Ann Surg Treat Res.
2022 Aug;103(2):81-86. 10.4174/astr.2022.103.2.81.
Comparison of gastric-jejunum pouch anastomosis and Billroth-II reconstructions after distal gastrectomy: a propensity score matching analysis
- Affiliations
-
- 1General Surgery Center, The General Hospital of Western Theater Command, Chengdu, China
- 2Western Theater Command Center for Disease Control and Prevention, Chengdu, China
- KMID: 2532362
- DOI: http://doi.org/10.4174/astr.2022.103.2.81
Abstract
- Purpose
Our study aimed to make a propensity score matching (PSM) analysis on the clinical application of gastricjejunum pouch anastomosis (GJPA) and Billroth-II anastomosis after distal gastrectomy.
Methods
We collected clinical data from 249 patients who received distal gastrectomy from January 2016 to July 2020. According to the reconstruction method used, all patients were divided into the Billroth-II group and the GJPA group. Clinical data and operation complications were analyzed.
Results
The clinical characteristics of the 2 groups were comparable after PSM. In the Billroth-II group, the incidence rate of delayed gastric emptying was higher than that in the GJPA group. Fewer patients suffered reflux gastritis in the GJPA group. The RGB (residue, gastritis, and bile) scores related to the severity of bile reflux into the remnant stomach, gastritis, and residue were higher in the Billroth-II group. Postoperative nutritional status and Visick classification demonstrated that postoperative subjective feelings in the GJPA group were improved significantly.
Conclusion
The application of GJPA in reconstruction after distal gastrectomy is safe, economical, and reliable. This reconstruction improved the quality of life of patients. It is worth popularizing widely in clinical settings.
Keyword
Figure
-
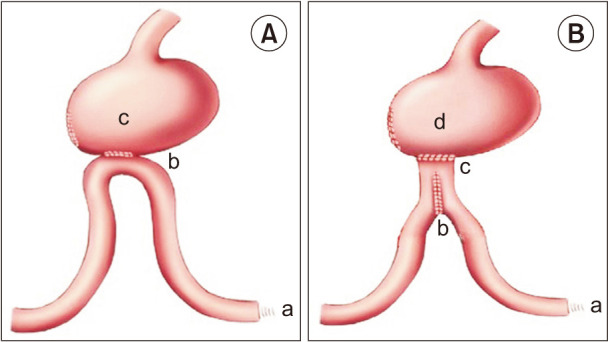
Fig. 1 (A) Billroth-II reconstruction. a, Treitz ligament; b, gastrointestinal anastomosis; and c, residual stomach. (B) Gastric-jejunum pouch anastomosis reconstruction. a, Treitz ligament; b, jejunal pouch (6 cm); c, gastrointestinal anastomosis; and d, residual stomach.
Reference
-
1. Lee S, Lee H, Lee J. Feasibility and safety of totally laparoscopic radical gastrectomy for advanced gastric cancer: comparison with early gastric cancer. J Gastric Cancer. 2018; 18:152–160. PMID: 29984065.
Article2. Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016; 66:115–132. PMID: 26808342.
Article3. So JB, Rao J, Wong AS, Chan YH, Pang NQ, Tay AY, et al. Roux-en-Y or Billroth II reconstruction after radical distal gastrectomy for gastric cancer: a multicenter randomized controlled trial. Ann Surg. 2018; 267:236–242. PMID: 28383294.
Article4. Kim JM, Park JH, Jeong SH, Lee YJ, Ju YT, Jeong CY, et al. Relationship between low body mass index and morbidity after gastrectomy for gastric cancer. Ann Surg Treat Res. 2016; 90:207–212. PMID: 27073791.
Article5. Lee MS, Ahn SH, Lee JH, Park DJ, Lee HJ, Kim HH, et al. What is the best reconstruction method after distal gastrectomy for gastric cancer? Surg Endosc. 2012; 26:1539–1547. PMID: 22179454.
Article6. Chen S, Chen DW, Chen XJ, Lin YJ, Xiang J, Peng JS. Postoperative complications and nutritional status between uncut Roux-en-Y anastomosis and Billroth II anastomosis after D2 distal gastrectomy: a study protocol for a multicenter randomized controlled trial. Trials. 2019; 20:428. PMID: 31300019.
Article7. Cao Y, Gong J, Gan W, Zhou J, Huang L, Wang Y, et al. Gastric-jejunum pouch side-to-end anastomosis: a novel and safe operation of gastrojejunostomy for preventing reflux gastritis. Int J Clin Exp Med. 2015; 8:5541–5546. PMID: 26131135.8. Santiago JM, Sasako M, Osorio J. [TNM-7th edition 2009 (UICC/AJCC) and Japanese Classification 2010 in Gastric Cancer: towards simplicity and standardisation in the management of gastric cancer]. Cir Esp. 2011; 89:275–281. Spanish. PMID: 21256476.
Article9. Nagano H, Ohyama S, Sakamoto Y, Ohta K, Yamaguchi T, Muto T, et al. The endoscopic evaluation of gastritis, gastric remnant residue, and the incidence of secondary cancer after pylorus-preserving and transverse gastrectomies. Gastric Cancer. 2004; 7:54–59. PMID: 15052441.
Article10. Poziomyck AK, Cavazzola LT, Coelho LJ, Lameu EB, Weston AC, Moreira LF. Nutritional assessment methods as predictors of postoperative mortality in gastric cancer patients submitted to gastrectomy. Rev Col Bras Cir. 2017; 44:482–490. PMID: 29019578.
Article11. Bove V, Tringali A, Familiari P, Gigante G, Boškoski I, Perri V, et al. ERCP in patients with prior Billroth II gastrectomy: report of 30 years’ experience. Endoscopy. 2015; 47:611–616. PMID: 25730282.
Article12. Vakhrushev IaM, Ivanov LA. [Changes in gastric secretory function in peptic ulcer patients after gastric resection]. Ter Arkh. 1991; 63:14–16. Russian.13. Collard JM, Romagnoli R. Roux-en-Y jejunal loop and bile reflux. Am J Surg. 2000; 179:298–303. PMID: 10875990.
Article14. Montesani C, D’Amato A, Santella S, Pronio A, Giovannini C, Cristaldi M, et al. Billroth I versus Billroth II versus Roux-en-Y after subtotal gastrectomy: prospective [correction of prespective] randomized study. Hepatogastroenterology. 2002; 49:1469–1473. PMID: 12239969.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of laparoscopy-assisted and totally laparoscopic Billroth-II distal gastrectomy for gastric cancer
- Comparative Study of Hand-Sutured versus Circular Stapled Anastomosis for Gastrojejunostomy in Laparoscopy Assisted Distal Gastrectomy
- Comparing short-term outcomes after totally laparoscopic distal gastrectomy and laparoscopy-assisted distal gastrectomy with Billroth I anastomosis: early experience of a single institution
- Recurrent Gastric Cancer at the Duodenal Stump after Billroth II Subtotal Gastrectomy
- Various types of reconstruction after pancreaticoduodenectomy for the patients who underwent all types of gastrectomy: a single-center experience
