The Role of 18F-FDG PET/CT in the Evaluation of Gastric Cancer Recurrence after Curative Gastrectomy
- Affiliations
-
- 1Digestive Disease Center, CHA Bundang Medical Center, CHA University, Seongnam, Korea. sphong@cha.ac.kr
- 2Department of Nuclear Medicine, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
- KMID: 1106441
- DOI: http://doi.org/10.3349/ymj.2011.52.1.81
Abstract
- PURPOSE
18F-fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) scans are frequently performed for the screening or staging of malignant tumors. This study aimed to assess the usefulness of 18F-FDG PET/CT in detection of gastric cancer recurrence after curative gastrectomy.
MATERIALS AND METHODS
Eighty nine patients who had undergone curative gastrectomy due to gastric cancer and had 18F-FDG PET/CT and contrast CT scans within 2 weeks for surveillance in asymptomatic patients (n = 11) or to clarify suspected recurrence (n = 78) were consecutively collected and retrospectively analyzed. They had clinical follow-up for at least 12 months after PET/CT and CT scans.
RESULTS
Fifteen of the 89 patients (16.9%) were diagnosed with recurrent gastric cancer in 21 organs. Forty one organs showed an increase in FDG uptake, and only 9 of these organs were diagnosed with recurrent gastric cancer by 18F-FDG PET/CT. The sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of the 18F-FDG PET/CT were 42.9%, 59.7%, 29.3%, 78.2%, and 57.3%, respectively. On the CT scan, 18 of 21 recurrent gastric cancers were detected, and 7 cases were in agreement with the 18F-FDG PET/CT. The sensitivity and specificity of the CT scan were 85.8% and 87.3%, respectively, which are superior to the 18F-FDG PET/CT. When we diagnosed a recurrence based on either 18F-FDG PET/CT or CT scans, the sensitivity increased to 95.2% and the specificity decreased to 45.6%, when compared with the contrast CT scan alone.
CONCLUSION
18F-FDG PET/CT is an insufficient diagnostic method in detection of recurrence after curative gastrectomy, and even less accurate than contrast CT scan alone.
MeSH Terms
Figure
-

Fig. 1 A case of recurring gastric cancer detected by FDG-uptake on PET/CT. This 57 year-old man showed no suspicion of recurrence on the abdomino-pelvic CT scan. However, on the whole body PET/CT scan, there was a high FDG-uptake on the left supraclavicular lymph node. This lesion was confirmed as distant nodal metastasis by biopsy. FDG, fluorodeoxyglucose; PET, positron emission.
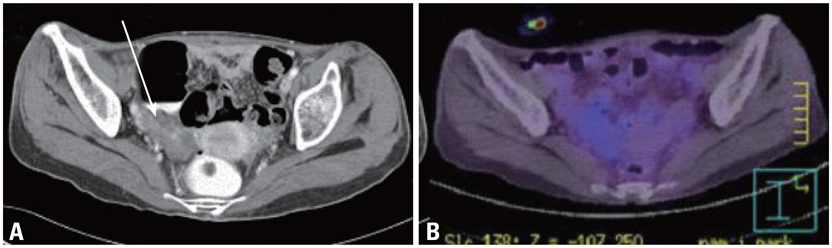
Fig. 2 A case of recurrent gastric cancer detected by CT scan but showing no FDG-uptake on PET/CT. (A) This 52 year-old woman showed peritoneal carcinomatosis and right ovarian enlargement with septated cystic mass on CT scan. (B) However, on the 18F-FDG PET/CT scan, there was no abnormal FDG-uptake. The recurrence was confirmed by peritoneal fluid cytology. FDG, fluorodeoxyglucose; PET, positron emission.
Cited by 2 articles
-
Imaging of Gastric Cancer Metabolism Using 18 F-FDG PET/CT
Mijin Yun
J Gastric Cancer. 2014;14(1):1-6. doi: 10.5230/jgc.2014.14.1.1.Diagnostic performance of F-18 FDG PET or PET/CT for detection of recurrent gastric cancer: a systematic review and meta-analysis
Chang In Choi, Jae Kyun Park, Tae Yong Jeon, Dae-Hwan Kim
J Yeungnam Med Sci. 2023;40(Suppl):S37-S46. doi: 10.12701/jyms.2023.00220.
Reference
-
1. Schwarz RE, Zagala-Nevarez K. Recurrence patterns after radical gastrectomy for gastric cancer: prognostic factors and implications for postoperative adjuvant therapy. Ann Surg Oncol. 2002. 9:394–400.
Article2. Yoo CH, Noh SH, Shin DW, Choi SH, Min JS. Recurrence following curative resection for gastric carcinoma. Br J Surg. 2000. 87:236–242.
Article3. Lim JS, Yun MJ, Kim MJ, Hyung WJ, Park MS, Choi JY, et al. CT and PET in stomach cancer: preoperative staging and monitoring of response to therapy. Radiographics. 2006. 26:143–156.
Article4. Habermann CR, Weiss F, Riecken R, Homarpisheh H, Bohnacker S, Staedtler C, et al. Preoperative staging of gastric adenocarcinoma: comparison of helical CT and endoscopic US. Radiology. 2004. 230:465–471.
Article5. Kuntz C, Herfarth C. Imaging diagnosis for staging of gastric cancer. Semin Surg Oncol. 1999. 17:96–102.
Article6. Halvorsen RA Jr, Yee J, McCormick VD. Diagnosis and staging of gastric cancer. Semin Oncol. 1996. 23:325–335.7. Park MJ, Lee WJ, Lim HK, Park KW, Choi JY, Kim BT. Detecting recurrence of gastric cancer: the value of FDG PET/CT. Abdom Imaging. 2009. 34:441–447.
Article8. Sun L, Su XH, Guan YS, Pan WM, Luo ZM, Wei JH, et al. Clinical role of 18F-fluorodeoxyglucose positron emission tomography/computed tomography in post-operative follow up of gastric cancer: initial results. World J Gastroenterol. 2008. 14:4627–4632.
Article9. Sim SH, Kim YJ, Oh DY, Lee SH, Kim DW, Kang WJ, et al. The role of PET/CT in detection of gastric cancer recurrence. BMC Cancer. 2009. 9:73.
Article10. De Potter T, Flamen P, Van Cutsem E, Penninckx F, Filez L, Bormans G, et al. Whole-body PET with FDG for the diagnosis of recurrent gastric cancer. Eur J Nucl Med Mol Imaging. 2002. 29:525–529.
Article11. Nakamoto Y, Togashi K, Kaneta T, Fukuda H, Nakajima K, Kitajima K, et al. Clinical value of whole-body FDG-PET for recurrent gastric cancer: a multicenter study. Jpn J Clin Oncol. 2009. 39:297–302.
Article12. Sobin LH, Wittekind CH. TNM classification of malignant tumors. International union against cancer (UICC). 2002. 6th ed. New York: Wilwy-Liss.13. Yun M, Kim BI. Roles of F-18 FDG PET or PET/CT for the evaluation of gastrointestinal malignancies. Korean J Gastroenterol. 2006. 48:378–387.14. Yun M, Choi HS, Yoo E, Bong JK, Ryu YH, Lee JD. The role of gastric distention in differentiating recurrent tumor from physiologic uptake in the remnant stomach on 18F-FDG PET. J Nucl Med. 2005. 46:953–957.15. Nunez RF, Yeung HW, Macapinlac H. Increased F-18 FDG uptake in the stomach. Clin Nucl Med. 1999. 24:281–282.
Article16. Beatty JS, Williams HT, Aldridge BA, Hughes MP, Vasudeva VS, Gucwa AL, et al. Incidental PET/CT findings in the cancer patient: how should they be managed? Surgery. 2009. 146:274–281.
Article17. Ishimori T, Patel PV, Wahl RL. Detection of unexpected additional primary malignancies with PET/CT. J Nucl Med. 2005. 46:752–757.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prognostic Value of Restaging F-18 Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography to Predict 3-Year Post-Recurrence Survival in Patients with Recurrent Gastric Cancer after Curative Resection
- Preoperative Nodal ¹â¸F-FDG Avidity Rather than Primary Tumor Avidity Determines the Prognosis of Patients with Advanced Gastric Cancer
- F18-fluorodeoxyglucose-positron emission tomography and computed tomography is not accurate in preoperative staging of gastric cancer
- Use of 18F-FDG PET/CT in Second Primary Cancer
- The Diagnostic Utility of PET-CT for the Preoperative Evaluation of Lymph Node Metastasis in Gastric Cancer Patients
