J Neurocrit Care.
2022 Jun;15(1):76-77. 10.18700/jnc.210041.
A case of Brown-Sequard syndrome caused by spinal cord infarction
- Affiliations
-
- 1Department of Neurology, Ajou University Medical Center, Suwon, Korea
- KMID: 2532005
- DOI: http://doi.org/10.18700/jnc.210041
Figure
-

Fig. 1. Magnetic resonance imaging scans of cervical spinal cord obtained on admission date. (A, B) Diffusion-weighted imaging demonstrates diffusion restriction of the spinal cord between C2 and C5 level. (C) Sagittal T2-weighted image demonstrates high T2 signal intensity of the spinal cord between C2 and C5 level. (D) Axial T2-weighted image shows high T2 signal intensity of the right half of the spinal cord at C4 level.
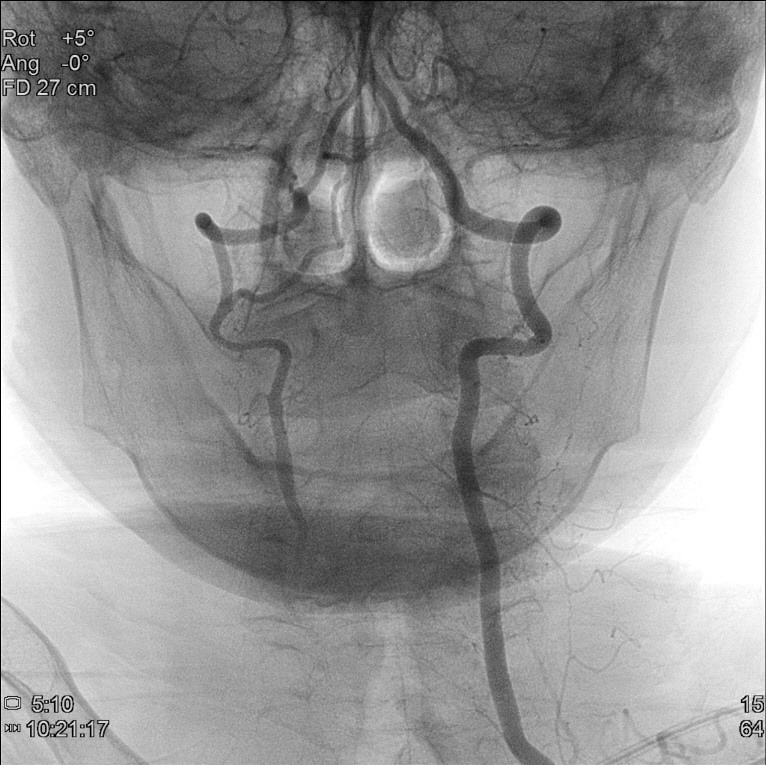
Fig. 2. Percutaneous cerebral angiography of posterior circulation showing the occlusion of right vertebral artery from its origin. The left vertebral artery, on the other hand, is intact.
Reference
-
1. Sandson TA, Friedman JH. Spinal cord infarction: report of 8 cases and review of the literature. Medicine (Baltimore). 1989; 68:282–92.2. Baumgartner RW, Waespe W. Anterior spinal artery syndrome of the cervical hemicord. Eur Arch Psychiatry Clin Neurosci. 1992; 241:205–9.
Article3. Santillan A, Nacarino V, Greenberg E, Riina HA, Gobin YP, Patsalides A. Vascular anatomy of the spinal cord. J Neurointerv Surg. 2012; 4:67–74.
Article4. Meng YY, Dou L, Wang CM, Kong DZ, Wei Y, Wu LS, et al. Spinal cord infarction presenting as Brown-Séquard syndrome from spontaneous vertebral artery dissection: a case report and literature review. BMC Neurol. 2019; 19:321.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Brown-Sequard Syndrome Caused by Spinal Cord Infarction: A Case Report and Literature Review
- Brown-Sequard Syndrome due to Herniated Cervical Disc
- Idiopathic Spinal Cord Herniation as a Treatable Cause of Progressive Brown-Sequard Syndrome
- Idiopathic Spinal Cord Herniation Presented as Brown-Sequard Syndrome: A Case Report and Surgical Outcome
- Motion Preserving Surgery in Two Cases of Brown-Sequard Syndrome Caused by Herniated Cervical Discs
