A case of esophageal perforation caused by suicidal caffeine poisoning in a teenager
- Affiliations
-
- 1Department of Pediatrics, Hanyang University Guri Hospital, Hanyang University College of Medicine, Guri, Republic of Korea
- 2Department of Thoracic and Cardiovascular Surgery, Hanyang University Seoul Hospital, Hanyang University College of Medicine, Seoul, Republic of Korea
- 3Department of Pediatrics, Hanyang University Seoul Hospital, Hanyang University College of Medicine, Seoul, Republic of Korea
- KMID: 2538081
- DOI: http://doi.org/10.22470/pemj.2022.00591
Abstract
- Spontaneous esophageal perforation (also known as Boerhaave syndrome) is associated with sudden increase in intra-esophageal pressure by vomiting, coughing or straining at stool. This case describes a 13-year-old girl who developed the perforation after consuming 270 mg/kg of caffeine tablets for a suicide attempt. Presumably, the perforation was caused primarily by caffeine-induced severe vomiting, and secondarily by caffeine-induced gastric acid secretion with smooth muscle relaxation and by the large amount of caffeine-induced sudden increase in intra-esophageal pressure.
Keyword
Figure
-
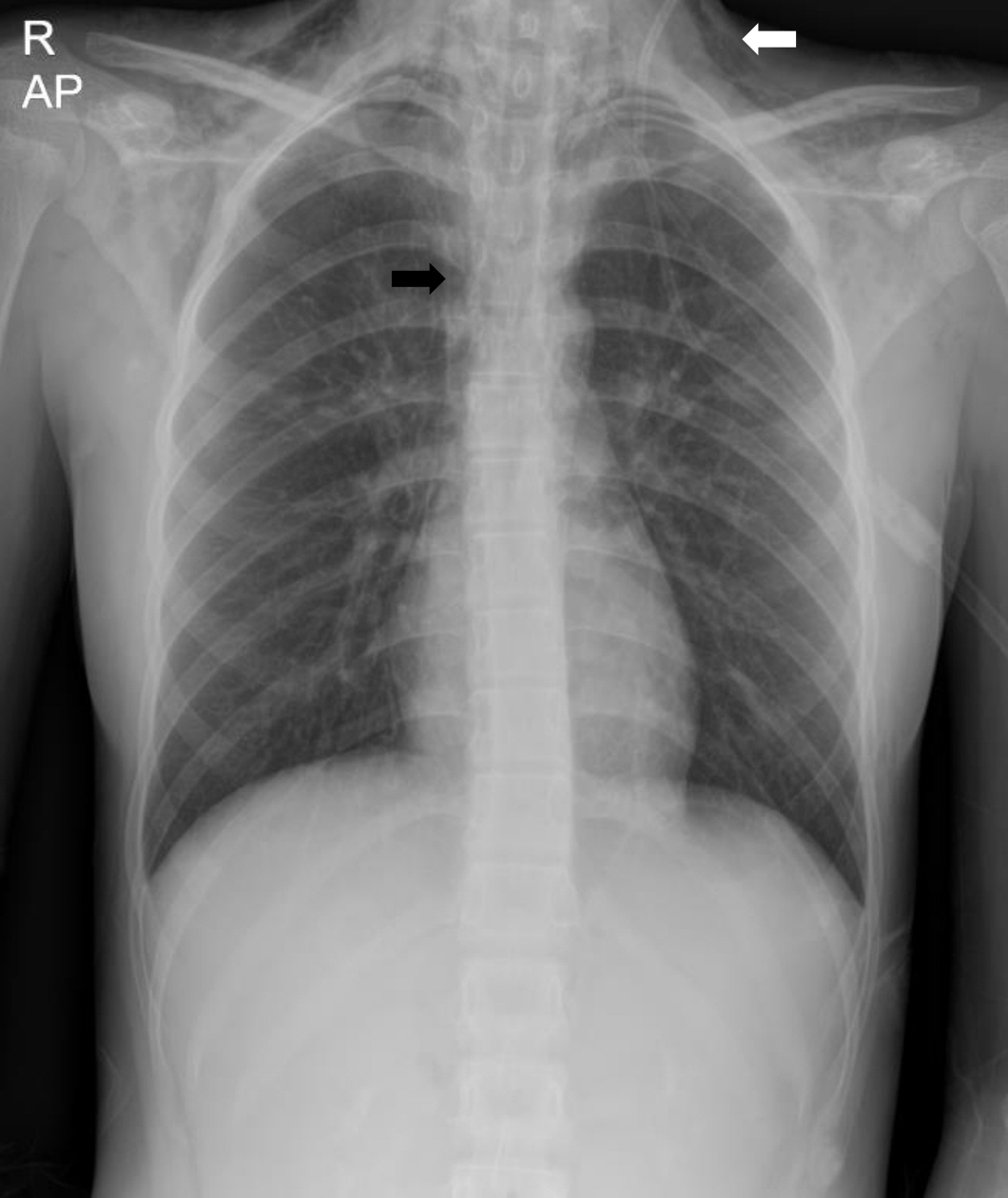
Fig. 1. Initial plain radiograph showing the subcutaneous emphysema (white arrow) in both sides of the lower neck and axillae, and pneumomediastinum (black arrow).
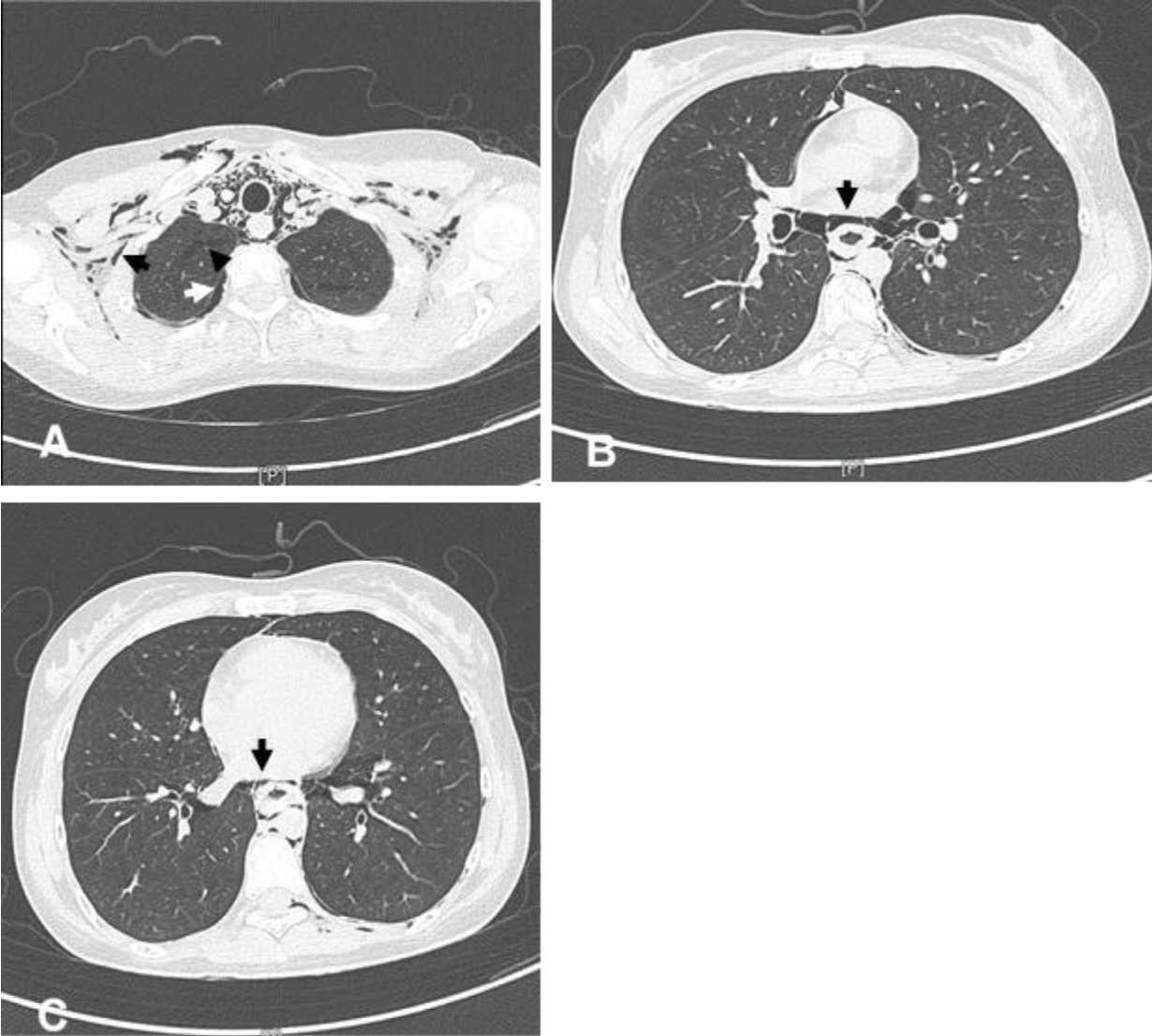
Fig. 2. Computed tomography scan of the chest showing the esophageal rupture, subcutaneous emphysema, and pneumomediastinum (day 1). It shows the scanty pneumothorax (white arrow, A), subcutaneous emphysema in the lower neck, axillae, and chest wall (black arrow, A), interstitial emphysema (arrowhead, A) in both lungs, and extensive pneumomediastinum (arrow, B). Of note, diffuse esophageal wall thickening with suspicious slit-like wall defect (arrow, C) indicates the esophageal rupture.
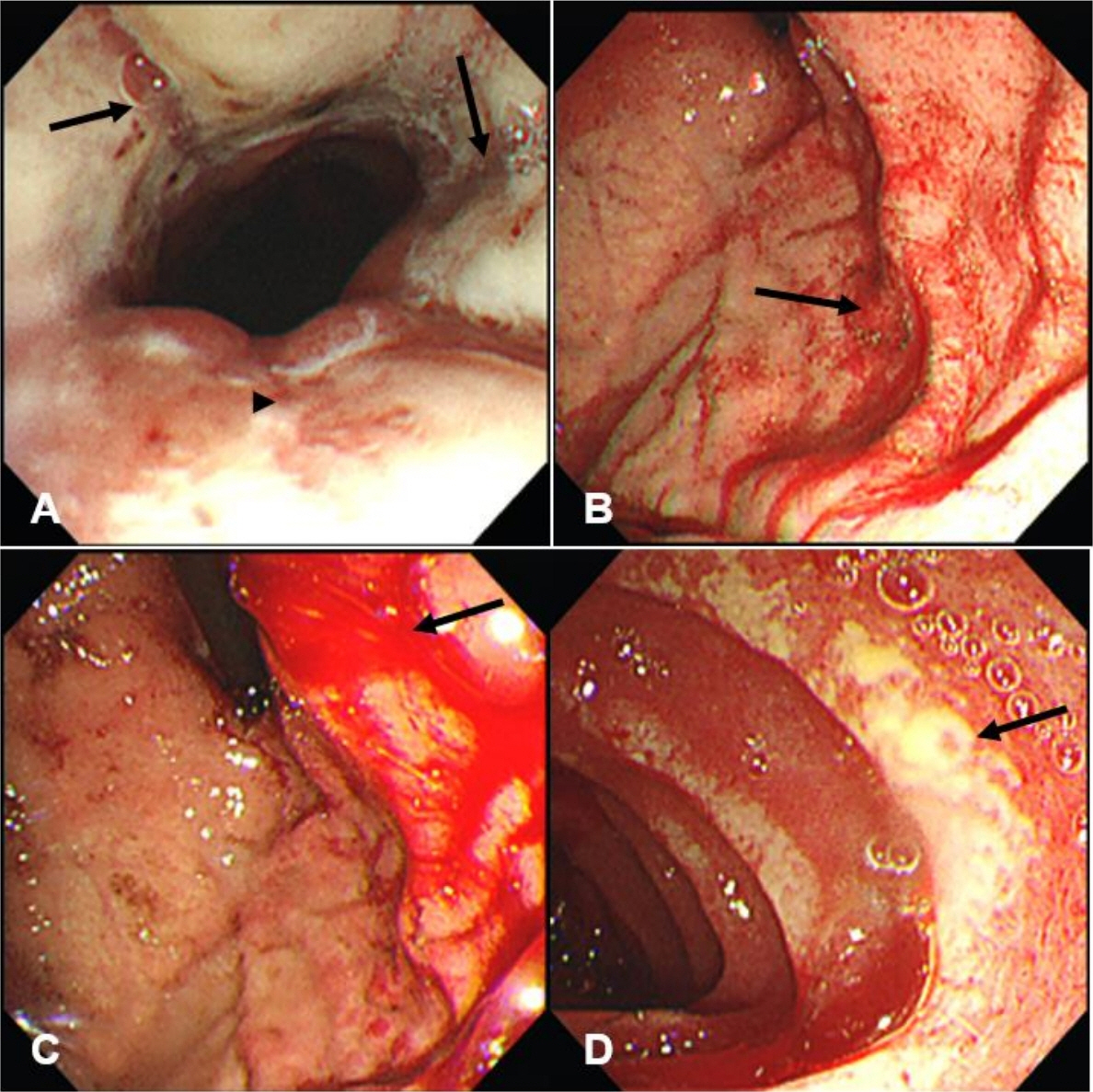
Fig. 3. Upper gastrointestinal endoscopic findings (day 2). Deep longitudinal tears (arrows, A) and ulcers (arrowhead, A) with severe bleeding are noted in the distal esophagus. The cardia shows active superficial ulcers (arrow, B) with current bleeding (arrow, C). Many ulcers are also noted in the first (image of the first portion is not shown) and the second portions of the duodenum. The ulcers are in a circumferential form, and are covered with creamy exudates (arrow, D).
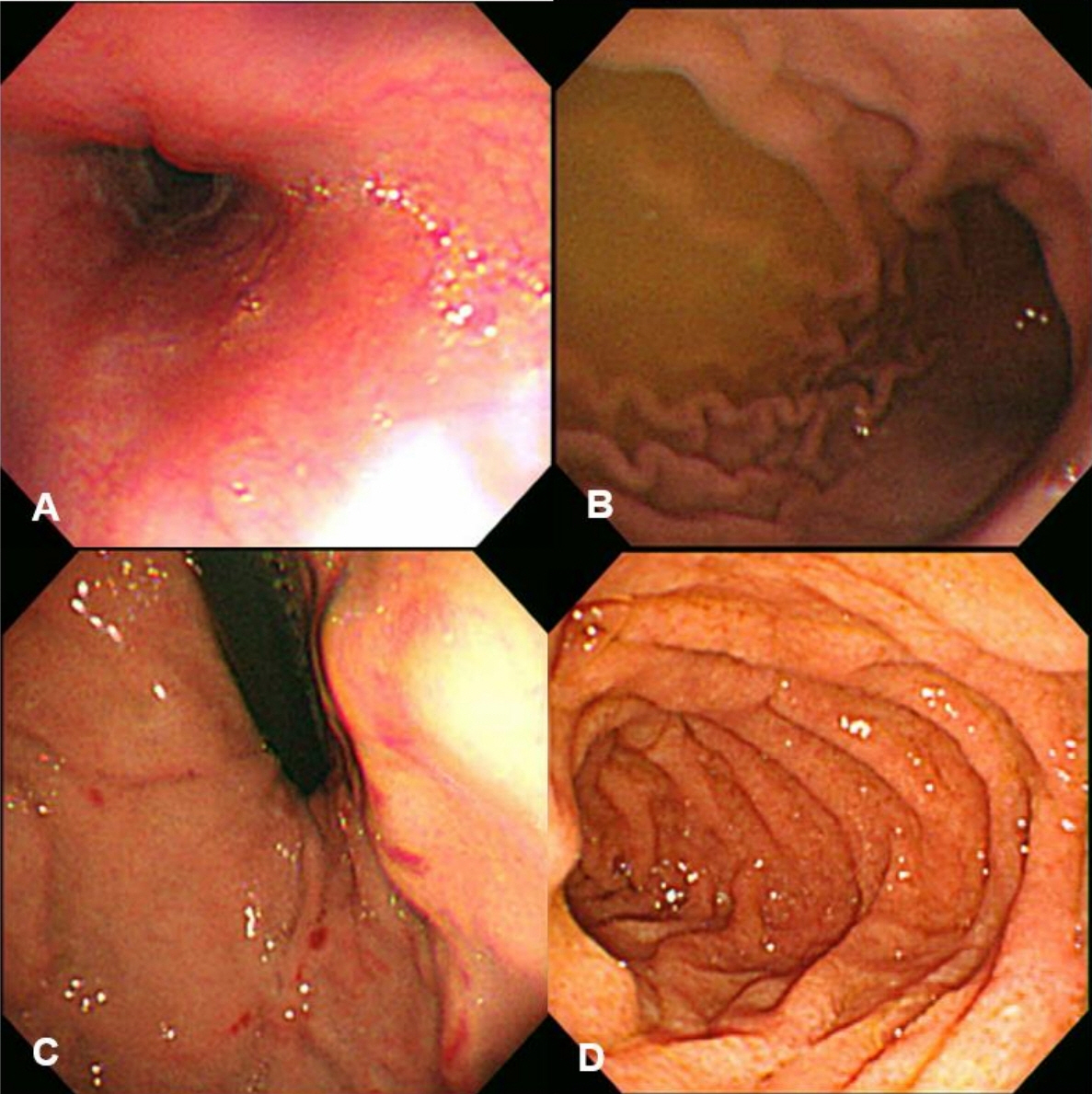
Fig. 4. Follow-up endoscopic findings (day 13). The previous bleeding and ulcers in the distal esophagus are improved with minor focal bleeding and good luminal patency (A). The previous gastric ulcers and hemorrhage are also improved with minor hemorrhagic spots noted in the cardia (B and C). The duodenal circumferential ulcers are in healing status (D).
Reference
-
References
1. Rentea RM, St Peter SD. Neonatal and pediatric esophageal perforation. Semin Pediatr Surg. 2017; 26:87–94.2. Guttman OR, Zachos M. Drug-induced esophageal injury with an occult vascular ring. Paediatr Child Health. 2011; 16:554–6.3. Boyce HW Jr. Drug-induced esophageal damage: diseases of medical progress. Gastrointest Endosc. 1998; 47:547–50.4. Szeremeta M, Sackiewicz A, Drobuliak P, Reszeć-Giełażyn J, Niemcunowicz-Janica A. Rare complications of fatal caffeine intoxication. Forensic Sci. 2022; 2:144–54.5. Lieu MT, Layoun ME, Dai D, Soo Hoo GW, Betancourt J. Tension hydropneumothorax as the initial presentation of Boerhaave syndrome. Respir Med Case Rep. 2018; 25:100–3.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Esophageal Perforation during Endoscopic Variceal Ligation
- The Effects of Caffeine and Aminophylline on co Poisoning Incuced Activity of Mouse
- Thoracoscopic Surgery for Esophageal Perforation and Achalasia: Two cases report
- Iatrogenic esophageal perforation in a newborn: A case report
- Esophageal Perforation Due to Swallowed Toothbrush
