Lobular Carcinoma In Situ during Preoperative Biopsy and the Rate of Upgrade
- Affiliations
-
- 1Department of Surgery, Yonsei University College of Medicine, Seoul, Korea
- 2Department of Pathology, Yonsei University College of Medicine, Seoul, Korea
- KMID: 2534186
- DOI: http://doi.org/10.4143/crt.2021.864
Abstract
- Purpose
There is a potential risk that lobular carcinoma in situ (LCIS) on preoperative biopsy might be diagnosed as ductal carcinoma in situ (DCIS) or invasive carcinoma in the final pathology. This study aimed to evaluate the rate of upgrade of LCIS on preoperative biopsy to DCIS or invasive carcinoma.
Materials and Methods
Data of 55 patients with LCIS on preoperative biopsy were analyzed. All patients underwent surgery between 1991 and 2016 at Severance Hospital in Seoul, Korea. We analyzed the rate of upgrade of preoperative LCIS to DCIS or invasive cancer in the final pathology. The clinicopathologic features related to the upgrade were evaluated.
Results
The rate of upgrade of LCIS to DCIS or invasive carcinoma was 16.4% (9/55). In multivariate analysis, microcalcification and progesterone receptor expression were significantly associated with the upgrade of LCIS (p=0.023 and p=0.044, respectively).
Conclusion
The current study showed a relatively high rate of upgrade of LCIS on preoperative biopsy to DCIS or invasive cancer. The presence of microcalcification and progesterone receptor expression may be potential predictors of upgradation of LCIS on preoperative biopsy. Surgical excision of the LCIS during preoperative biopsy could be a management option to identify the concealed malignancy.
Keyword
Figure
-
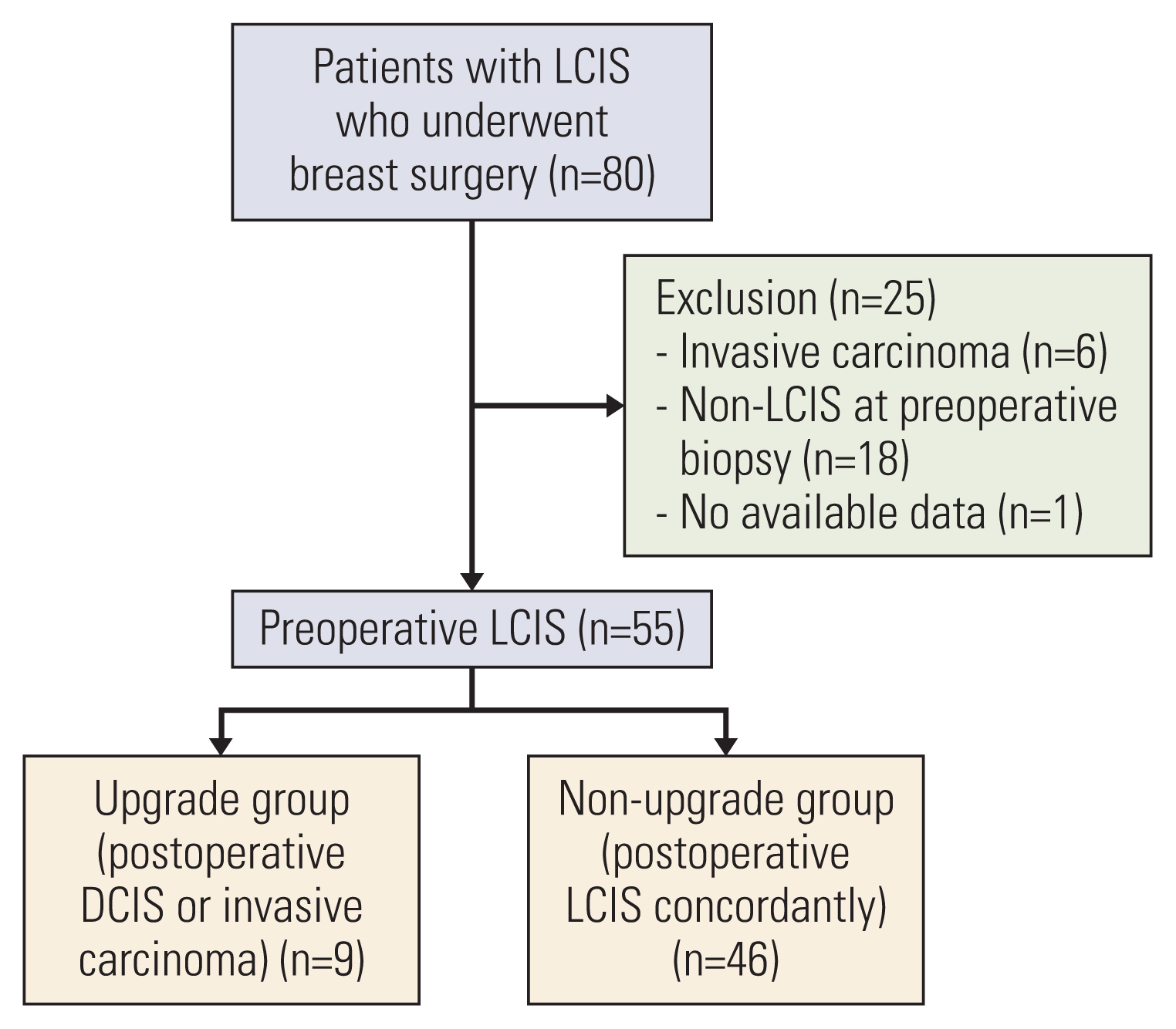
Fig. 1 Schema of the study design to analyze the upgrade rate of preoperative LCIS. DCIS, ductal carcinoma in situ; LCIS, lobular carcinoma in situ.
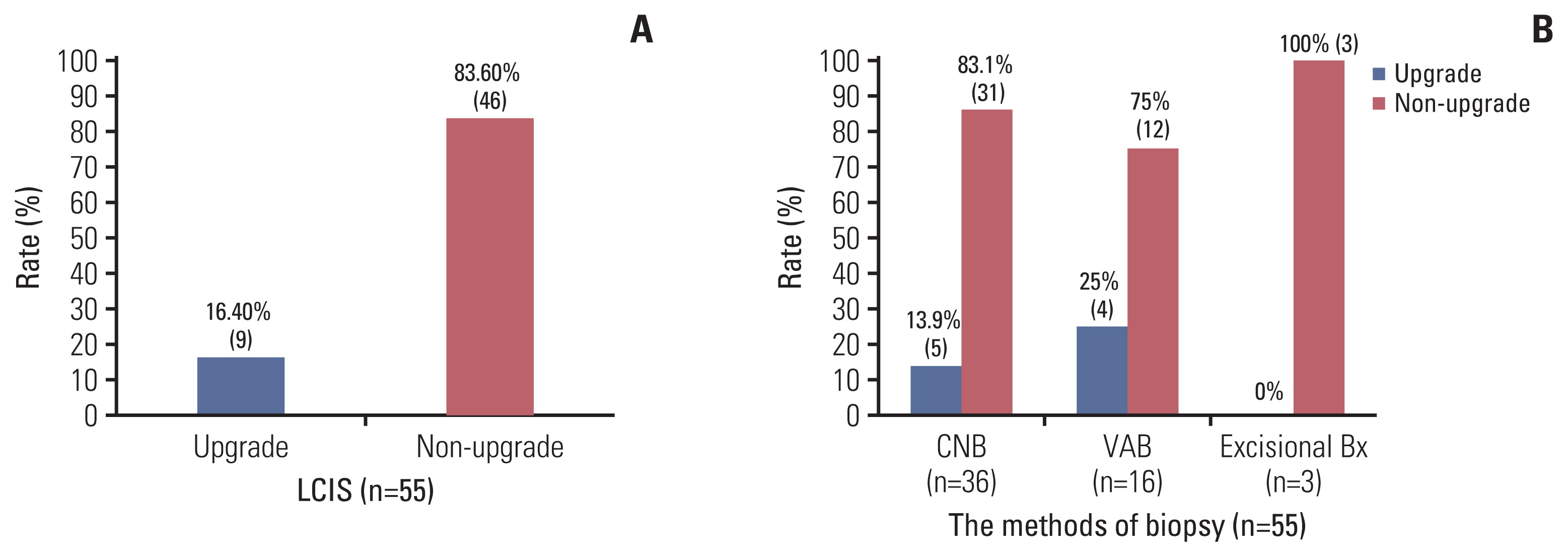
Fig. 2 The rate of upgrade of preoperative LCIS. (n=55). (A) The rate of upgrade of preoperative LCIS. (B) The rate of upgrade of preoperative LCIS according to the methods of preoperative biopsy. Bx, biopsy; CNB, core needle biopsy; LCIS, lobular carcinoma in situ; VAB, vacuum assisted biopsy.
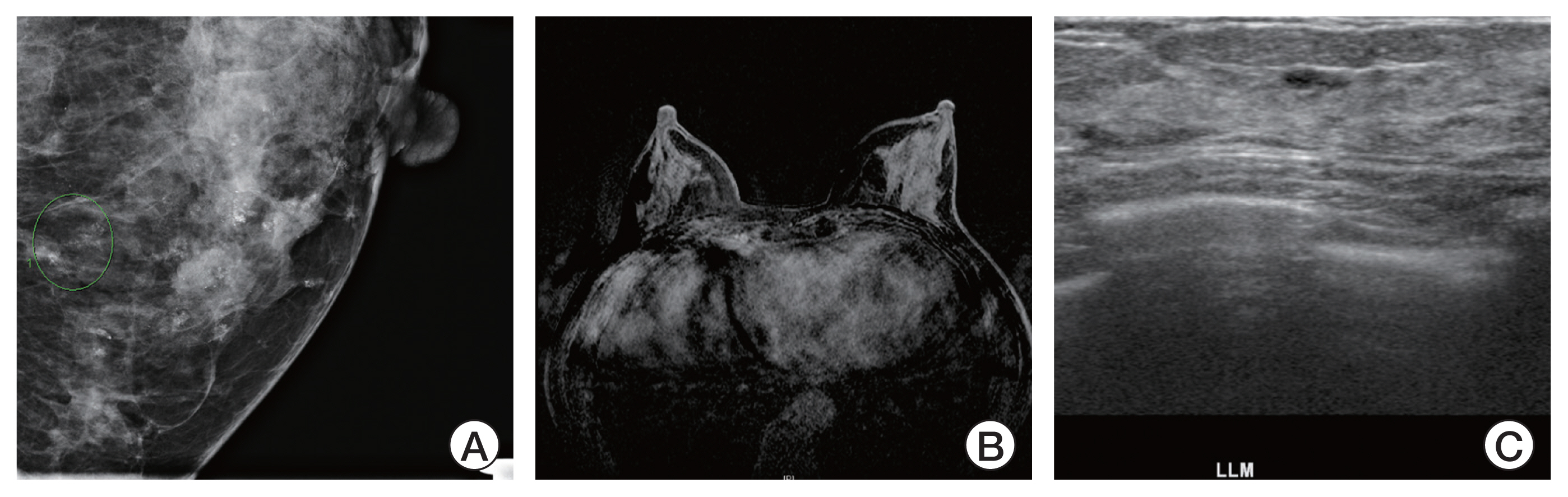
Fig. 3 A case of the upgrade group with definite microcalcification on mammography without USG and MRI findings and the PR positivity. (A) Increased extent and amount of grouped microcalcification in lower central portion of the left breast on mammography. (B) Multiple probable benign enhancement without localized suspicious enhancements in both breasts on MRI. (C) Increased benign looking lesions in the both breasts on USG. MRI, magnetic resonance imaging; PR, progesterone receptor; USG, ultrasonography.
Reference
-
References
1. Bevers TB, Helvie M, Bonaccio E, Calhoun KE, Daly MB, Farrar WB, et al. NCCN clinical practice guidelines in oncology (NCCN Guidelines): breast cancer screening and diagnosis. Plymouth Meeting, PA: National Comprehensive Cancer Network;2019.2. Middleton LP, Grant S, Stephens T, Stelling CB, Sneige N, Sahin AA. Lobular carcinoma in situ diagnosed by core needle biopsy: when should it be excised? Mod Pathol. 2003; 16:120–9.3. Shah-Khan MG, Geiger XJ, Reynolds C, Jakub JW, Deperi ER, Glazebrook KN. Long-term follow-up of lobular neoplasia (atypical lobular hyperplasia/lobular carcinoma in situ) diagnosed on core needle biopsy. Ann Surg Oncol. 2012; 19:3131–8.4. Giuliano AE, Connolly JL, Edge SB, Mittendorf EA, Rugo HS, Solin LJ, et al. Breast cancer-major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin. 2017; 67:290–303.5. Sen LQ, Berg WA, Hooley RJ, Carter GJ, Desouki MM, Sumkin JH. Core breast biopsies showing lobular carcinoma in situ should be excised and surveillance is reasonable for atypical lobular hyperplasia. AJR Am J Roentgenol. 2016; 207:1132–45.6. Park HS, Kim HY, Park S, Kim EK, Kim SI, Park BW. A nomogram for predicting underestimation of invasiveness in ductal carcinoma in situ diagnosed by preoperative needle biopsy. Breast. 2013; 22:869–73.7. Li CI, Malone KE, Saltzman BS, Daling JR. Risk of invasive breast carcinoma among women diagnosed with ductal carcinoma in situ and lobular carcinoma in situ, 1988–2001. Cancer. 2006; 106:2104–12.8. Cheng P, Huang Q, Shou J, Hu G, Han M, Huang J. Treatment and survival outcomes of lobular carcinoma in situ of the breast: a SEER population based study. Oncotarget. 2017; 8:103047–54.9. Schmidt H, Arditi B, Wooster M, Weltz C, Margolies L, Bleiweiss I, et al. Observation versus excision of lobular neoplasia on core needle biopsy of the breast. Breast Cancer Res Treat. 2018; 168:649–54.10. Wen HY, Brogi E. Lobular carcinoma in situ. Surg Pathol Clin. 2018; 11:123–45.11. Foschini MP, Miglio R, Fiore R, Baldovini C, Castellano I, Callagy G, et al. Pre-operative management of pleomorphic and florid lobular carcinoma in situ of the breast: report of a large multi-institutional series and review of the literature. Eur J Surg Oncol. 2019; 45:2279–86.12. Calhoun BC, Collins LC. Recommendations for excision following core needle biopsy of the breast: a contemporary evaluation of the literature. Histopathology. 2016; 68:138–51.13. Khoury T, Kumar PR, Li Z, Karabakhtsian RG, Sanati S, Chen X, et al. Lobular neoplasia detected in MRI-guided core biopsy carries a high risk for upgrade: a study of 63 cases from four different institutions. Mod Pathol. 2016; 29:25–33.14. Desai AA, Jimenez RE, Hoskin TL, Day CN, Boughey JC, Hieken TJ. Treatment outcomes for pleomorphic lobular carcinoma in situ of the breast. Ann Surg Oncol. 2018; 25:3064–8.15. Genco IS, Tugertimur B, Chang Q, Cassell L, Hajiyeva S. Outcomes of classic lobular neoplasia diagnosed on breast core needle biopsy: a retrospective multi-center study. Virchows Arch. 2020; 476:209–17.16. Holbrook AI, Hanley K, Jeffers C, Kang J, Cohen MA. Triaging atypical lobular hyperplasia and lobular carcinoma in situ on percutaneous core biopsy to surgery or observation: assiduous radiologic-pathologic correlation works, quantitating extent of disease does not. Arch Pathol Lab Med. 2019; 143:621–7.17. Nakhlis F, Harrison BT, Giess CS, Lester SC, Hughes KS, Coopey SB, et al. Evaluating the rate of upgrade to invasive breast cancer and/or ductal carcinoma in situ following a core biopsy diagnosis of non-classic lobular carcinoma in situ. Ann Surg Oncol. 2019; 26:55–61.18. Youk JH, Kim EK, Kim MJ, Ko KH, Kwak JY, Son EJ, et al. Concordant or discordant? Imaging-pathology correlation in a sonography-guided core needle biopsy of a breast lesion. Korean J Radiol. 2011; 12:232–40.19. Cangiarella J, Guth A, Axelrod D, Darvishian F, Singh B, Simsir A, et al. Is surgical excision necessary for the management of atypical lobular hyperplasia and lobular carcinoma in situ diagnosed on core needle biopsy?: a report of 38 cases and review of the literature. Arch Pathol Lab Med. 2008; 132:979–83.20. Bowman K, Munoz A, Mahvi DM, Breslin TM. Lobular neoplasia diagnosed at core biopsy does not mandate surgical excision. J Surg Res. 2007; 142:275–80.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Invasive Lobular Carcinoma of the Breast Associated with Mixed Lobular and Ductal Carcinoma In Situ: A Case Report
- Lobular carcinoma in situ in sclerosing adenosis
- Multi-Focal Lobular Carcinoma In Situ Arising in Benign Phyllodes Tumor: A Case Report
- Atypical Ductal Hyperplasia: Risk Factors for Predicting Pathologic Upgrade on Excisional Biopsy
- Borderline Phyllodes Tumor with an Incidental Invasive Tubular Carcinoma and Lobular Carcinoma In Situ Component: A Case Report
