESP block after the caudal end of the probe is rotated medially, here, transverse process of L4 appears in view. The red arrow represents needle path towards transverse process of L4. SEQ: Single puncture combined lumbar Erector spinae and Quadratus lumborum block, PSSS: paraspinous sagittal shift, QL: quadratus lumborum, PM: psoas muscle, LA: local anesthetic, ESP: erector spinae plane, ES: erector spinae muscle, Psoas: psoas major muscle, tr pr L4: transverse process of lumbar vertebra 4, tr pr L5: transverse process of lumbar vertebra 5.
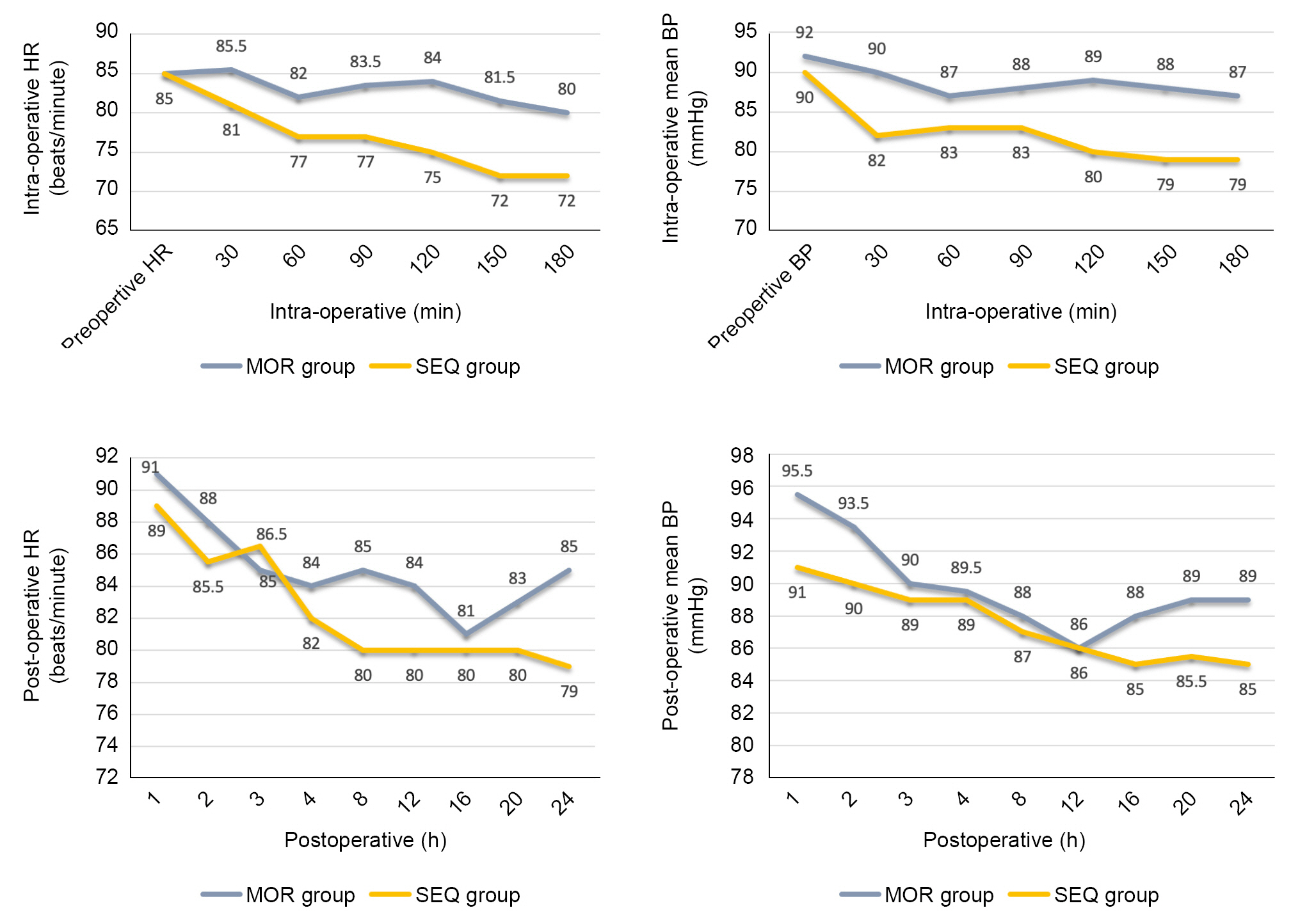
Fig. 4. Comparison of the intra-operative and post-operative hemodynamics between the two groups. MOR: morphine, SEQ: Single puncture combined lumbar Erector spinae and Quadratus lumborum block, BP: blood pressure, HR: heart rate. *P < 0.05 was considered statistically significant.

Fig. 5. Comparison between of the resting and dynamic VAS scores between the two groups. MOR: morphine, SEQ: Single puncture combined lumbar Erector spinae and Quadratus lumborum block, VAS: visual analogue scale. *P < 0.05 was considered statistically significant.
Reference
-
1. Chelly JE, Casati A, Al-Samsam T, Coupe K, Criswell A, Tucker J. Continuous lumbar plexus block for acute postoperative pain management after open reduction and internal fixation of acetabular fractures. J Orthop Trauma. 2003; 17:362–7.2. Strauss JE, O’Toole RV, Pollak AN. Does supplemental epidural anesthesia improve outcomes of acetabular fracture surgery? J Orthop Trauma. 2012; 26:67–72.
Article3. Vergari A, Frassanito L, Tamburello E, Nestorini R, Sala FD, Lais G, et al. Supra-inguinal fascia iliaca compartment block for postoperative analgesia after Acetabular fracture surgery. Injury. 2020; 51:2996–8.
Article4. Luftig J, Dreyfuss A, Mantuani D, Howell K, White A, Nagdev A. A new frontier in pelvic fracture pain control in the ED: successful use of the pericapsular nerve group (PENG) block. Am J Emerg Med. 2020; 38:2761.e5–9.
Article5. Ciftci B, Ekinci M, Celik EC, Yayik AM, Aydin ME, Ahiskalioglu A. Ultrasound-Guided erector spinae plane block versus modified-thoracolumbar interfascial plane block for lumbar discectomy surgery: a randomized, controlled study. World Neurosurg. 2020; 144:e849–55.
Article6. Celik M, Tulgar S, Ahiskalioglu A, Alper F. Is high volume lumbar erector spinae plane block an alternative to transforaminal epidural injection? Evaluation with MRI. Reg Anesth Pain Med. 2019; 44:906–7.
Article7. Tulgar S, Ermis MN, Ozer Z. Combination of lumbar erector spinae plane block and transmuscular quadratus lumborum block for surgical anaesthesia in hemiarthroplasty for femoral neck fracture. Indian J Anaesth. 2018; 62:802–5.
Article8. Ahiskalioglu A, Tulgar S, Celik M, Ozer Z, Alici HA, Aydin ME. Lumbar erector spinae plane block as a main anesthetic method for hip surgery in high risk elderly patients: initial experience with a magnetic resonance imaging. Eurasian J Med. 2020; 52:16–20.9. Alici HA, Ahiskalioglu A, Aydin ME, Ahiskalioglu EO, Celik M. High volume single injection lumbar erector spinae plane blockprovides effective analgesia for lower extremity herpes zoster. J Clin Anesth. 2019; 54:136–7.10. Tulgar S, Selvi O, Senturk O, Ermis MN, Cubuk R, Ozer Z. Clinical experiences of ultrasound-guided lumbar erector spinae plane block for hip joint and proximal femur surgeries. J Clin Anesth. 2018; 47:5–6.
Article11. González SD, Pomes J, Parts-Galino A, Garcia J, Martinez-Camacho A, Sala-Blanch X. Anatomical description of anaesthetic spread after deep erector spinae plane block at L-4. Rev Esp Anestesiol Reanim (Engl Ed). 2019; 66:409–16.12. Harbell MW, Seamans DP, Koyyalamudi V, Kraus MB, Craner RC, Langley NR. Evaluating the extent of lumbar erector spinae plane block: an anatomical study. Reg Anesth Pain Med. 2020; 45:640–4.
Article13. Hockett MM, Hembrador S, Lee A. Continuous quadratus lumborum block for postoperative pain in total hip arthroplasty: a case report. A A Case Rep. 2016; 7:129–31.14. La Colla L, Ben-David B, Merman R. Quadratus Lumborum block as an alternative to lumbar plexus block for hip surgery: a report of 2 cases. A A Case Rep. 2017; 8:4–6.
Article15. Kukreja P, MacBeth L, Sturdivant A, Morgan CJ, Ghanem E, Kalagara H, et al. Anterior quadratus lumborum block analgesia for total hip arthroplasty: a randomized, controlled study. Reg Anesth Pain Med. 2019; 44:1075–9.
Article16. Willard FH, Vleeming A, Schuenke MD, Danneels L, Schleip R. The thoracolumbar fascia: anatomy, function and clinical considerations. J Anat. 2012; 221:507–36.
Article17. Carline L, McLeod GA, Lamb C. A cadaver study comparing spread of dye and nerve involvement after three different quadratus lumborum blocks. Br J Anaesth. 2016; 117:387–94.
Article18. Alabd AS, Moustafa MA, Ahmed AMM. [Paraspinous Sagittal Shift (PSSS): a novel approach for transmuscular quadratus lumborum block for hip surgery analgesia – four case reports]. Braz J Anesthesiol. 2020; 70:178–83. Portuguese.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Erector Spinae Plane Block in Patients with Low Back Pain
- Erector spinae plane block for spinal surgery: a systematic review and meta-analysis
- Response to "Comment on Feasibility and efficacy of erector spinae plane block versus transversus abdominis plane block in laparoscopic bariatric surgery: a randomized comparative trial"
- Comment on "Feasibility and efficacy of erector spinae plane block versus transversus abdominis plane block in laparoscopic bariatric surgery: a randomized comparative trial"
- Anatomical classification and clinical application of thoracic paraspinal blocks
