Middle meningeal artery: An effective pathway for achieving complete obliteration following transarterial Ethylene Vinyl Copolymer (Onyx) embolization of dural arteriovenous fistulas
- Akamatsu Y1,2
- Gomez-Paz S1
- Tonetti DA3
- Vergara-Garcia D1
- Moholkar VM4
- Kuhn AL4
- Chida K1,2
- Singh J4
- Rodrigues KdM4
- Massari F4
- Moore JM1
- Ogilvy CS1
- Puri AS4
- Thomas AJ
 5
5
- Affiliations
-
- 1Neurosurgical Service, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, USA
- 2Department of Neurosurgry, Iwate Medical University, Yahaba, Japan
- 3Department of Neurosurgery University of California San Francisco, San Francisco, CA, USA
- 4Division of Interventional Neuroradiology, Department of Radiology, University of Massachusetts Medical Center, Worcester, MA, USA
- 5Department of Neurological Surgery, Cooper University Health Care, Camden, NJ, USA
- KMID: 2533672
- DOI: http://doi.org/10.7461/jcen.2022.E2021.03.008
Abstract
Objective
Transarterial Onyx embolization is the mainstay of intracranial non-cavernous dural arteriovenous fistulas (dAVFs) treatment. Although the dural arterial supply varies depending on the location, the impact of arterial access on treatment outcomes has remained unclear. The aim of this study was to characterize factors as sociated with complete obliteration following transarterial Onyx embolization, with a special focus on arterial access routes and dAVF location.
Methods
A retrospective analysis of the patients who underwent transarterial Onyx embolization for intracranial dAVFs at two academic institutions was performed. Patients with angiographic follow-up were considered eligible to investigate the impact of the arterial access on achieving complete obliteration.
Results
Sixty-eight patients underwent transarterial Onyx embolization of intracranial dAVFs. Complete obliteration was achieved in 65% of all treated patients and in 75% of those with cortical venous reflux. Multivariable analysis identified middle meningeal artery (MMA) access to be a significant independent predictive factor for complete obliteration (OR, 2.32; 95% CI, 1.06-5.06; p=0.034). Subgroup analysis showed that supratentorial and lateral cerebellar convexity dAVFs (OR, 5.72, 95% CI, 1.89-17.33, p=0.002), and Borden type III classification at pre-treatment (OR, 3.13, 95% CI, 1.05- 9.35, p=0.041), were independent predictive factors for complete obliteration following embolization through the MMA.
Conclusions
MMA access is an independent predictive factor for complete obliteration following transarterial Onyx embolization for intracranial non-cavernous dAVFs. It is particularly effective for supratentorial and lateral cerebellar convexity dAVFs and those that are Borden type III.
Keyword
Figure
-
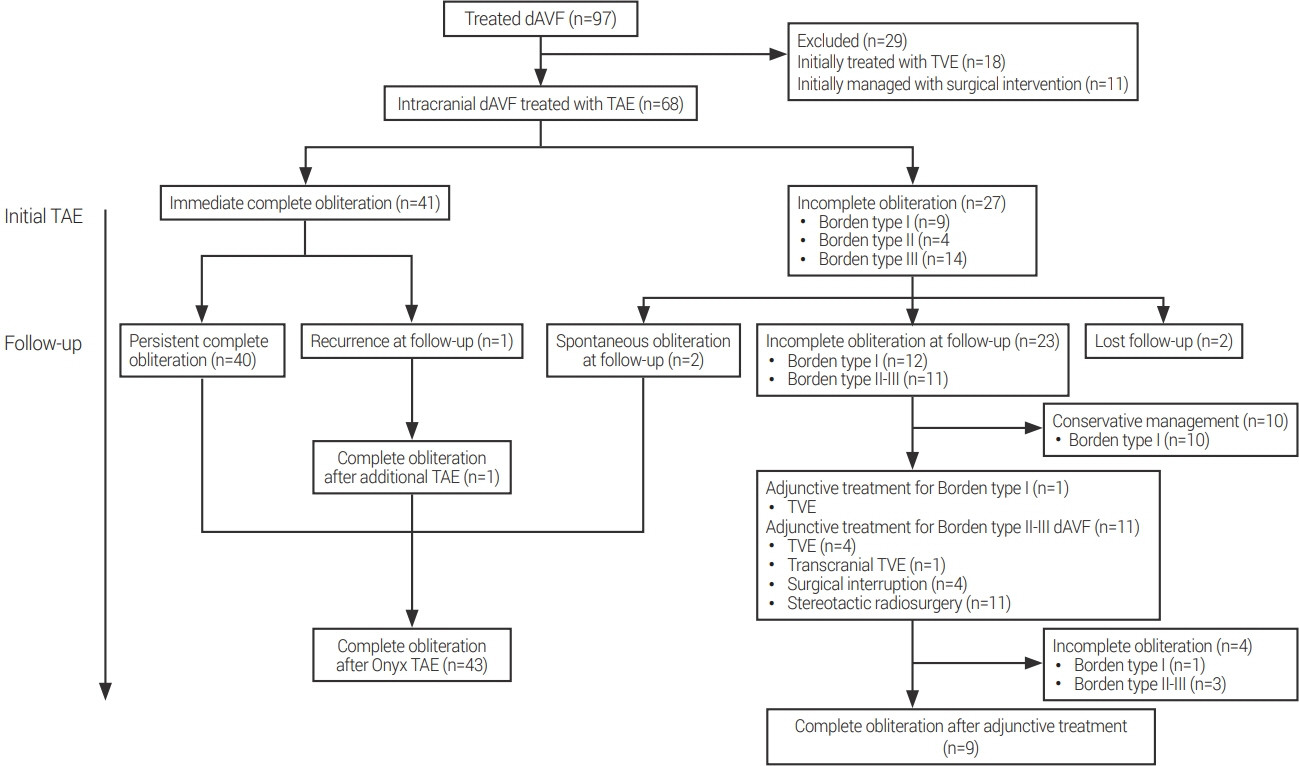
Fig. 1. Treatment flow diagram of our study cohort. TAE, transarterial embolization; dAVF, dural arteriovenous fistula; TVE, transvenous embolization

Fig. 2. Lateral view of left external carotid artery angiogram showing the dAVF at the isolated transverse sinus fed by the posterior convexity branch of the middle meningeal artery (MMA) (black arrowhead) and transosseous branch of the occipital artery (white arrowhead), and drainage into the dilated cortical vein (black arrow) (A). Selective angiogram of the MMA showing a wedged microcatheter position (B). Left external carotid artery angiogram obtained after embolization confirming complete dAVF obliteration (C). Non-subtracted image showing Onyx cast following embolization (white arrows) (D). dAVF, dural arteriovenous fistula
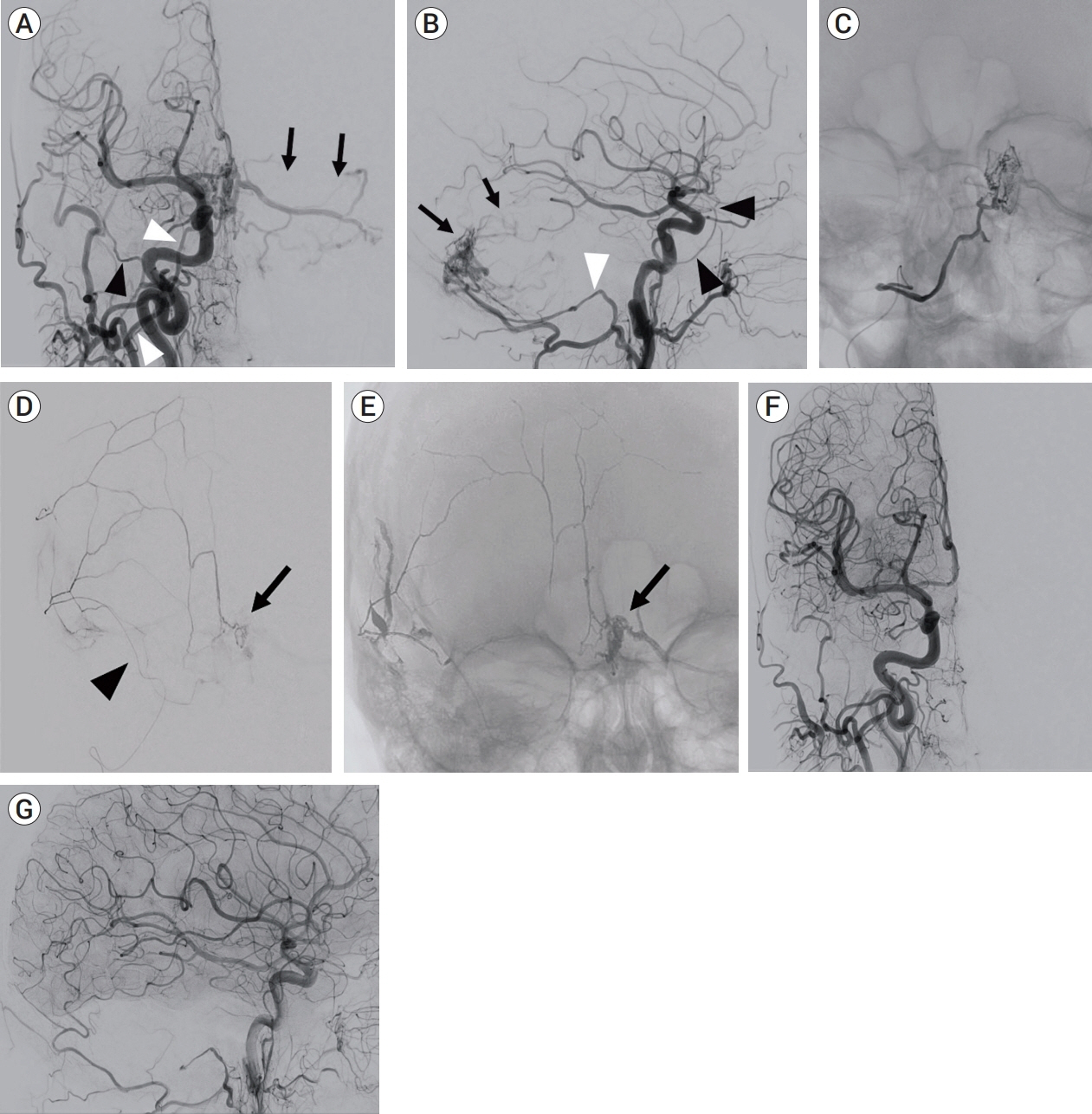
Fig. 3. Anteroposterior (A) and lateral (B) view of right common carotid artery angiogram showing a dAVF at the torcula fed by the hypoglossal branches (white arrowheads) of the occipital artery (OA) and draining into left cerebellar cortical veins (black arrows). Note that feeding branches from the middle meningeal artery (MMA) (black arrowheads) are not clearly identified on this injection. Anteroposterior (C) view of selective angiogram of the hypoglossal branch of the OA. Onyx injection was not attempted due to the difficulty of distal catheter navigation. Selective injection from the small caliber MMA showing a wedged microcatheter position (black arrowhead) and contribution to the fistula (black arrow) (D). Non-subtracted image showing Onyx cast penetrating into the fistula pouch (black arrow) (E). Anteroposterior (F) and lateral (G) view of the right common carotid artery angiogram obtained after embolization through the small MMA confirming complete fistula obliteration. dAVF, dural arteriovenous fistula
Reference
-
1. Borden JA, Wu JK, Shucart WA. A proposed classification for spinal and cranial dural arteriovenous fistulous malformations and implications for treatment. J Neurosurg. 1995; Feb. 82(2):166–79.
Article2. Cha KC, Yeon JY, Kim GH, Jeon P, Kim JS, Hong SC. Clinical and angiographic results of patients with dural arteriovenous fistula. J Clin Neurosci. 2013; Apr. 20(4):536–42.
Article3. Chandra RV, Leslie-Mazwi TM, Mehta BP, Yoo AJ, Rabinov JD, Pryor JC, et al. Transarterial Onyx embolization of cranial dural arteriovenous fistulas: long-term follow-up. AJNR Am J Neuroradiol. 2014; Sep. 35(9):1793–7.
Article4. Chapot R, Stracke P, Velasco A, Nordmeyer H, Heddier M, Stauder M, et al. The pressure cooker technique for the treatment of brain AVMs. J Neuroradiol. 2014; Mar. 41(1):87–91.
Article5. De Keukeleire K, Vanlangenhove P, Kalala Okito JP, Hallaert G, Van Roost D, Defreyne L. Transarterial embolization with Onyx for treatment of intracranial non-cavernous dural arteriovenous fistula with or without cortical venous reflux. J Neurointerv Surg. 2011; Sep. 3(3):224–8.
Article6. Kim B, Jeon P, Kim K, Kim S, Kim H, Byun HS, et al. Predictive factors for response of intracranial dural arteriovenous fistulas to transarterial Onyx embolization: angiographic subgroup analysis of treatment outcomes. World Neurosurg. 2016; Apr. 88:609–18.
Article7. Mantilla D, Le Corre M, Cagnazzo F, Gascou G, Eker O, Machi P, et al. Outcome of transarterial treatment of dural arteriovenous fistulas with direct or indirect cortical venous drainage. J Neurointerv Surg. 2018; Oct. 10(10):958–63.
Article8. Martins C, Yasuda A, Campero A, Ulm AJ, Tanriover N, Rhoton A Jr. Microsurgical anatomy of the dural arteries. Neurosurgery. 2005; Apr. 56(2 Suppl):211–51. discussion 211-51.
Article9. Sadeh-Gonike U, Magand N, Armoiry X, Riva R, Labeyrie PE, Lamy B, et al. Transarterial Onyx embolization of intracranial dural fistulas: a prospective cohort, systematic review, and meta-analysis. Neurosurgery. 2018; Jun. 82(6):854–63.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Treatment of Dural Arteriovenous Fistulas: Single Center Experience
- A Case of Intraosseous Dural Arteriovenous Fistulas Involving Diploic Vein Treated with Transarterial Onyx Embolization
- Transcranial Direct Middle Meningeal Artery Puncture for the Onyx Embolization of Dural Arteriovenous Fistula Involving the Superior Sagittal Sinus
- Hairball-Like Migration of “Onyx Threads” into the Draining Vein during Transarterial Embolization of a Dural Arteriovenous Fistula: A Case Report and Experimental Validation
- Dural Arteriovenous Fistula Involving Transverse Sinus: Successful Embolization Using Onyx(R)
