Diagnostic performance of F-18 FDG PET or PET/CT for detection of recurrent gastric cancer: a systematic review and meta-analysis
- Affiliations
-
- 1Department of Surgery and Biomedical Research Institute, Pusan National University Hospital, Pusan National University College of Medicine, Busan, Korea
- KMID: 2548341
- DOI: http://doi.org/10.12701/jyms.2023.00220
Abstract
- Background
This systematic review and meta-analysis investigated the diagnostic performance of F-18 fluorodeoxyglucose (FDG) positron emission tomography (PET) or PET/computed tomography (PET/CT) for the detection of disease recurrence after curative resection of gastric cancer.
Methods
The PubMed and Embase databases, from the earliest available date of indexing through November 30, 2019, were searched for studies evaluating the diagnostic performance of F-18 FDG PET or PET/CT to detect recurrent disease after gastric cancer surgery.
Results
Across 17 studies (1,732 patients), the pooled sensitivity for F-18 FDG PET or PET/CT was 0.82 (95% confidence interval [CI], 0.74–0.88) with heterogeneity of I2=76.5 (p<0.001), and the specificity was 0.86 (95% CI, 0.78–0.91) with heterogeneity of I2=94.2 (p<0.001). Likelihood ratio (LR) tests gave an overall positive LR of 6.0 (95% CI, 3.6–9.7) and negative LR of 0.2 (95% CI, 0.14–0.31). The pooled diagnostic odds ratio was 29 (95% CI, 13–63). The summary receiver operating characteristic curve indicates that the area under the curve was 0.91 (95% CI, 0.88–0.93).
Conclusion
The current meta-analysis showed good sensitivity and specificity of F-18 FDG PET or PET/CT for detecting recurrent disease after curative resection of gastric cancer despite heterogeneity in ethnicity, recurrence rate, histology, and interpretation method.
Keyword
Figure
-
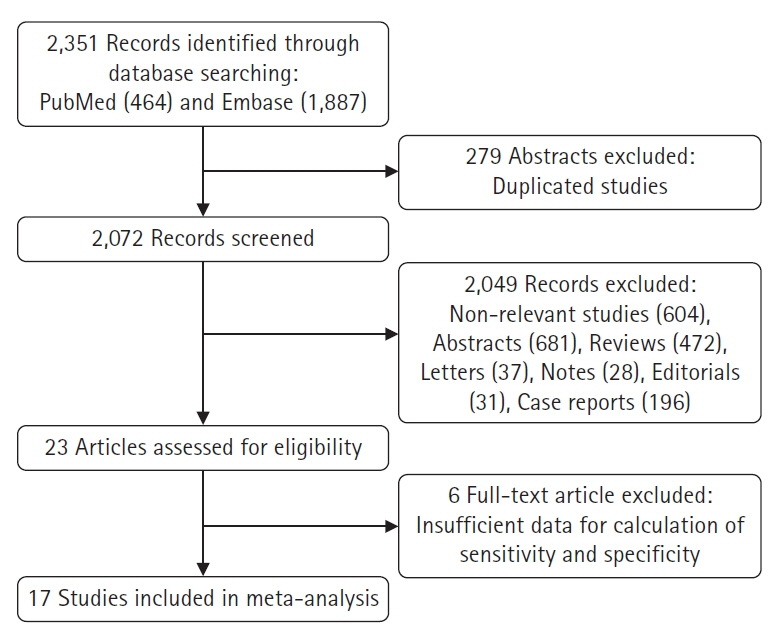
Fig. 1. Flowchart of the search for eligible studies on the diagnostic performance of F-18 FDG PET or PET/CT for detection of recurrent disease after curative resection of gastric cancer. FDG, fluorodeoxyglucose; PET, positron emission tomography; CT, computed tomography.

Fig. 2. Results of Deeks’ funnel plot of asymmetry test for publication bias. Non-significant slope indicates that no significant bias was found. ESS, effective sample size.

Fig. 3. Risk of bias and applicability concerns summary.
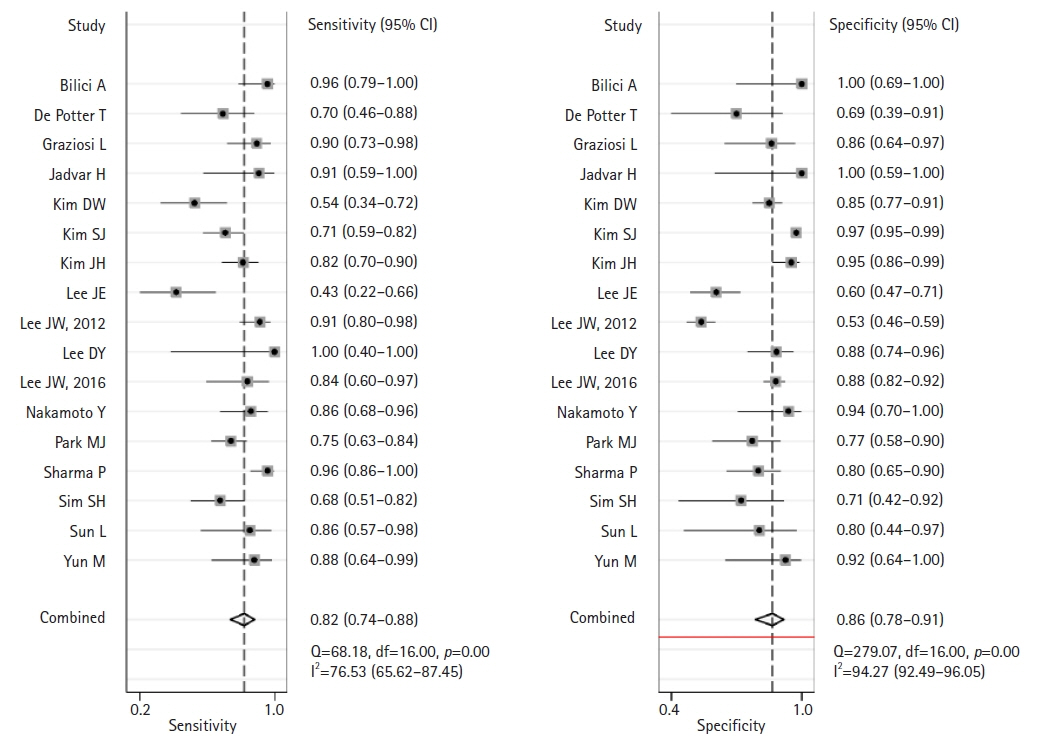
Fig. 4. Forest plot of pooled sensitivity and specificity of F-18 fluorodeoxyglucose positron emission tomography (PET) or PET/computed tomography for detection of disease recurrence after curative resection in patients with gastric cancer.
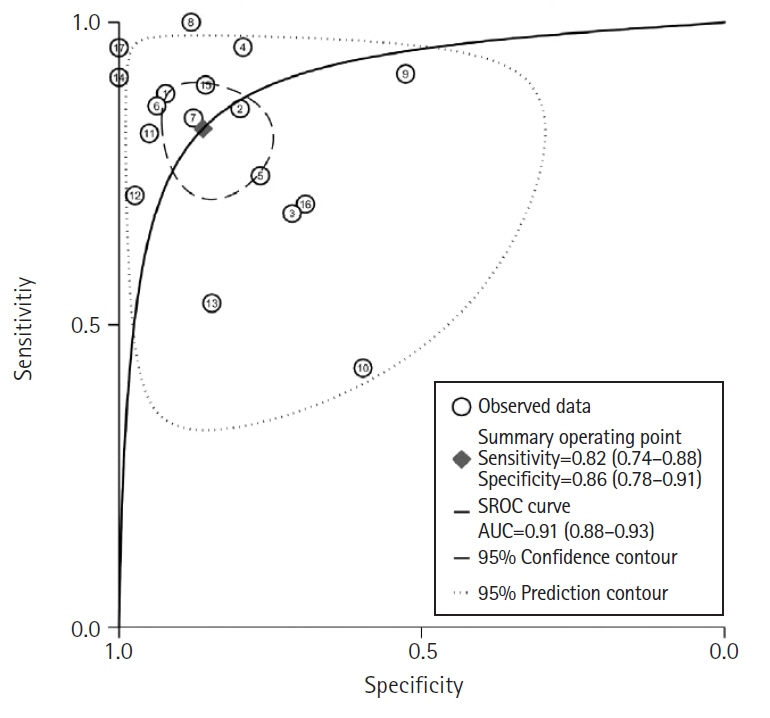
Fig. 5. The summary receiver operating characteristic (SROC) curves of F-18 fluorodeoxyglucose positron emission tomography (PET) or PET/computed tomography for detection of recurrent disease after curative resection of gastric cancer.
Reference
-
References
1. International Agency for Research on Cancer. Cancer fact sheet stomach: Globocan 2020 [Internet]. Geneva: World Health Organization;2022. [cited 2023 Apr 30]. https://gco.iarc.fr/today/data/factsheets/cancers/7-Stomach-fact-sheet.pdf.2. National Cancer Center; Korea Central Cancer Registry. Korean Cancer Report 2020. Goyang: National Cancer Center;2022.3. Japanese Gastric Cancer Association. Japanese Gastric Cancer Treatment Guidelines 2021 (6th edition). Gastric Cancer. 2023; 26:1–25.4. Park SH, Kang MJ, Yun EH, Jung KW. Epidemiology of Gastric Cancer in Korea: Trends in Incidence and Survival Based on Korea Central Cancer Registry Data (1999-2019). J Gastric Cancer. 2022; 22:160–8.
Article5. Blodgett TM, Meltzer CC, Townsend DW. PET/CT: form and function. Radiology. 2007; 242:360–85.
Article6. Czernin J, Allen-Auerbach M, Schelbert HR. Improvements in cancer staging with PET/CT: literature-based evidence as of September 2006. J Nucl Med. 2007; 48(1 Suppl):78S–88S.7. Bar-Shalom R, Yefremov N, Guralnik L, Gaitini D, Frenkel A, Kuten A, et al. Clinical performance of PET/CT in evaluation of cancer: additional value for diagnostic imaging and patient management. J Nucl Med. 2003; 44:1200–9.8. Bilici A, Ustaalioglu BB, Seker M, Kefeli U, Canpolat N, Tekinsoy B, et al. The role of 18F-FDG PET/CT in the assessment of suspected recurrent gastric cancer after initial surgical resection: can the results of FDG PET/CT influence patients' treatment decision making? Eur J Nucl Med Mol Imaging. 2011; 38:64–73.
Article9. De Potter T, Flamen P, Van Cutsem E, Penninckx F, Filez L, Bormans G, et al. Whole-body PET with FDG for the diagnosis of recurrent gastric cancer. Eur J Nucl Med Mol Imaging. 2002; 29:525–9.
Article10. Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011; 155:529–36.
Article11. Glas AS, Lijmer JG, Prins MH, Bonsel GJ, Bossuyt PM. The diagnostic odds ratio: a single indicator of test performance. J Clin Epidemiol. 2003; 56:1129–35.
Article12. Thompson SG. Why sources of heterogeneity in meta-analysis should be investigated. BMJ. 1994; 309:1351–5.
Article13. Deeks JJ, Macaskill P, Irwig L. The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J Clin Epidemiol. 2005; 58:882–93.
Article14. Hamza TH, van Houwelingen HC, Stijnen T. The binomial distribution of meta-analysis was preferred to model within-study variability. J Clin Epidemiol. 2008; 61:41–51.
Article15. Reitsma JB, Glas AS, Rutjes AW, Scholten RJ, Bossuyt PM, Zwinderman AH. Bivariate analysis of sensitivity and specificity produces informative summary measures in diagnostic reviews. J Clin Epidemiol. 2005; 58:982–90.
Article16. Rutter CM, Gatsonis CA. A hierarchical regression approach to meta-analysis of diagnostic test accuracy evaluations. Stat Med. 2001; 20:2865–84.
Article17. Lijmer JG, Mol BW, Heisterkamp S, Bonsel GJ, Prins MH, van der Meulen JH, et al. Empirical evidence of design-related bias in studies of diagnostic tests. JAMA. 1999; 282:1061–6.
Article18. Graziosi L, Bugiantella W, Cavazzoni E, Cantarella F, Porcari M, Baffa N, et al. Role of FDG-PET/CT in follow-up of patients treated with resective gastric surgery for tumour. Ann Ital Chir. 2011; 82:125–9.19. Jadvar H, Tatlidil R, Garcia AA, Conti PS. Evaluation of recurrent gastric malignancy with [F-18]-FDG positron emission tomography. Clin Radiol. 2003; 58:215–21.
Article20. Kim DW, Park SA, Kim CG. Detecting the recurrence of gastric cancer after curative resection: comparison of FDG PET/CT and contrast-enhanced abdominal CT. J Korean Med Sci. 2011; 26:875–80.
Article21. Kim SJ, Cho YS, Moon SH, Bae JM, Kim S, Choe YS, et al. Primary tumor ¹⁸F-FDG avidity affects the performance of ¹⁸F-FDG PET/CT for detecting gastric cancer recurrence. J Nucl Med. 2016; 57:544–50.
Article22. Kim JH, Heo SH, Kim JW, Shin SS, Min JJ, Kwon SY, et al. Evaluation of recurrence in gastric carcinoma: comparison of contrast-enhanced computed tomography and positron emission tomography/computed tomography. World J Gastroenterol. 2017; 23:6448–56.
Article23. Lee JE, Hong SP, Ahn DH, Jeon TJ, Kang MK, Kwon CI, et al. The role of 18F-FDG PET/CT in the evaluation of gastric cancer recurrence after curative gastrectomy. Yonsei Med J. 2011; 52:81–8.
Article24. Lee JW, Lee SM, Lee MS, Shin HC. Role of ¹⁸F-FDG PET/CT in the prediction of gastric cancer recurrence after curative surgical resection. Eur J Nucl Med Mol Imaging. 2012; 39:1425–34.
Article25. Lee DY, Lee CH, Seo MJ, Lee SH, Ryu JS, Lee JJ. Performance of (18)F-FDG PET/CT as a postoperative surveillance imaging modality for asymptomatic advanced gastric cancer patients. Ann Nucl Med. 2014; 28:789–95.
Article26. Lee JW, Lee SM, Son MW, Lee MS. Diagnostic performance of FDG PET/CT for surveillance in asymptomatic gastric cancer patients after curative surgical resection. Eur J Nucl Med Mol Imaging. 2016; 43:881–8.
Article27. Nakamoto Y, Togashi K, Kaneta T, Fukuda H, Nakajima K, Kitajima K, et al. Clinical value of whole-body FDG-PET for recurrent gastric cancer: a multicenter study. Jpn J Clin Oncol. 2009; 39:297–302.
Article28. Park MJ, Lee WJ, Lim HK, Park KW, Choi JY, Kim BT. Detecting recurrence of gastric cancer: the value of FDG PET/CT. Abdom Imaging. 2009; 34:441–7.
Article29. Sharma P, Singh H, Suman SK, Sharma A, Reddy RM, Thulkar S, et al. 18F-FDG PET-CT for detecting recurrent gastric adenocarcinoma: results from a Non-Oriental Asian population. Nucl Med Commun. 2012; 33:960–6.30. Sim SH, Kim YJ, Oh DY, Lee SH, Kim DW, Kang WJ, et al. The role of PET/CT in detection of gastric cancer recurrence. BMC Cancer. 2009; 9:73.
Article31. Sun L, Su XH, Guan YS, Pan WM, Luo ZM, Wei JH, et al. Clinical role of 18F-fluorodeoxyglucose positron emission tomography/computed tomography in post-operative follow up of gastric cancer: initial results. World J Gastroenterol. 2008; 14:4627–32.
Article32. Yun M, Choi HS, Yoo E, Bong JK, Ryu YH, Lee JD. The role of gastric distention in differentiating recurrent tumor from physiologic uptake in the remnant stomach on 18F-FDG PET. J Nucl Med. 2005; 46:953–7.33. Lee JH, Son SY, Lee CM, Ahn SH, Park DJ, Kim HH. Factors predicting peritoneal recurrence in advanced gastric cancer: implication for adjuvant intraperitoneal chemotherapy. Gastric Cancer. 2014; 17:529–36.
Article34. Whiting J, Sano T, Saka M, Fukagawa T, Katai H, Sasako M. Follow-up of gastric cancer: a review. Gastric Cancer. 2006; 9:74–81.
Article35. Kim KW, Choi BI, Han JK, Kim TK, Kim AY, Lee HJ, et al. Postoperative anatomic and pathologic findings at CT following gastrectomy. Radiographics. 2002; 22:323–36.
Article36. Lim JS, Kim MJ, Yun MJ, Oh YT, Kim JH, Hwang HS, et al. Comparison of CT and 18F-FDG pet for detecting peritoneal metastasis on the preoperative evaluation for gastric carcinoma. Korean J Radiol. 2006; 7:249–56.
Article37. Wu LM, Hu JN, Hua J, Gu HY, Zhu J, Xu JR. 18 F-fluorodeoxyglucose positron emission tomography to evaluate recurrent gastric cancer: a systematic review and meta-analysis. J Gastroenterol Hepatol. 2012; 27:472–80.38. Alakus H, Batur M, Schmidt M, Drebber U, Baldus SE, Vallböhmer D, et al. Variable 18F-fluorodeoxyglucose uptake in gastric cancer is associated with different levels of GLUT-1 expression. Nucl Med Commun. 2010; 31:532–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Imaging of Gastric Cancer Metabolism Using 18 F-FDG PET/CT
- Roles of F-18 FDG PET or PET/CT for the Evaluation of Gastrointestinal Malignancies
- The Role of 18F-FDG PET/CT in the Evaluation of Gastric Cancer Recurrence after Curative Gastrectomy
- Use of 18F-FDG PET/CT in Second Primary Cancer
- False Positive of F-18 FDG-PET/CT due to Activated Charcoal Granuloma from Intraperitoneal Chemotherapy: A Case Report
