Clin Exp Otorhinolaryngol.
2023 Aug;16(3):251-258. 10.21053/ceo.2023.00619.
Treatment Efficacy of Various Maneuvers for Lateral Canal Benign Paroxysmal Positional Vertigo With Apogeotropic Nystagmus: A Randomized Controlled Trial
- Lee HJ
 1
1 - Jeon EJ1
- Nam S2
- Mun SK3
- Yoo SY4
- Bu SH5
- Choi JW6
- Chung JH7
- Hong SM8
- Lee SH7
- Kim MB9
- Koo JW10
- Kim HJ11
- Seo JH12
- Ahn SK13
- Park SN12
- Kim M14
- Chung WH15
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Incheon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Incheon, Korea
- 2Department of Otorhinolaryngology, Keimyung University Dongsan Hospital, Keimyung University School of Medicine, Daegu, Korea
- 3Department of Otorhinolaryngology-Head and Neck Surgery, Chung-Ang University College of Medicine, Seoul, Korea
- 4Myoung-dong Yonsei Ear Clinic, Seoul, Korea
- 5Department of Otorhinolaryngology-Head and Neck Surgery, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea
- 6Department of Otorhinolaryngology-Head and Neck Surgery, Chungnam National University College of Medicine, Daejeon, Korea
- 7Department of Otolaryngology-Head and Neck Surgery, Hanyang University College of Medicine, Seoul, Korea
- 8Department of Otorhinolaryngology-Head and Neck Surgery, Dongtan Sacred Heart Hospital, Hallym University College of Medicine, Hwaseong, Korea
- 9Department of Otorhinolaryngology-Head and Neck Surgery, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea
- 10Department of Otorhinolaryngology-Head and Neck Surgery, Seoul National University Bundang Hospital, Seongnam, Korea
- 11Department of Otorhinolaryngology-Head and Neck Surgery, Inha University College of Medicine, Incheon, Korea
- 12Department of Otolaryngology-Head and Neck Surgery, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 13Department of Otorhinolaryngology, Gyeongsang National University Hospital, Gyeongsang National University College of Medicine, Jinju, Korea
- 14Department of Otorhinolaryngology-Head and Neck Surgery, Catholic Kwandong University College of Medicine, Gangneung, Korea
- 15Department of Otorhinolaryngology-Head and Neck Surgery, Samsung Medical Center, Sungkyunkwan University, School of Medicine, Seoul, Korea
- KMID: 2545264
- DOI: http://doi.org/10.21053/ceo.2023.00619
Abstract
Objectives
The aim of this study was to determine the most effective treatment approach by comparing the impacts of various otolith reduction techniques in patients with apogeotropic lateral semicircular canal benign paroxysmal positional vertigo (LC-BPPV).
Methods
We performed a multicenter randomized prospective study from January to December 2015, involving 72 consecutive patients with apogeotropic LC-BPPV. The patients were divided into three treatment groups: therapeutic head-shaking (group A), the Gufoni-Appiani maneuver (group B), and the cupulolith repositioning maneuver (CuRM; group C). Each group underwent evaluation and treatment up to the fourth week. Treatment success was defined as the disappearance of positional vertigo and nystagmus.
Results
This study included 72 patients (49 male and 23 female), with a mean (±standard deviation) age of 55.4±13.5 years. The mean duration of vertigo experienced prior to treatment was 3.9±4.4 days. The mean latency and duration of nystagmus were 2.7±3.0 seconds and 47.9±15.8 seconds, respectively. The overall treatment frequency was 2.0±0.9. The number of treatments differed significantly among the three groups (P<0.05). After 4 weeks, the success rates for groups A, B, and C were 90.5%, 92.3%, and 100%, respectively. No significant difference was observed in the success rate across treatment methods and periods (P>0.05). However, CuRM was the only method with a 100% treatment success rate.
Conclusion
While no clear difference was observed among the three treatments for LC-BPPV, CuRM was found to be superior to the other approaches in the long term.
Keyword
Figure
-
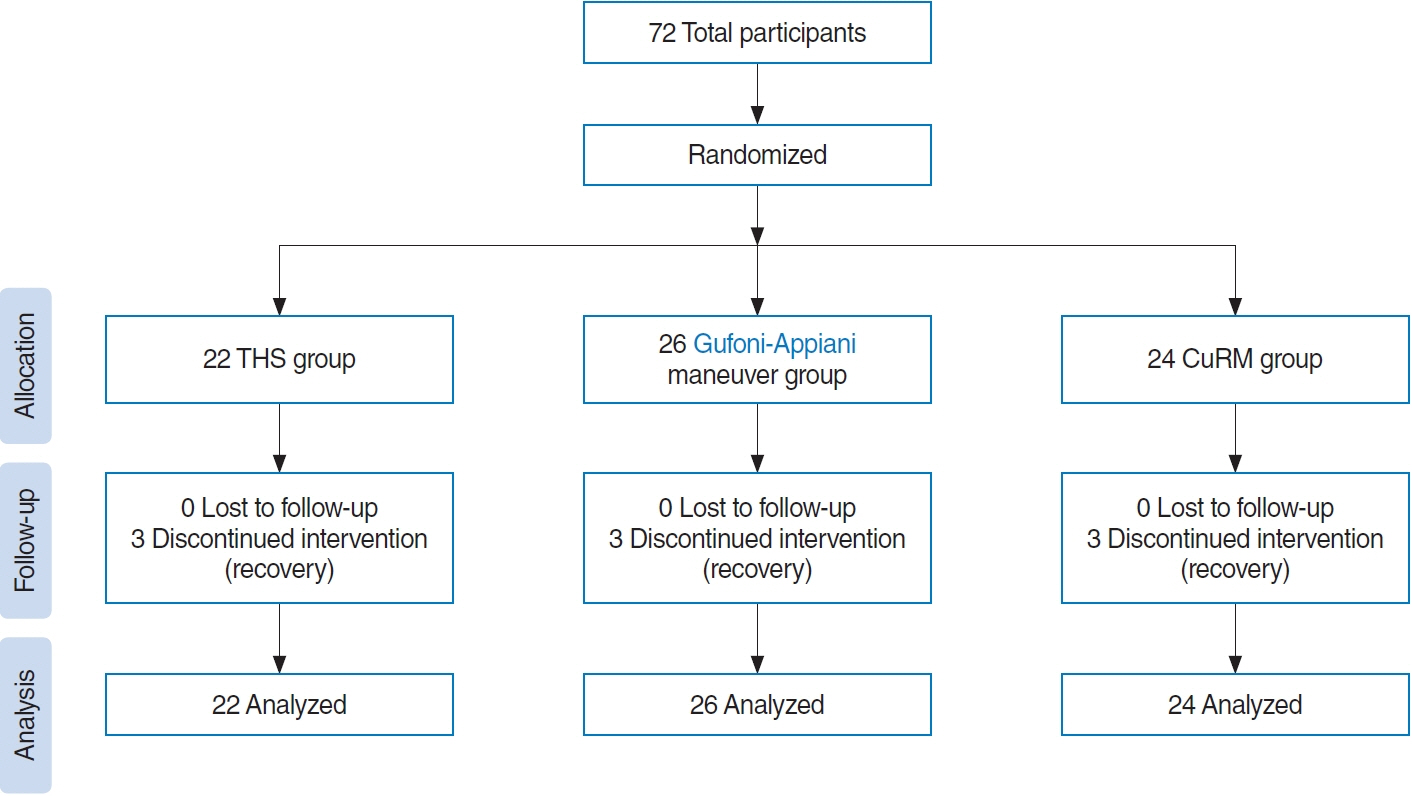
Fig. 1. Flow diagram illustrating the effects of various otolith reduction techniques in patients with apogeotropic lateral semicircular canal benign paroxysmal positional vertigo. THS, therapeutic head-shaking; CuRM, cupulolith repositioning maneuver.
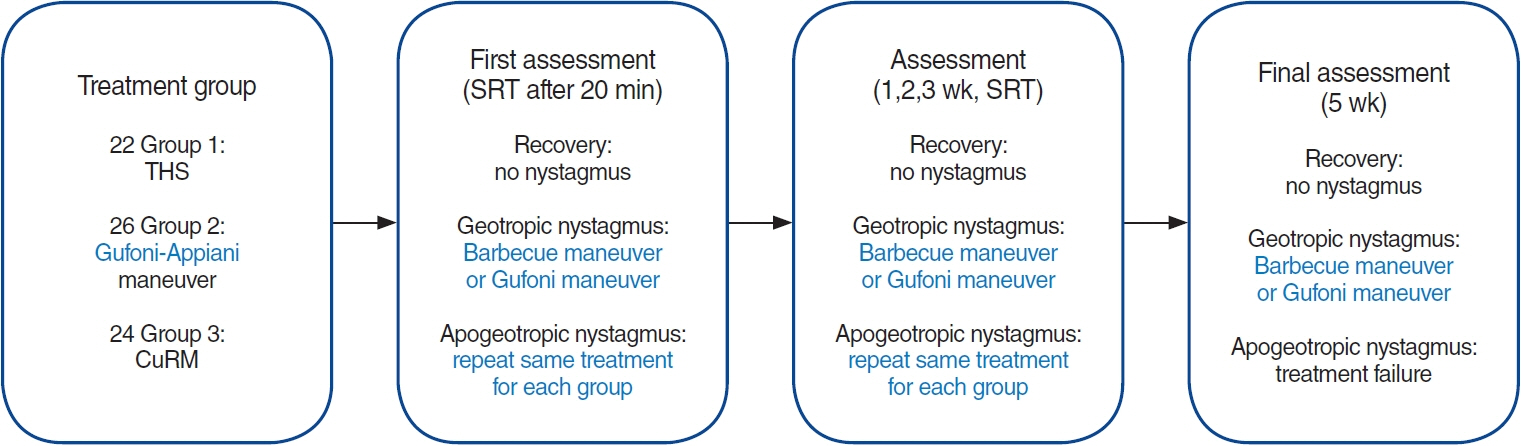
Fig. 2. A schematic representation of the study design. THS, therapeutic head-shaking; CuRM, cupulolith repositioning maneuver; SRT, supine roll test.

Fig. 3. The success rate of each otolith repositioning maneuver. THS, therapeutic head-shaking; CuRM, cupulolith repositioning maneuver; Total, mean success rate of the three treatments.
Reference
-
1. Parnes LS, Agrawal SK, Atlas J. Diagnosis and management of benign paroxysmal positional vertigo (BPPV). CMAJ. 2003; Sep. 169(7):681–93.2. von Brevern M, Radtke A, Lezius F, Feldmann M, Ziese T, Lempert T, et al. Epidemiology of benign paroxysmal positional vertigo: a population based study. J Neurol Neurosurg Psychiatry. 2007; Jul. 78(7):710–5.3. Anagnostou E, Kouzi I, Spengos K. Diagnosis and treatment of anterior-canal benign paroxysmal positional vertigo: a systematic review. J Clin Neurol. 2015; Jul. 11(3):262–7.4. Zuma E Maia F, Ramos BF, Cal R, Brock CM, Mangabeira Albernaz PL, Strupp M. Management of lateral semicircular canal benign paroxysmal positional vertigo. Front Neurol. 2020; Sep. 11:1040.5. Yu J, Gu Y, Meng G, Zhu X, Wang W, Liu X, et al. Nystagmus parameters of supine roll test correlates with prognosis after repositioning maneuver in horizontal semicircular canal benign paroxysmal positional vertigo. Front Neurol. 2021; Dec. 12:790430.6. Baloh RW, Yue Q, Jacobson KM, Honrubia V. Persistent direction-changing positional nystagmus: another variant of benign positional nystagmus. Neurology. 1995; Jul. 45(7):1297–301.7. Steddin S, Ing D, Brandt T. Horizontal canal benign paroxysmal positioning vertigo (h-BPPV): transition of canalolithiasis to cupulolithiasis. Ann Neurol. 1996; Dec. 40(6):918–22.8. Ramos BF, Cal R, Brock CM, Mangabeira Albernaz PL, Zuma e Maia F. Apogeotropic variant of horizontal semicircular canal benign paroxysmal positional vertigo: where are the particles. Audiol Res. 2019; Aug. 9(2):228.9. Oh SY, Kim JS, Jeong SH, Oh YM, Choi KD, Kim BK, et al. Treatment of apogeotropic benign positional vertigo: comparison of therapeutic head-shaking and modified Semont maneuver. J Neurol. 2009; Aug. 256(8):1330–6.10. Ciniglio Appiani G, Catania G, Gagliardi M, Cuiuli G. Repositioning maneuver for the treatment of the apogeotropic variant of horizontal canal benign paroxysmal positional vertigo. Otol Neurotol. 2005; Mar. 26(2):257–60.11. Vannucchi P, Giannoni B, Pagnini P. Treatment of horizontal semicircular canal benign paroxysmal positional vertigo. J Vestib Res. 1997; Jan-Feb. 7(1):1–6.12. Correia F, Castelhano L, Cavilhas P, Escada P. Lateral semicircular canal-BPPV: prospective randomized study on the efficacy of four repositioning maneuvers. Acta Otorrinolaringol Esp (Engl Ed). 2022; Jan-Feb. 73(1):27–34.13. Tirelli G, Russolo M. 360-Degree canalith repositioning procedure for the horizontal canal. Otolaryngol Head Neck Surg. 2004; Nov. 131(5):740–6.14. Kim SH, Jo SW, Chung WK, Byeon HK, Lee WS. A cupulolith repositioning maneuver in the treatment of horizontal canal cupulolithiasis. Auris Nasus Larynx. 2012; Apr. 39(2):163–8.15. Casani AP, Vannucci G, Fattori B, Berrettini S. The treatment of horizontal canal positional vertigo: our experience in 66 cases. Laryngoscope. 2002; Jan. 112(1):172–8.16. Koo JW, Moon IJ, Shim WS, Moon SY, Kim JS. Value of lying-down nystagmus in the lateralization of horizontal semicircular canal benign paroxysmal positional vertigo. Otol Neurotol. 2006; Apr. 27(3):367–71.17. Kong TH, Song MH, Kang JW, Shim DB. Double-blind randomized controlled trial on efficacy of cupulolith repositioning maneuver for treatment of apogeotropic horizontal canal benign paroxysmal positional vertigo. Acta Otolaryngol. 2020; Jun. 140(6):473–8.18. Gufoni M, Mastrosimone L, Di Nasso F. Repositioning maneuver in benign paroxysmal vertigo of horizontal semicircular canal. Acta Otorhinolaryngol Ital. 1998; Dec. 18(6):363–7.19. Lempert T, Tiel-Wilck K. A positional maneuver for treatment of horizontal-canal benign positional vertigo. Laryngoscope. 1996; Apr. 106(4):476–8.20. Jeon EJ, Chung WH, Choi JH, Nam EC, Park HJ, Lee JD, et al. Multicenter study on the clinician’s diagnostic and therapeutic approaches for benign paroxysmal positional vertigo in Korea. Res Vestib Sci. 2013; Sep. 12(3):79–92.21. Cakir BO, Ercan I, Cakir ZA, Civelek S, Sayin I, Turgut S. What is the true incidence of horizontal semicircular canal benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg. 2006; Mar. 134(3):451–4.22. Shim DB, Ko KM, Lee JH, Park HJ, Song MH. Natural history of horizontal canal benign paroxysmal positional vertigo is truly short. J Neurol. 2015; Jan. 262(1):74–80.23. Zuma e Maia F. New treatment strategy for apogeotropic horizontal canal benign paroxysmal positional vertigo. Audiol Res. 2016; Nov. 6(2):163.24. Kim JS, Oh SY, Lee SH, Kang JH, Kim DU, Jeong SH, et al. Randomized clinical trial for apogeotropic horizontal canal benign paroxysmal positional vertigo. Neurology. 2012; Jan. 78(3):159–66.25. Li JC. Mastoid oscillation: a critical factor for success in canalith repositioning procedure. Otolaryngol Head Neck Surg. 1995; Jun. 112(6):670–5.26. Motamed M, Osinubi O, Cook JA. Effect of mastoid oscillation on the outcome of the canalith repositioning procedure. Laryngoscope. 2004; Jul. 114(7):1296–8.27. Sargent EW, Bankaitis AE, Hollenbeak CS, Currens JW. Mastoid oscillation in canalith repositioning for paroxysmal positional vertigo. Otol Neurotol. 2001; Mar. 22(2):205–9.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Central Apogeotropic Direction Changing Positional Nystagmus due to Fourth Ventricle Mass Mimicking Horizontal Canal Cupulolithiasis Benign Paroxysmal Positional Vertigo
- Isolated Cerebellar Nodular Infarction with Apogeotropic Central Paroxysmal Positional Nystagmus
- Clinical Significance of Spontaneous Nystagmus in Horizontal Semicircular Canal Benign Paroxysmal Positional Vertigo
- A Case of Horizontal Canal Benign Paroxysmal Positional Vertigo
- Positional Dizziness and Vertigo without Nystagmus and Orthostatic Hypotension
