Effect of the Concomitant Use of Subcutaneous Basal Insulin and Intravenous Insulin Infusion in the Treatment of Severe Hyperglycemic Patients
- Lim Y
 1,2
1,2 - Ohn JH1,2
- Jeong J3
- Ryu J1,2
- Kim Sw1,2
- Cho JH1,2
- Park HS1,2
- Kim HW1,2
- Lee J1,2
- Kim ES1,2
- Kim NH1,2
- Jo YH3
- Jang HC1,2
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea
- 2Hospital Medicine Center, Seoul National University Bundang Hospital, Seongnam, Korea
- 3Department of Emergency Medicine, Seoul National University Bundang Hospital, Seongnam, Korea
- KMID: 2531388
- DOI: http://doi.org/10.3803/EnM.2021.1341
Abstract
- Background
No consensus exists regarding the early use of subcutaneous (SC) basal insulin facilitating the transition from continuous intravenous insulin infusion (CIII) to multiple SC insulin injections in patients with severe hyperglycemia other than diabetic ketoacidosis. This study evaluated the effect of early co-administration of SC basal insulin with CIII on glucose control in patients with severe hyperglycemia.
Methods
Patients who received CIII for the management of severe hyperglycemia were divided into two groups: the early basal insulin group (n=86) if they received the first SC basal insulin 0.25 U/kg body weight within 24 hours of CIII initiation and ≥4 hours before discontinuation, and the delayed basal insulin group (n=79) if they were not classified as the early basal insulin group. Rebound hyperglycemia was defined as blood glucose level of >250 mg/dL in 24 hours following CIII discontinuation. Propensity score matching (PSM) methods were additionally employed for adjusting the confounding factors (n=108).
Results
The rebound hyperglycemia incidence was significantly lower in the early basal insulin group than in the delayed basal insulin group (54.7% vs. 86.1%), despite using PSM methods (51.9%, 85.2%). The length of hospital stay was shorter in the early basal insulin group than in the delayed basal insulin group (8.5 days vs. 9.6 days, P=0.027). The hypoglycemia incidence did not differ between the groups.
Conclusion
Early co-administration of basal insulin with CIII prevents rebound hyperglycemia and shorten hospital stay without increasing the hypoglycemic events in patients with severe hyperglycemia.
Figure
-
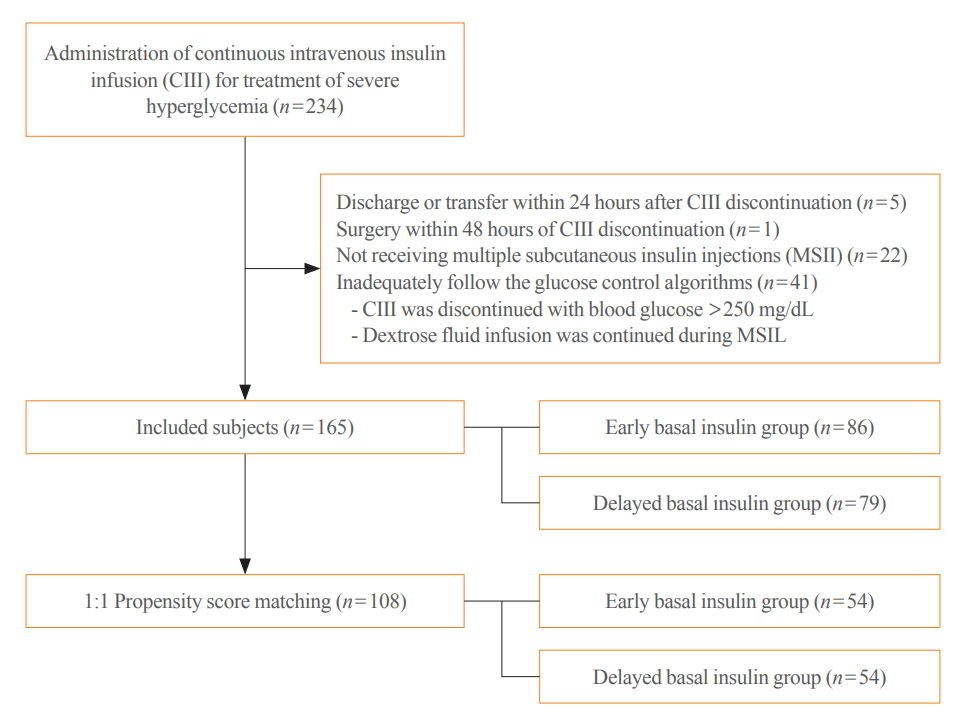
Fig. 1. Flow chart of patient enrollment. Among identified 234 subjects, 165 subjects were finally included. MSII, multiple subcutaneous insulin injection.
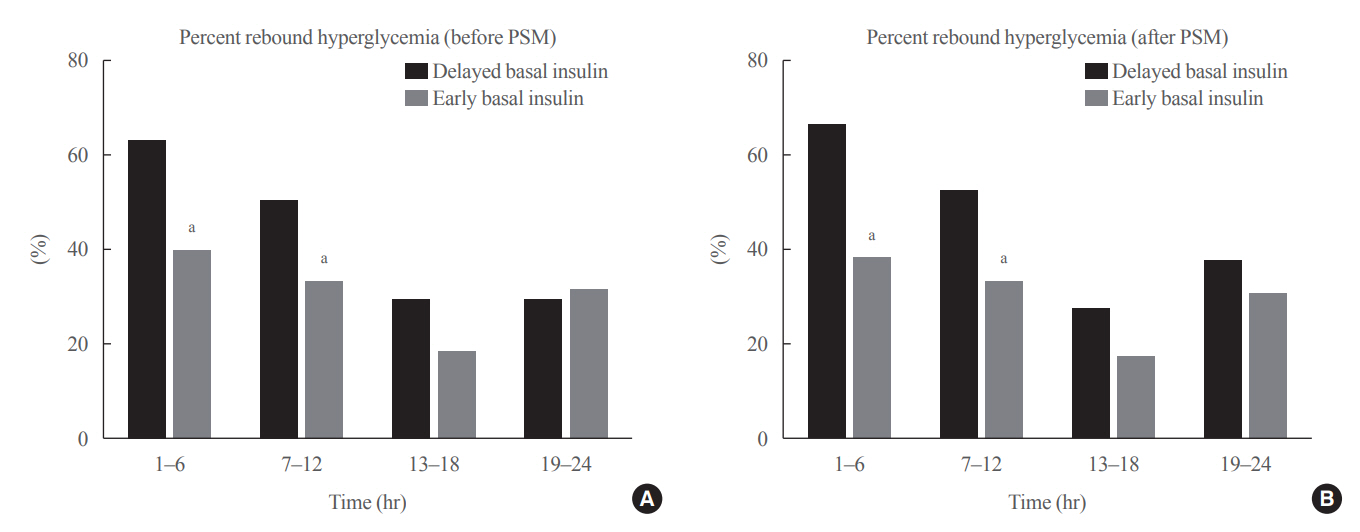
Fig. 2. Incidence of rebound hyperglycemia stratified by 6 hours intervals (A) before and (B) after propensity score matching (PSM). The rate of rebound hyperglycemia was lower in the early basal group than in the delayed basal group during the first 12 hours. aStatistically significant (P<0.05) by Fisher exact tests.
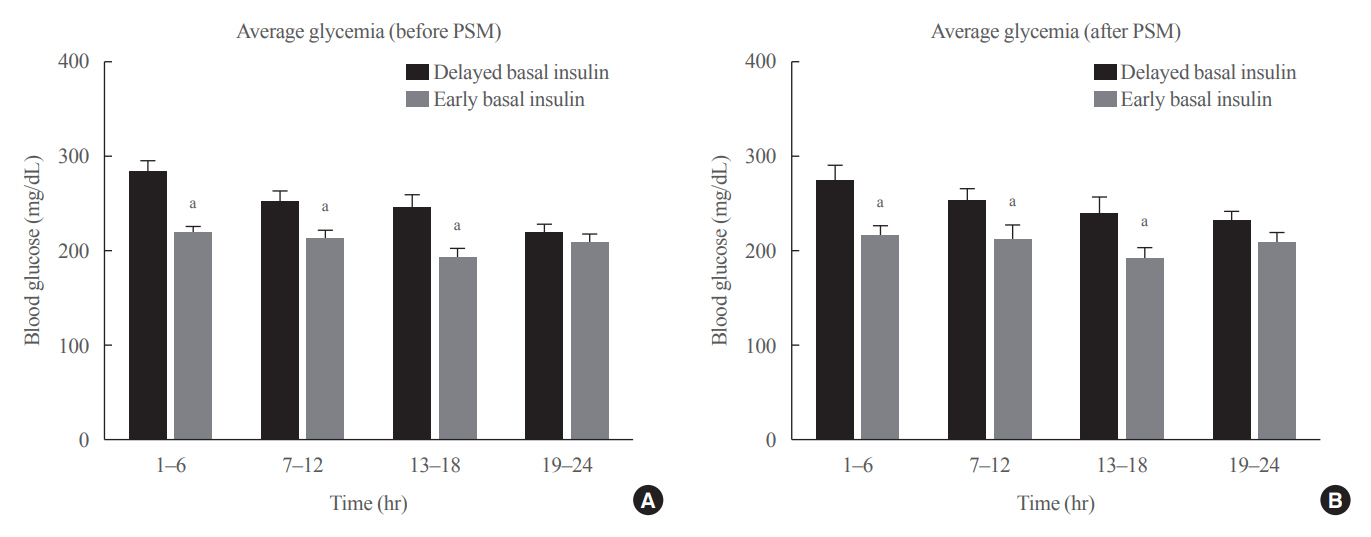
Fig. 3. Average glucose level categorized into four 6-hour intervals (A) before and (B) after propensity score matching (PSM). Data presented as mean±standard error of the mean. The average blood glucose levels were lower in the first 18 hours. aStatistically significant (P<0.05)by Mann-Whitney U tests.
Reference
-
1. American Diabetes Association. 15. Diabetes care in the hospital: standards of medical care in diabetes-2021. Diabetes Care. 2021; 44(Suppl 1):S211–20.2. Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN. Hyperglycemic crises in adult patients with diabetes. Diabetes Care. 2009; 32:1335–43.
Article3. Umpierrez G, Korytkowski M. Diabetic emergencies: ketoacidosis, hyperglycaemic hyperosmolar state and hypoglycaemia. Nat Rev Endocrinol. 2016; 12:222–32.
Article4. Luzi L, Barrett EJ, Groop LC, Ferrannini E, DeFronzo RA. Metabolic effects of low-dose insulin therapy on glucose metabolism in diabetic ketoacidosis. Diabetes. 1988; 37:1470–7.
Article5. Moghissi ES, Korytkowski MT, DiNardo M, Einhorn D, Hellman R, Hirsch IB, et al. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Diabetes Care. 2009; 32:1119–31.
Article6. Ramos P, Childers D, Maynard G, Box K, Namba J, Stadalman K, et al. Maintaining glycemic control when transitioning from infusion insulin: a protocol-driven, multidisciplinary approach. J Hosp Med. 2010; 5:446–51.
Article7. Avanzini F, Marelli G, Donzelli W, Busi G, Carbone S, Bellato L, et al. Transition from intravenous to subcutaneous insulin: effectiveness and safety of a standardized protocol and predictors of outcome in patients with acute coronary syndrome. Diabetes Care. 2011; 34:1445–50.8. Furnary AP, Braithwaite SS. Effects of outcome on in-hospital transition from intravenous insulin infusion to subcutaneous therapy. Am J Cardiol. 2006; 98:557–64.
Article9. Weant KA, Ladha A. Conversion from continuous insulin infusions to subcutaneous insulin in critically ill patients. Ann Pharmacother. 2009; 43:629–34.
Article10. Hsia E, Seggelke S, Gibbs J, Hawkins RM, Cohlmia E, Rasouli N, et al. Subcutaneous administration of glargine to diabetic patients receiving insulin infusion prevents rebound hyperglycemia. J Clin Endocrinol Metab. 2012; 97:3132–7.
Article11. Czosnowski QA, Swanson JM, Lobo BL, Broyles JE, Deaton PR, Finch CK. Evaluation of glycemic control following discontinuation of an intensive insulin protocol. J Hosp Med. 2009; 4:28–34.
Article12. Barski L, Brandstaetter E, Sagy I, Jotkowitz A. Basal insulin for the management of diabetic ketoacidosis. Eur J Intern Med. 2018; 47:14–6.
Article13. Niswender KD. Basal insulin: physiology, pharmacology, and clinical implications. Postgrad Med. 2011; 123:17–26.
Article14. Heise T, Hermanski L, Nosek L, Feldman A, Rasmussen S, Haahr H. Insulin degludec: four times lower pharmacodynamic variability than insulin glargine under steady-state conditions in type 1 diabetes. Diabetes Obes Metab. 2012; 14:859–64.
Article15. Ratner RE, Gough SC, Mathieu C, Del Prato S, Bode B, Mersebach H, et al. Hypoglycaemia risk with insulin degludec compared with insulin glargine in type 2 and type 1 diabetes: a pre-planned meta-analysis of phase 3 trials. Diabetes Obes Metab. 2013; 15:175–84.
Article16. Ketan D, Mark S. The management of diabetic ketoacidosis in adults [Internet]. Solihull: Joint British Diabetes Societies Inpatient Care Group;2013. [cited 2022 Mat 9]. Available from: https://abcd.care/resource/jbds-02-management-diabeticketoacidosis-adults.17. Holt RIG. Textbook of diabetes. 4th ed. Oxford: Blackwell Publishing Ltd;2010. Chapter 34, Acute metabolic complications of diabetes: diabetic ketoacidosis and hyperosmolar hyperglycemia. p. 546–52.18. Clement S, Braithwaite SS, Magee MF, Ahmann A, Smith EP, Schafer RG, et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004; 27:553–91.
Article19. Kelly JL. Continuous insulin infusion: when, where, and how? Diabetes Spectr. 2014; 27:218–23.
Article20. Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009; 28:3083–107.
Article21. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale: Lawrence Erlbaum Associates;1988.22. Stuart EA, Lee BK, Leacy FP. Prognostic score-based balance measures can be a useful diagnostic for propensity score methods in comparative effectiveness research. J Clin Epidemiol. 2013; 66(8 Suppl):S84–90.
Article23. Rubin DB. Using propensity scores to help design observational studies: application to the tobacco litigation. Health Serv Outcomes Res Methodol. 2001; 2:169–88.24. Houshyar J, Bahrami A, Aliasgarzadeh A. Effectiveness of insulin glargine on recovery of patients with diabetic ketoacidosis: a randomized controlled trial. J Clin Diagn Res. 2015; 9:OC01–5.
Article25. Rappaport SH, Endicott JA, Gilbert MP, Farkas JD, Clouser RD, McMillian WD. A retrospective study of early vs delayed home dose basal insulin in the acute management of diabetic ketoacidosis. J Endocr Soc. 2019; 3:1079–86.
Article26. Harrison VS, Rustico S, Palladino AA, Ferrara C, Hawkes CP. Glargine co-administration with intravenous insulin in pediatric diabetic ketoacidosis is safe and facilitates transition to a subcutaneous regimen. Pediatr Diabetes. 2017; 18:742–8.
Article27. Becker RH, Dahmen R, Bergmann K, Lehmann A, Jax T, Heise T. New insulin glargine 300 units · mL-1 provides a more even activity profile and prolonged glycemic control at steady state compared with insulin glargine 100 units·mL-1. Diabetes Care. 2015; 38:637–43.28. Lucidi P, Porcellati F, Rossetti P, Candeloro P, Cioli P, Marzotti S, et al. Pharmacokinetics and pharmacodynamics of therapeutic doses of basal insulins NPH, glargine, and detemir after 1 week of daily administration at bedtime in type 2 diabetic subjects: a randomized cross-over study. Diabetes Care. 2011; 34:1312–4.29. Scott AR; Joint British Diabetes Societies (JBDS) for Inpatient Care. Management of hyperosmolar hyperglycaemic state in adults with diabetes. Diabet Med. 2015; 32:714–24.
Article30. Aggarwal A, Rawn JD, Pendergrass ML, Garg RK. Long-acting subcutaneously administered insulin for glycemic control immediately after cardiac surgery. Endocr Pract. 2011; 17:558–62.
Article31. Doshi P, Potter AJ, De Los Santos D, Banuelos R, Darger BF, Chathampally Y. Prospective randomized trial of insulin glargine in acute management of diabetic ketoacidosis in the emergency department: a pilot study. Acad Emerg Med. 2015; 22:657–62.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intraoperative and Postoperative Glycemic Management in Patients with Diabetes
- Continuous subcutaneous insulin infusion and glycemic control
- Unusually Elevated Serum Insulin Level in a Diabetic Patient during Recombinant Insulin Therapy
- Intensive Insulin Therapy in Type 1 Diabetes
- Correlation between Basal Insulin Requirements and Daily Administered Insulin Dosage in Diabetes
