Ann Pediatr Endocrinol Metab.
2023 Jun;28(2):144-148. 10.6065/apem.2142218.109.
Combination therapy of liothyronine and levothyroxine for hypothyroidism-induced dilated cardiomyopathy
- Affiliations
-
- 1Department of Pediatrics, Severance Children's Hospital, Endocrine Research Institute, Yonsei University College of Medicine, Seoul, Korea
- 2Division of Pediatric Cardiology, Department of Pediatrics, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea
- 3Department of Pediatrics, Inha University Hospital, Incheon, Korea
- 4Department of Pediatrics, Gangnam Severance Hospital, Yonsei University College of Medicine , Seoul, Korea
- KMID: 2543296
- DOI: http://doi.org/10.6065/apem.2142218.109
Abstract
- Thyroid hormone plays a vital role in regulating human metabolism. They affect the functions of major organs, such as the brain, liver, skeletal muscle, and heart. Hypothyroidism can lead to dilated cardiomyopathy and decreased heart function. In this report, we describe a case of a teenage boy who developed dilated cardiomyopathy due to hypothyroidism and was considered to undergo heart transplantation. Levothyroxine monotherapy was initiated but produced no improvement. Thereafter, a combination therapy of liothyronine and levothyroxine was administered, and heart function was gradually restored; he recovered completely after 6 months. Cardiac myocytes respond more specifically to liothyronine than to levothyroxine. Therefore, we suggest that liothyronine and levothyroxine combination therapy should be considered rather than levothyroxine monotherapy for hypothyroidism accompanied by heart disease.
Keyword
Figure
-

Fig. 1. Chest x-ray on the first day after transfer. Chest x-ray showed cardiomegaly and right pleural effusion in initial chest x-ray (A) and showed normal findings at 12 months of follow-up (B).

Fig. 2. Markedly enlarged left ventricle with moderate mitral regurgitation was seen in the initial apical four-chamber view via transthoracic echocardiography (A), and decreased left ventricle to normal range without mitral regurgitation was seen in the same view at 12 months of follow-up (B).
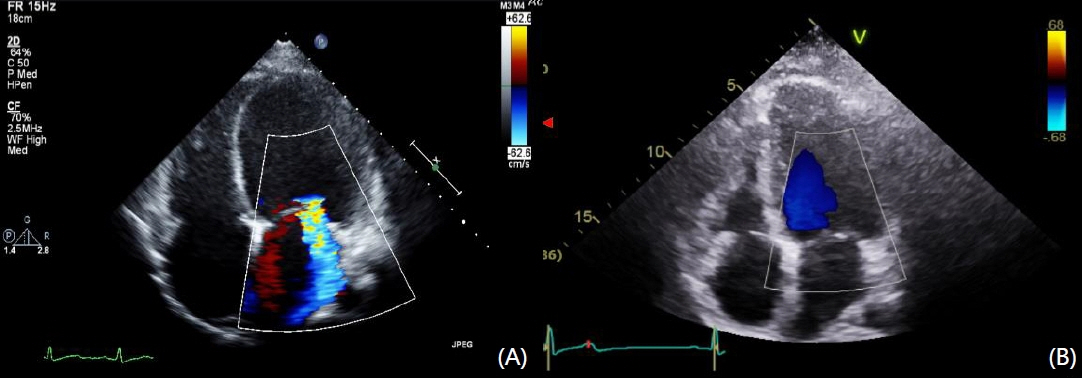
Fig. 3. The 12-lead electrocardiography findings. The patient had sinus tachycardia in initial electrocardiography (A) and normal sinus rhythm at 12 months of follow-up (B).
Reference
-
References
1. Brent GA. Mechanisms of thyroid hormone action. J Clin Invest. 2012; 122:3035–43.2. Mullur R, Liu YY, Brent GA. Thyroid hormone regulation of metabolism. Physiol Rev. 2014; 94:355–82.3. Klein I, Danzi SJC. Thyroid disease and the heart. 2007; 116:1725–35.4. Cohn JN, Bristow MR, Chien KR, Colucci WS, Frazier OH, Leinwand LA, et al. Report of the National Heart, Lung, and Blood Institute Special Emphasis Panel on Heart Failure Research. Circulation. 1997; 95:766–70.5. Davis PJ, Davis FB. Acute cellular actions of thyroid hormone and myocardial function. Ann Thorac Surg. 1993; 56(1 Suppl):S16–23.6. Klein I, Danzi S. Thyroid hormone treatment to mend a broken heart. J Clin Endocrinol Metab. 2008; 93:1172–4.7. Henderson KK, Danzi S, Paul JT, Leya G, Klein I, Samarel AM. Physiological replacement of T3 improves left ventricular function in an animal model of myocardial infarction-induced congestive heart failure. Circ Heart Fail. 2009; 2:243–52.8. Brent G, Davies T, Larsen P. Hypothyroidism and thyroiditis. In : Kronenberg HM, Melmed S, Polonsky KS, Larsen PR, editors. Williams textbook of endocrinology. 11th ed. Philadelphia (PA): Elsevier;2008. p. 406–35.9. Wang W, Guan H, Gerdes AM, Iervasi G, Yang Y, Tang Y-DJTJoCE, et al. Thyroid status, cardiac function, and mortality in patients with idiopathic dilated cardiomyopathy. J Clin Endocrinol Metab. 2015; 100:3210–8.10. Bozkurt B, Colvin M, Cook J, Cooper LT, Deswal A, Fonarow GC, et al. Current diagnostic and treatment strategies for specific dilated cardiomyopathies: a scientific statement from the American Heart Association. Circulation. 2016; 134:e579–646.11. Bezdah L, Slimène H, Kammoun M, Haddad A, Belhani A. Hypothyroid dilated cardiomyopathy. Ann Cardiol Angeiol (Paris). 2004; 53:217–20. French.12. Jansen J, Friesema EC, Kester MH, Schwartz CE, Visser TJ. Genotype-phenotype relationship in patients with mutations in thyroid hormone transporter MCT8. Endocrinology. 2008; 149:2184–90.13. Visser WE, Wong WS, van Mullem AA, Friesema EC, Geyer J, Visser TJ. Study of the transport of thyroid hormone by transporters of the SLC10 family. Mol Cell Endocrinol. 2010; 315:138–45.14. Klein I, Danzi S. Thyroid disease and the heart. Curr Probl Cardiol. 2016; 41:65–92.15. Lazar MA. Thyroid hormone receptors: multiple forms, multiple possibilities. Endocr Rev. 1993; 14:184–93.16. Hodin RA, Lazar MA, Chin WW. Differential and tissue-specific regulation of the multiple rat c-erbA messenger RNA species by thyroid hormone. J Clin Invest. 1990; 85:101–5.17. Park KW, Dai HB, Ojamaa K, Lowenstein E, Klein I, Sellke FW. The direct vasomotor effect of thyroid hormones on rat skeletal muscle resistance arteries. Anesth Analg. 1997; 85:734–8.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Combination therapy of liothyronine and levothyroxine for hypothyroidism-induced dilated cardiomyopathy
- A Case of Obstructive Sleep Apnea Syndrome Associated with Primary Hypothyroidism and Dilated Cardiomyopathy
- Dilated Cardiomyopathy Secondary to Hypothyroidism: Case Report with a Review of Literatures
- A Case of Hypocalcemia-Induced Dilated Cardiomyopathy
- Two cases of doxorubicin-induced dilated cardiomyopathy
