A Phase I/IIa Randomized Trial Evaluating the Safety and Efficacy of SNK01 Plus Pembrolizumab in Patients with Stage IV Non-Small Cell Lung Cancer
- Kim EJ
 1,2
1,2 - Cho YH3,4
- Kim DH3
- Ko DH5
- Do EJ3
- Kim SY6
- Kim YM7
- Jung JS7
- Kang Y7
- Ji W8
- Choi MG8
- Lee JC1
- Rho JK6
- Choi CM1,8
- Affiliations
-
- 1Department of Oncology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 2Division of Hematology/Oncology, Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea
- 3Asan Institute for Life Sciences, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 4Data Convergence Drug Research Center, Therapeutics and Biotechnology Division, Korea Research Institute of Chemical Technology (KRICT), Daejeon, Korea
- 5Department of Laboratory Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 6Department of Convergence Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 7NKMAX Co., Ltd., Seongnam, Korea
- 8Department of Pulmonology and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2534180
- DOI: http://doi.org/10.4143/crt.2021.986
Abstract
- Purpose
The aim of this study is to evaluate the safety and efficacy of ex vivo activated and expanded natural killer (NK) cell therapy (SNK01) plus pembrolizumab in a randomized phase I/IIa clinical trial.
Materials and Methods
Overall, 18 patients with advanced non–small cell lung cancer (NSCLC) and a programmed death ligand 1 tumor proportion score of 1% or greater who had a history of failed frontline platinum-based therapy were randomized (2:1) to receive pembrolizumab every 3 weeks +/– 6 weekly infusions of SNK01 at either 2×109 or 4×109 cells per infusion (pembrolizumab monotherapy vs. SNK01 combination). The primary endpoint was safety, whereas the secondary endpoints were the objective response rate (ORR), progression-free survival (PFS), overall survival, and quality of life.
Results
Since no dose-limiting toxicity was observed, the maximum tolerated dose was determined as SNK01 4×109 cells/dose. The safety data did not show any new safety signals when SNK01 was combined with pembrolizumab. The ORR and the 1-year survival rate in the NK combination group were higher than those in patients who underwent pembrolizumab monotherapy (ORR, 41.7% vs. 0%; 1-year survival rate, 66.7% vs. 50.0%). Furthermore, the median PFS was higher in the SNK01 combination group (6.2 months vs. 1.6 months, p=0.001).
Conclusion
Based on the findings of this study, the NK cell combination therapy may consider as a safe treatment method for stage IV NSCLC patients who had a history of failed platinum-based therapy without an increase in adverse events.
Figure
-
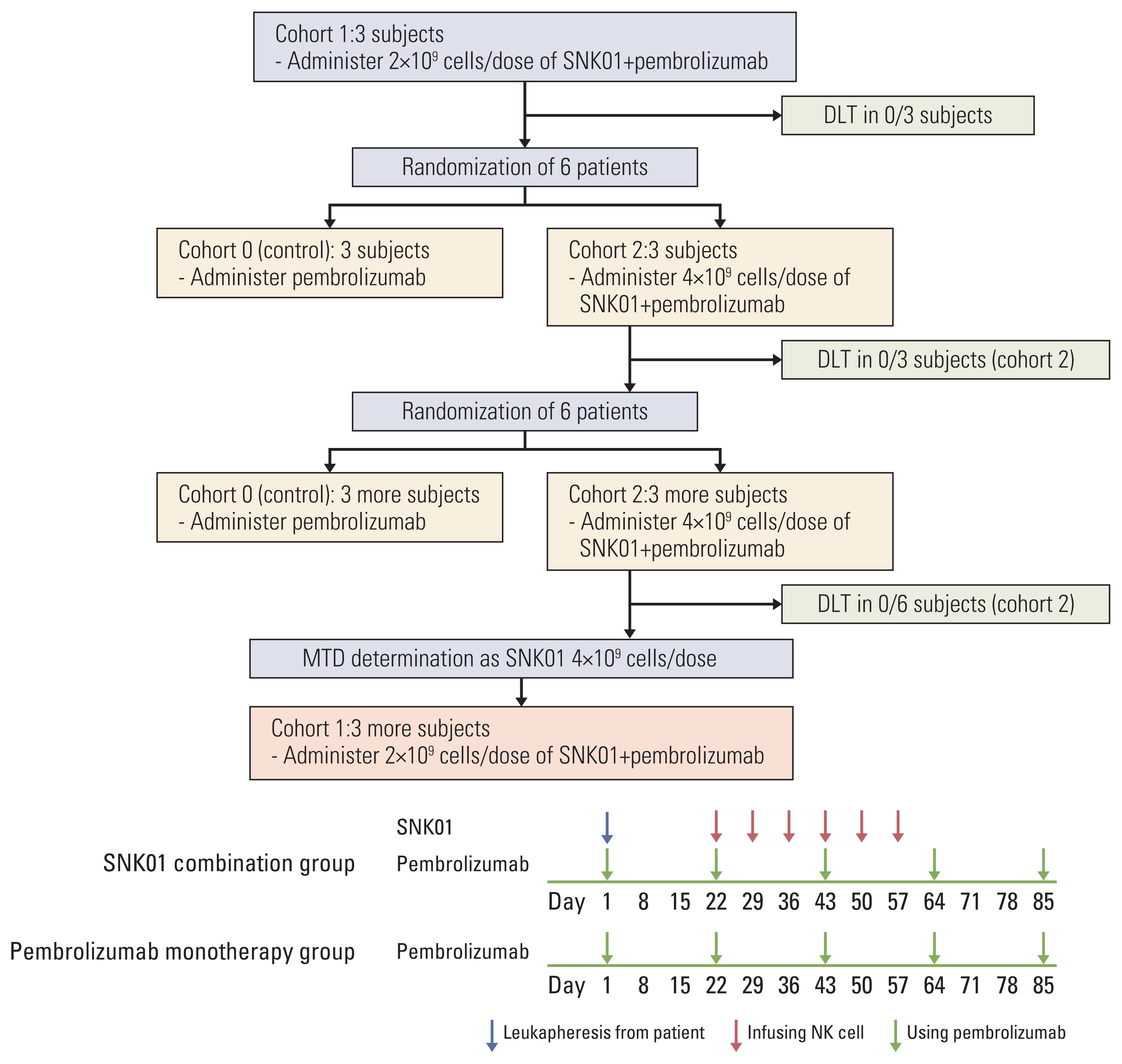
Fig. 1 Clinical trial profile. In total, 20 patients were enrolled to the trial. Except for the first three and the last three patients (cohort 1), the remaining patients were randomly assigned to cohort 0 or 2. The pembrolizumab monotherapy group (cohort 0) received regular therapy with intravenous injection of pembrolizumab (200 mg) on the indicated time. The pembrolizumab plus SNK01 group (cohort 1 or 2) received pembrolizumab plus a total of 6 SNK01 infusions in 42 days, i.e., weekly infusion for 6 weeks. DLT, dose-limiting toxicity; MTD, maximum tolerated dose; NK, natural killer.
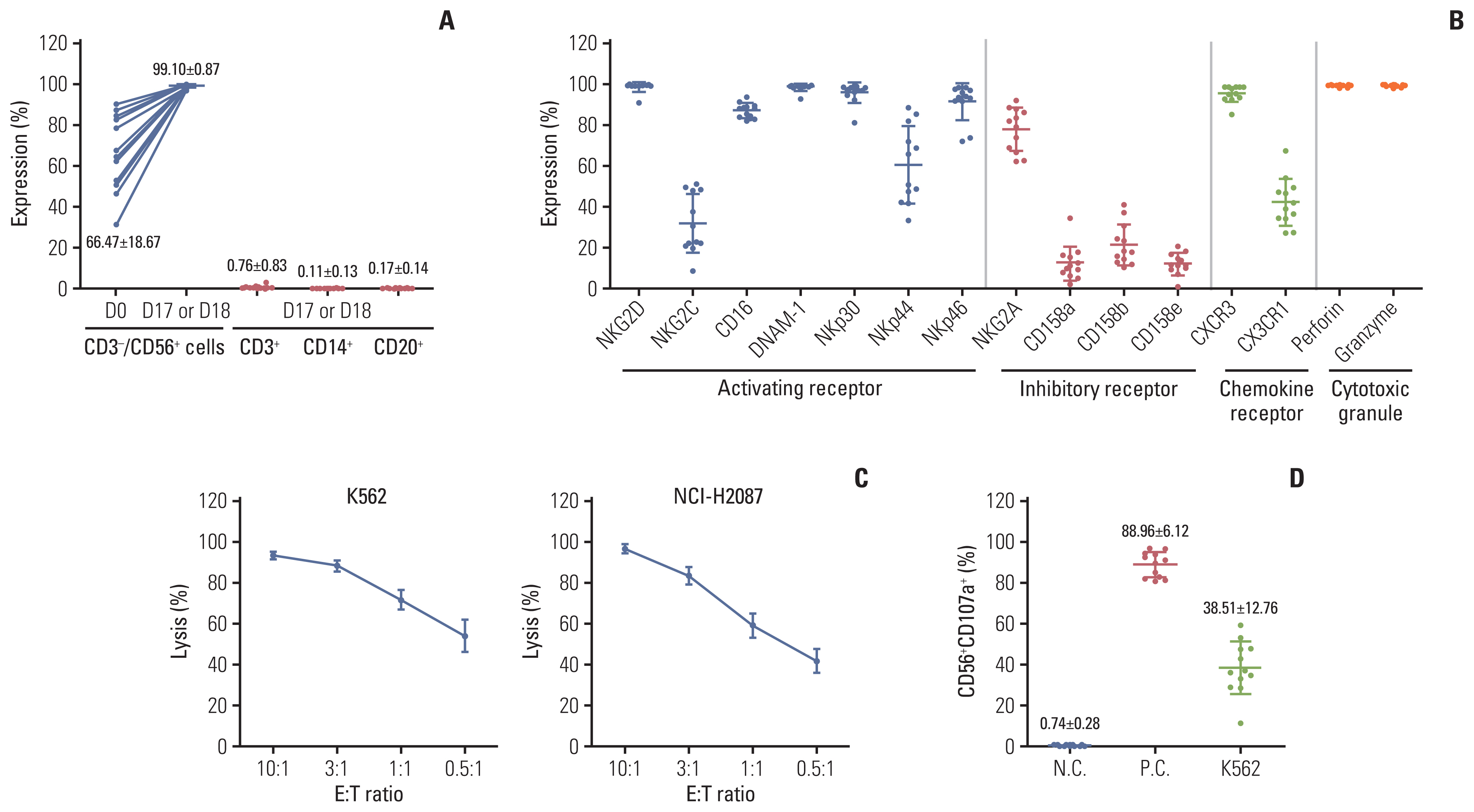
Fig. 2 Characteristics of expanded NK cells. (A) The percentages of CD3−CD56+ NK cells, CD3+ T cells, CD20+ B cells, and CD14+ monocytes were analyzed flow cytometrically on freshly isolated positive cells using CliniMACS CD56 microbeads (D0; before expansion) and expanded NK cells for 17–18 days of culture (D17–18). (B) The fold expansion of the total cell population after 17–18 days of culture (D17–18). The expression levels of activating receptors, inhibitory receptors, chemokine receptors, perforin, and granzyme B were analyzed flow cytometrically among CD56+ gated cells after 17–18 days of culture. (C) The cytotoxic activity of expanded NK cells against the K562 and NCI-H2087 cell lines was measured via calcein-release assay at E:T ratios of 10:1 to 0.5:1 in triplicate. (D) The NK cell degranulation activity was measured flow cytometrically with % of CD56+CD107a+ in coincubation with K562 cells (E:T ratio=1:1), with phorbol 12-myristate 13-acetate/ionomycin treatment (as positive control, P.C.), or without treatment (negative control, N.C.). Dots represent the mean value of each patient from 5 to 6 cultures for clinical trial. Horizontal bars indicate the mean value, and each point represents mean±standard deviation. NK, natural killer.
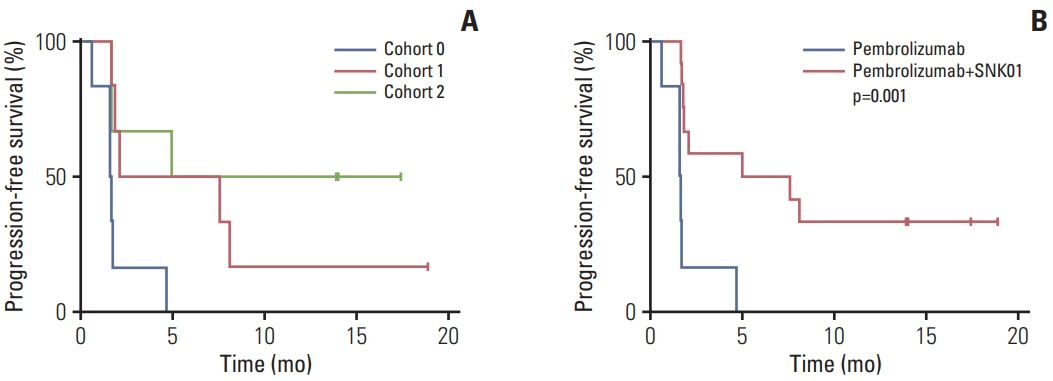
Fig. 3 Progression-free survival analysis. Kaplan-Meier analysis was used to estimate the progression-free survival of each cohort (A) or group patients who received natural killer cell infusion (B).
Reference
-
References
1. Molina JR, Yang P, Cassivi SD, Schild SE, Adjei AA. Non-small cell lung cancer: epidemiology, risk factors, treatment, and survivorship. Mayo Clin Proc. 2008; 83:584–94.2. Cosaert J, Quoix E. Platinum drugs in the treatment of non-small-cell lung cancer. Br J Cancer. 2002; 87:825–33.3. Tiseo M, Boni L, Ardizzoni A. Platinum-based versus non-platinum-based chemotherapy in advanced non-small-cell lung cancer: does cisplatin versus carboplatin make a difference? J Clin Oncol. 2005; 23:6276–7.4. Grupp SA, Kalos M, Barrett D, Aplenc R, Porter DL, Rheingold SR, et al. Chimeric antigen receptor-modified T cells for acute lymphoid leukemia. N Engl J Med. 2013; 368:1509–18.5. Hui R, Garon EB, Goldman JW, Leighl NB, Hellmann MD, Patnaik A, et al. Pembrolizumab as first-line therapy for patients with PD-L1-positive advanced non-small cell lung cancer: a phase 1 trial. Ann Oncol. 2017; 28:874–81.6. Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012; 12:252–64.7. Rizzo A, Ricci AD, Brandi G. PD-L1, TMB, MSI, and other predictors of response to immune checkpoint inhibitors in biliary tract cancer. Cancers (Basel). 2021; 13:558.8. Yarchoan M, Albacker LA, Hopkins AC, Montesion M, Murugesan K, Vithayathil TT, et al. PD-L1 expression and tumor mutational burden are independent biomarkers in most cancers. JCI Insight. 2019; 4:e126908.9. Marcus L, Lemery SJ, Keegan P, Pazdur R. FDA approval summary: pembrolizumab for the treatment of microsatellite instability-high solid tumors. Clin Cancer Res. 2019; 25:3753–8.10. Reck M, Rodriguez-Abreu D, Robinson AG, Hui R, Csoszi T, Fulop A, et al. Updated analysis of KEYNOTE-024: pembrolizumab versus platinum-based chemotherapy for advanced non-small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J Clin Oncol. 2019; 37:537–46.11. Chowdhury PS, Chamoto K, Honjo T. Combination therapy strategies for improving PD-1 blockade efficacy: a new era in cancer immunotherapy. J Intern Med. 2018; 283:110–20.12. Schmidt C. The benefits of immunotherapy combinations. Nature. 2017; 552:S67–9.13. Liu S, Galat V, Galat Y, Lee YKA, Wainwright D, Wu J. NK cell-based cancer immunotherapy: from basic biology to clinical development. J Hematol Oncol. 2021; 14:7.14. Wu SY, Fu T, Jiang YZ, Shao ZM. Natural killer cells in cancer biology and therapy. Mol Cancer. 2020; 19:120.15. Cichocki F, Bjordahl R, Gaidarova S, Mahmood S, Abujarour R, Wang H, et al. iPSC-derived NK cells maintain high cytotoxicity and enhance in vivo tumor control in concert with T cells and anti-PD-1 therapy. Sci Transl Med. 2020; 12:eaaz5618.16. Hsu J, Hodgins JJ, Marathe M, Nicolai CJ, Bourgeois-Daigneault MC, Trevino TN, et al. Contribution of NK cells to immunotherapy mediated by PD-1/PD-L1 blockade. J Clin Invest. 2018; 128:4654–68.17. Lin M, Luo H, Liang S, Chen J, Liu A, Niu L, et al. Pembrolizumab plus allogeneic NK cells in advanced non-small cell lung cancer patients. J Clin Invest. 2020; 130:2560–9.18. Dong W, Wu X, Ma S, Wang Y, Nalin AP, Zhu Z, et al. The mechanism of anti-PD-L1 antibody efficacy against PD-L1-negative tumors identifies NK cells expressing PD-L1 as a cytolytic effector. Cancer Discov. 2019; 9:1422–37.19. Pesce S, Greppi M, Grossi F, Del Zotto G, Moretta L, Sivori S, et al. PD/1-PD-Ls checkpoint: insight on the potential role of NK cells. Front Immunol. 2019; 10:1242.20. Lim SA, Kim TJ, Lee JE, Sonn CH, Kim K, Kim J, et al. Ex vivo expansion of highly cytotoxic human NK cells by cocultivation with irradiated tumor cells for adoptive immunotherapy. Cancer Res. 2013; 73:2598–607.21. Huang Z, Su W, Lu T, Wang Y, Dong Y, Qin Y, et al. First-line immune-checkpoint inhibitors in non-small cell lung cancer: current landscape and future progress. Front Pharmacol. 2020; 11:578091.22. Sui H, Ma N, Wang Y, Li H, Liu X, Su Y, et al. Anti-PD-1/PD-L1 therapy for non-small-cell lung cancer: toward personalized medicine and combination strategies. J Immunol Res. 2018; 2018:6984948.23. Herbst RS, Baas P, Kim DW, Felip E, Perez-Gracia JL, Han JY, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet. 2016; 387:1540–50.24. Gandhi L, Rodriguez-Abreu D, Gadgeel S, Esteban E, Felip E, De Angelis F, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018; 378:2078–92.25. Paul S, Lal G. The molecular mechanism of natural killer cells function and its importance in cancer immunotherapy. Front Immunol. 2017; 8:1124.26. Hu W, Wang G, Huang D, Sui M, Xu Y. Cancer immunotherapy based on natural killer cells: current progress and new opportunities. Front Immunol. 2019; 10:1205.27. Parkhurst MR, Riley JP, Dudley ME, Rosenberg SA. Adoptive transfer of autologous natural killer cells leads to high levels of circulating natural killer cells but does not mediate tumor regression. Clin Cancer Res. 2011; 17:6287–97.28. Shin MH, Kim J, Lim SA, Kim J, Kim SJ, Lee KM. NK cell-based immunotherapies in cancer. Immune Netw. 2020; 20:e14.29. Choi MG, Kim YJ, Lee JC, Rho JK, Choi CM. Efficacy of natural killer cell activity as a biomarker for predicting immunotherapy response in non-small cell lung cancer. Thorac Cancer. 2020; 11:3337–45.30. Tang SQ, Tang LL, Mao YP, Li WF, Chen L, Zhang Y, et al. The pattern of time to onset and resolution of immune-related adverse events caused by immune checkpoint inhibitors in cancer: a pooled analysis of 23 clinical trials and 8,436 patients. Cancer Res Treat. 2021; 53:339–54.31. Das S, Johnson DB. Immune-related adverse events and anti-tumor efficacy of immune checkpoint inhibitors. J Immunother Cancer. 2019; 7:306.32. Naing A, Hajjar J, Gulley JL, Atkins MB, Ciliberto G, Meric-Bernstam F, et al. Strategies for improving the management of immune-related adverse events. J Immunother Cancer. 2020; 8:e001754.33. Wong HH, Halford S. Dose-limiting toxicity and maximum tolerated dose: still fit for purpose? Lancet Oncol. 2015; 16:1287–8.34. Yang YJ, Park JC, Kim HK, Kang JH, Park SY. A trial of autologous ex vivo-expanded NK cell-enriched lymphocytes with docetaxel in patients with advanced non-small cell lung cancer as second- or third-line treatment: phase IIa study. Anticancer Res. 2013; 33:2115–22.35. Hastings K, Yu HA, Wei W, Sanchez-Vega F, DeVeaux M, Choi J, et al. EGFR mutation subtypes and response to immune checkpoint blockade treatment in non-small-cell lung cancer. Ann Oncol. 2019; 30:1311–20.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Etoposide and cisplatin combination chemotherapy in extensive stage small cell lung cancer
- Efficacy of Combination Chemotherapy with Vinorelbine, Ifosfamide, and Cisplatin in Patients with Advanced Non-Small Cell Lung Cancer
- Clinical Efficacy of Immune Checkpoint Inhibitors in Non–Small Cell Lung Cancer Patients with Liver Metastases: A Network Meta-Analysis of Nine Randomized Controlled Trials
- Adjuvant Pembrolizumab in Patients with Stage IIIA/N2 Non–Small Cell Lung Cancer Completely Resected after Neoadjuvant Concurrent Chemoradiation: A Prospective, Open-Label, Single-Arm, Phase 2 Trial
- Clinical Outcomes after Upfront Surgery in Clinical Stage I–IIA Small Cell Lung Cancer
