Deconstructive repair of a traumatic vertebrovertebral arteriovenous fistula via a contralateral endovascular approach
- Affiliations
-
- 1Department of Neurology, Mount Sinai Hospital, New York City, NY, USA
- 2Department of Radiology, Division of Neuroradiology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA
- 3Department of Neurosurgery, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA
- 4Department of Neurology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA
- KMID: 2533682
- DOI: http://doi.org/10.7461/jcen.2022.E2021.10.002
Abstract
- Vertebrovertebral arteriovenous fistulas (VVAVFs) are rare entities that lack consensus guidelines for their management. Our case describes the successful treatment of a traumatic VVAVF via a contralateral deconstructive endovascular approach. A 64-year-old female presented following a traumatic fall. Computed tomography angiogram highlighted a 2 cm pseudoaneurysm of the right vertebral artery (VA) with epidural contrast enhancement and a hematoma with flow voids within the epidural space. Digital subtraction angiography showed a VVAVF at C2-3 with retrograde filling of the distal right VA. Having undergone several unsuccessful passes of the proximal dissection flap in the right VA, the patient underwent a contralateral deconstructive approach with correction of the VVAVF without complication. The remaining feeding branches had occluded after 1 week. The patient made a complete recovery without neurological sequelae at 3-month follow-up.
Figure
-
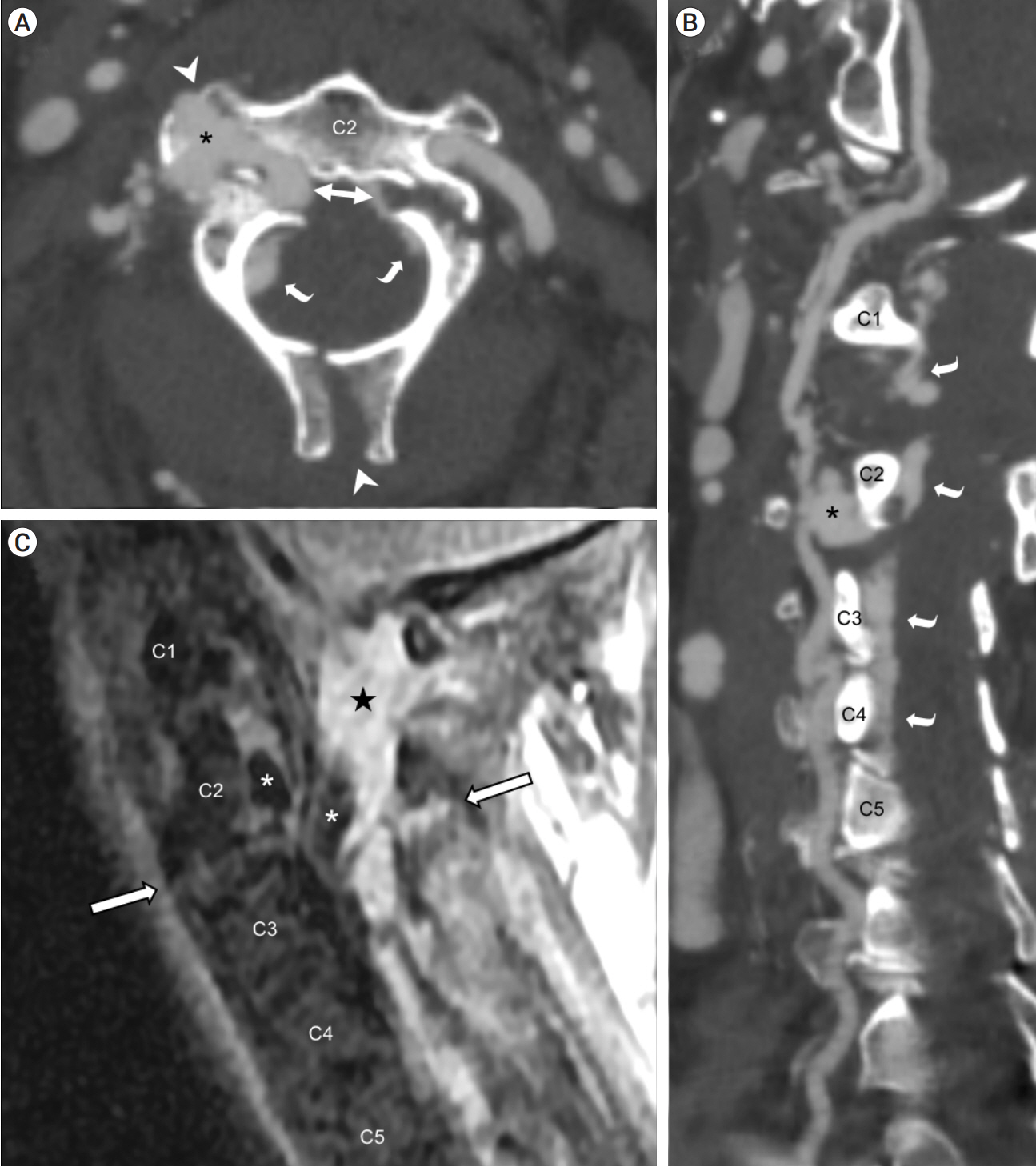
Fig. 1. Non-invasive preoperative imaging. CT angiography of the neck in axial plane (A) and curved planar reformation along the right cervical vertebral artery (B) showed an asymmetrical fracture at the right pedicle and left pars interarticularis of C2 (bidirectional arrow), with extension to the right transverse process and spinous process (white arrowheads); right vertebral artery pseudoaneurysm insinuating into fracture lines (asterisk); and prominent epidural contrast enhancement (curved arrows). MRI of the cervical spine on a right parasagittal short TI inversion recovery (STIR) image (C) showed prevertebral and paraspinal fluid, discoligamentous complex injury through the C2-3 intervertebral level (outlined arrows), circumferential epidural hematoma (star), and flow voids in the pseudoaneurysm extending into the epidural space (asterisks). CT, computed tomography; MRI, magnetic resonance imaging

Fig. 2. Catheter angiography before (A-C) and after (D-F) endovascular treatment and spinal fixation. Right vertebral artery injection in right anterior oblique (A) and lateral (B) projections showed pseudoaneurysmal outpouching (arrowhead) surrounding the distal V2 (intraforaminal) segment, no distal arterial opacification, and early filling of the engorged internal vertebral venous plexus and other venous structures cranial and caudal to the level of injury (curved arrows), indicating a vertebrovertebral arteriovenous fistula (VVAVF). Left vertebral artery injection in the anteroposterior projection (C) showed retrograde filling of the distal right vertebral artery and the VVAVF (curved arrows). Follow-up angiogram after coil embolization of the pseudoaneurysm and fistulous connection showed no filling of the entire right vertebral artery on right subclavian artery injection (D, subtracted image; E, unsubtracted image showing coils [outlined arrow] and spinal hardware) and on left vertebral artery injection (F). No early venous filling was shown to suggest residual fistula.
Reference
-
1. Aljobeh A, Sorenson TJ, Bortolotti C, Cloft H, Lanzino G. Vertebral arteriovenous fistula: a review article. World Neurosurg. 2019; Feb. 122:e1388–97.
Article2. Berenstein A, Lasjaunias P, ter Brugge KG. Vertebro-vertebral arteriovenous fistulae. In : Berenstein A, Lasjaunias P, Brugge KG, editors. Surgical Neuroangiography. New York: Springer-Verlag;2004. p. 743–51.3. Groen RJ, Groenewegen HJ, van Alphen HA, Hoogland PV. Morphology of the human internal vertebral venous plexus: a cadaver study after intravenous araldite CY 221 injection. Anat Rec. 1997; Oct. 249(2):285–94.
Article4. He H, Li Q, Du M, Chen K, Li X, Li J, et al. Endovascular and surgical approaches of iatrogenic vertebrovertebral arteriovenous fistula. J Vasc Surg Cases Innov Tech. 2021; Feb. 7(2):206–10.
Article5. Mitchell J. Vertebral artery blood flow velocity changes associated with cervical spine rotation: a meta-analysis of the evidence with implications for professional practice. J Man Manip Ther. 2009; 17(1):46–57.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Deconstructive repair of a direct carotid-cavernous fistula via a posterior circulation retrograde approach
- Endovascular Stent-Graft Treatment of a Traumatic Vertebral Artery Pseudoaneurysm and Vertebrojugular Fistula
- Cervical spinal extradural arteriovenous fistula successfully treated using transarterial balloon-assisted coil embolization
- Post-Traumatic Arteriovenous Fistula of the Scalp
- Stereotactic radiosurgery for dural arteriovenous fistula
