Strategies for Renal Protection in Cardiovascular Interventions
- Ali ZA
 1,2,3
1,2,3 - Escaned J4
- Dudek D5,6
- Radhakrishnan J7
- Galougahi KK8,9
- Affiliations
-
- 1The Heart Center, St. Francis Hospital, Roslyn, NY, USA
- 2DeMatteis Cardiovascular Institute, St. Francis Hospital, Roslyn, NY, USA
- 3Clinical Trials Center, Cardiovascular Research Foundation, New York, NY, USA
- 4Hospital Clinico San Carlos IDISSC and Universidad Complutense de Madrid, Madrid, Spain
- 5Institute of Cardiology, Jagiellonian University, Krakow, Poland
- 6Maria Cecilia Hospital, GVM Care & Research, Cotignola (RA), Ravenna, Italy
- 7Division of Nephrology, Department of Medicine, Vagelos College of Physicians & Surgeons, Columbia University, New York, NY, USA
- 8Heart Research Institute, Sydney, Australia
- 9Sydney Medical School, Faculty of Medicine and Health, The University of Sydney, Sydney, Australia
- KMID: 2530730
- DOI: http://doi.org/10.4070/kcj.2022.0093
Abstract
- Coronary artery disease is highly prevalent in chronic kidney disease (CKD) and is a risk factor for contrast-associated acute kidney injury (CA-AKI), a complication of cardiovascular procedures that require contrast administration (e.g., coronary angiography, percutaneous coronary intervention [PCI]). CA-AKI has a major impact on morbidity, mortality, and healthcare resource utilization. The incidence of CA-AKI is particularly high in patients with pre-existing CKD, advanced age and comorbidities that increase the likelihood of CKD. The focus of the present review is to provide a brief overview on the assessment of the risk for and prevention of CA-AKI in patients undergoing angiography and PCI, including recognition of the important patient- and procedure-related factors that may contribute to CA-AKI. Preventive and treatment strategies, the mainstay of which is volume repletion by normal saline, are briefly discussed. The main focus of the review is placed on technical details of contrast minimization techniques, including ultra-low contrast angiography and zerocontrast PCI. Operator competence in such techniques is important to ensure that procedural challenges in patients with CKD, like vessel calcification, multivessel disease and complex anatomical subsets, are effectively addressed by PCI while minimizing the risk of CA-AKI.
Keyword
Figure
-

Figure 1 Pathway for ultra-low contrast angiography and ultra-low or zero-contrast percutaneous intervention.ACS = acute coronary syndrome; AP = antero-posterior; CA-AKI = contrast-associated acute kidney injury; CCS = chronic coronary syndrome; CV = contrast volume; DES = drug-eluting stent; DM = diabetes mellitus; EKG = electrocardiogram; GFR = glomerular filtration rate; LAO = left anterior oblique; LCA = left coronary artery; LVEDP = left ventricular end-diastolic pressure; MAX = Medial dissection, Apposition, eXpansion; MLD = Morphology, Length, Diameter ; PCI = percutaneous coronary intervention.

Figure 2 Ultra-low contrast angiography in a patient with advanced chronic kidney disease (stage 5, estimated glomerular filtration rate 13 mL/min). (A) Radial access is avoided so that the radial artery is preserved for access for hemodialysis in the near future. Femoral access is performed using a combination of ultrasound to mark the common femoral bifurcation, a hemostat to mark the mid-femoral head using the micropuncture kit to gain access. (B) The left ventricular end diastolic pressure is measured to guide intravenous hydration. (C) Intracoronary injection of 10 mL of 0.9% heparinized normal saline. If the catheter is engaged, transient EKG changes will occur. Single view, low-magnification, non-panned angiograms of the right (LAO-cranial), circumflex (AP-caudal), and left anterior descending coronary arteries (AP-cranial) are obtained. Total contrast volume was 9.6 mL.AP = antero-posterior; LAO = left anterior oblique.
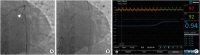
Figure 3 Ultra-low contrast angiography with adjunctive coronary physiology to resolve diagnostic ambiguity. (A) A patient with advanced chronic kidney disease (stage 5, estimated glomerular filtration rate 8 mL/min) undergoes ultra-low contrast angiography with contrast dilution, which suggests an ambiguous lesion in the proximal circumflex coronary artery (arrow). (B-C) Invasive coronary physiology is performed, without contrast-guidance, which excludes significant ischemia, with resting full-cycle ratio of 0.94.

Figure 4 Zero contrast percutaneous coronary intervention in a patient with advanced chronic kidney disease. (A) A road map from a previously performed ultralow contrast angiogram of the RCA with 3 mL contrast in the AP cranial view is projected. (B) Spot iFR of the distal vessel confirms significant ischemia (iFR 0.67). (C) Co-registration of iFR pullback with the angiographic silhouette of the guidewire reveals a focal flow-limiting stenosis in the mid RCA segment, while confirming that the proximal lesion (A*) is non-ischemic. (D) A reference segment distal to the lesion is identified manually and marked with cine angiography. (E) By co-registering the intravascular ultrasound system pullback with the guidewire, reference vessel measurements are performed at the distal reference segment, revealing a mean distal vessel size of 3.1 mm. (F) Following the same approach, a proximal, disease-free segment is identified, the length of lesion measured from the distal reference to this segment (yellow line) is 33.7 mm and mean proximal vessel size is 3.7 mm. (G-I) The stent is then deployed using co-registration, which may be automated (G), or manual (H), where the distal stent marker is aligned to the intravascular ultrasound transducer and a 3.0 mm by 33 mm drug eluting stent is deployed. (J) Using the advanced fluoroscopic device detection, the distal segment of stent is post-dilated pre-emptively with a 3.0 mm non-compliant balloon while avoiding the distal edge of the stent, and (K) the proximal segment of the stent with a 3.5 mm non-compliant balloon. (L) Stent expansion is assessed by measuring the manually identified minimal stent area (7.2 mm2) and comparing it with (M) the distal reference area (7.1 mm2), confirming >100% expansion. The distal and proximal stent edge were free of dissection (not shown). (N) A final spot iFR measurement confirms resolution of ischemia with pullback (O) confirming no need for further intra-stent optimization.AP = antero-posterior; iFR = instantaneous flow ratio; RCA = right coronary artery.

Figure 5 Techniques to increase safety of ultra-low or zero contrast percutaneous coronary intervention. (A) Baseline coronary angiogram. (B) Workhorse guide wires are bent at the tip with exaggerated curves to promote knuckling of the wire (white circles) and protect against distal wire perforation. (C) Dynamic coronary roadmap, a real-time, motion-compensated navigation system, can help prevent inadvertent wire passage into small vessels, which may track along the same course as the target vessel.
Reference
-
1. Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. Am J Kidney Dis. 2002; 39:930–936. PMID: 11979336.
Article2. Mozaffarian D, Benjamin EJ, Go AS, et al. Executive summary: heart disease and stroke statistics--2016 update: a report from the American Heart Association. Circulation. 2016; 133:447–454. PMID: 26811276.3. Solomon R. Contrast media: are there differences in nephrotoxicity among contrast media? BioMed Res Int. 2014; 2014:934947. PMID: 24587997.
Article4. Weisbord SD, Palevsky PM. Contrast-induced acute kidney injury: short- and long-term implications. Semin Nephrol. 2011; 31:300–309. PMID: 21784279.
Article5. Tong J, Li H, Zhang H, et al. Neutrophil gelatinase-associated lipocalin in the prediction of contrast-induced nephropathy: a systemic review and meta-analysis. J Cardiovasc Pharmacol. 2015; 66:239–245. PMID: 25915514.
Article6. Chertow GM, Normand SL, McNeil BJ. “Renalism”: inappropriately low rates of coronary angiography in elderly individuals with renal insufficiency. J Am Soc Nephrol. 2004; 15:2462–2468. PMID: 15339996.
Article7. Section 2: AKI definition. Kidney Int Suppl (2011). 2012; 2:19–36. PMID: 25018918.8. van der Molen AJ, Reimer P, Dekkers IA, et al. Post-contrast acute kidney injury - Part 1: definition, clinical features, incidence, role of contrast medium and risk factors: recommendations for updated ESUR Contrast Medium Safety Committee guidelines. Eur Radiol. 2018; 28:2845–2855. PMID: 29426991.
Article9. Budano C, Levis M, D’Amico M, et al. Impact of contrast-induced acute kidney injury definition on clinical outcomes. Am Heart J. 2011; 161:963–971. PMID: 21570530.
Article10. Slocum NK, Grossman PM, Moscucci M, et al. The changing definition of contrast-induced nephropathy and its clinical implications: insights from the Blue Cross Blue Shield of Michigan Cardiovascular Consortium (BMC2). Am Heart J. 2012; 163:829–834. PMID: 22607861.
Article11. Mehran R, Aymong ED, Nikolsky E, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. 2004; 44:1393–1399. PMID: 15464318.
Article12. Fähling M, Seeliger E, Patzak A, Persson PB. Understanding and preventing contrast-induced acute kidney injury. Nat Rev Nephrol. 2017; 13:169–180. PMID: 28138128.
Article13. Tziakas D, Chalikias G, Stakos D, et al. Validation of a new risk score to predict contrast-induced nephropathy after percutaneous coronary intervention. Am J Cardiol. 2014; 113:1487–1493. PMID: 24630389.
Article14. Gurm HS, Seth M, Dixon SR, et al. Contemporary use of and outcomes associated with ultra-low contrast volume in patients undergoing percutaneous coronary interventions. Catheter Cardiovasc Interv. 2019; 93:222–230. PMID: 30144337.
Article15. Ranucci M, Castelvecchio S, Menicanti L, Frigiola A, Pelissero G. Risk of assessing mortality risk in elective cardiac operations: age, creatinine, ejection fraction, and the law of parsimony. Circulation. 2009; 119:3053–3061. PMID: 19506110.
Article16. Liu YH, Liu Y, Zhou YL, et al. Comparison of different risk scores for predicting contrast induced nephropathy and outcomes after primary percutaneous coronary intervention in patients with ST elevation myocardial infarction. Am J Cardiol. 2016; 117:1896–1903. PMID: 27161818.
Article17. Mohebi R, Karimi Galougahi K, Garcia JJ, et al. Long-term clinical impact of contrast-associated acute kidney injury following PCI: an ADAPT-DES Substudy. JACC Cardiovasc Interv. 2022; 15:753–766. PMID: 35305904.
Article18. Isaka Y, Hayashi H, Aonuma K, et al. Guideline on the use of iodinated contrast media in patients with kidney disease 2018. Clin Exp Nephrol. 2020; 24:1–44.
Article19. Brar SS, Aharonian V, Mansukhani P, et al. Haemodynamic-guided fluid administration for the prevention of contrast-induced acute kidney injury: the POSEIDON randomised controlled trial. Lancet. 2014; 383:1814–1823. PMID: 24856027.
Article20. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012; 120:c179–c184. PMID: 22890468.
Article21. Ali ZA, Karimi Galougahi K, Nazif T, et al. Imaging- and physiology-guided percutaneous coronary intervention without contrast administration in advanced renal failure: a feasibility, safety, and outcome study. Eur Heart J. 2016; 37:3090–3095. PMID: 26957421.
Article22. Nyman U, Björk J, Aspelin P, Marenzi G. Contrast medium dose-to-GFR ratio: a measure of systemic exposure to predict contrast-induced nephropathy after percutaneous coronary intervention. Acta Radiol. 2008; 49:658–667. PMID: 18568558.
Article23. Rahim HM, Flattery E, Gkargkoulas F, et al. Ultra-low-contrast angiography in patients with advanced chronic kidney disease and previous coronary artery bypass surgery. Coron Artery Dis. 2019; 30:346–351. PMID: 31094895.
Article24. Bhatti N, Rahim H, Chen S, et al. Ultra-low contrast coronary angiography in patients with advanced chronic kidney disease: feasibility and outcomes compared with conventional angiography. J Am Coll Cardiol. 2019; 74:B30.25. Karimi Galougahi K, Zalewski A, Leon MB, Karmpaliotis D, Ali ZA. Optical coherence tomography-guided percutaneous coronary intervention in pre-terminal chronic kidney disease with no radio-contrast administration. Eur Heart J. 2016; 37:1059. PMID: 26685137.
Article26. Rahim H, Flattery E, Gkargkoulas F, et al. Clinical outcomes of imaging- and physiology-guided PCI without contrast administration in advanced renal failure. J Am Coll Cardiol. 2019; 74:B32.27. Karimi Galougahi K, Mintz GS, Karmpaliotis D, Ali ZA. Zero-contrast percutaneous coronary intervention on calcified lesions facilitated by rotational atherectomy. Catheter Cardiovasc Interv. 2017; 90:E85–E89. PMID: 28303645.
Article28. Karimi Galougahi K, Patel S, Shlofmitz RA, et al. Calcific plaque modification by acoustic shockwaves - intravascular lithotripsy in coronary interventions. Circ Cardiovasc Interv. 2021; 14:e009354. PMID: 32907343.29. Hatem R, Finn MT, Riley RF, et al. Zero contrast retrograde chronic total occlusions percutaneous coronary intervention: a case series. Eur Heart J Case Rep. 2018; 2:1–5.
Article30. Madhavan MV, Prasad M, Fall KN, Rahim H, Ali ZA. Zero-contrast multivessel revascularization for acute coronary syndrome in a patient with chronic kidney disease. JACC Case Rep. 2019; 1:774–780. PMID: 34316930.
Article31. Parviz Y, Fall K, Stone GW, et al. Imaging and physiology to guide venous graft interventions without contrast administration in advanced renal failure. J Invasive Cardiol. 2017; 29:E163–E165. PMID: 29086735.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Adequacy of Ambulatory Hemodynamic Assessments for Reducing All-Cause Mortality in Individuals With Heart Failure
- Bioengineering the Heart: Harnessing Biomaterials for Innovative Cardiovascular Interventions
- The Role of Distal Protection Devices for Cardiovascular Intervention
- Vascular Access: The Alpha and Omega of Cardiovascular Intervention
- RSV Prevention Strategies in Korean Children: A Review of Current Approaches and Emerging Options
