Elevated On-Treatment Diastolic Blood Pressure and Cardiovascular Outcomes in the Presence of Achieved Systolic Blood Pressure Targets
- Kim DH
 1
1 - Cho IJ2
- Kim W3
- Lee CJ4
- Kim HC4
- Shin JH5
- Kang SH6
- Jung MH7
- Kwon CH8
- Lee JH9
- Kim HL20
- Kim HM11
- Cho I4
- Kang DR12
- Lee HY13
- Chung WJ14
- Kim KI15
- Cho EJ16
- Sohn IS17
- Park S3
- Shin J18
- Ryu SK19
- Kang SM3
- Pyun WB2
- Cho MC9
- Kim JH20
- Lee JH21
- Ihm SH22
- Sung KC23
- Affiliations
-
- 1Division of Cardiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 2Division of Cardiology, Department of Internal Medicine, Ewha Womans University Seoul Hospital, College of Medicine, Ewha Womans University, Seoul, Korea
- 3Cardiovascular Center, Korea University Guro Hospital, Seoul, Korea
- 4Division of Cardiology, Severance Cardiovascular Hospital and Cardiovascular Research Institute, Yonsei University College of Medicine, Seoul, Korea
- 5Division of Cardiology, Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea
- 6Cardiovascular Center, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea
- 7Cardiovascular Center, Dongtan Sacred Heart Hospital, Hallym University College of Medicine, Hwaseong, Korea
- 8Division of Cardiology, Department of Internal Medicine, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea
- 9Division of Cardiology, Department of Internal Medicine, Chungbuk National University Hospital, Chungbuk National University College of Medicine, Cheongju, Korea
- 10Department of Internal Medicine, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul, Korea
- 11Division of Cardiology, Department of Internal Medicine, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul, Korea
- 12Department of Precision Medicine, Wonju College of Medicine, Yonsei University, Wonju, Korea
- 13Division of Cardiology, Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea
- 14Division of Cardiology, Department of Internal Medicine, Gil Hospital, Gachon University, Incheon, Korea
- 15Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea
- 16Division of Cardiology, Department of Internal Medicine, Yeouido St. Mary’s Hospital, The Catholic University of Korea, Seoul, Korea
- 17Division of Cardiology, Department of Internal Medicine, Kyung Hee University at Gangdong, Seoul, Korea
- 18Division of Cardiology, Department of Internal Medicine, College of Medicine, Hanyang University, Seoul, Korea
- 19Division of Cardiology, Department of Internal Medicine, Eulji Medical School of Medicine, Seoul, Korea
- 20Division of Cardiology, Department of Internal Medicine, Eulji Medical School of Medicine, Seoul, Korea
- 21Department of Biostatistics, Wonju College of Medicine, Yonsei University, Wonju, Korea
- 22Division of Cardiology, Department of Internal Medicine, Bucheon St. Mary’s Hospital, The Catholic University of Korea, Seoul, Korea
- 23Division of Cardiology, Department of Internal Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea
- KMID: 2530455
- DOI: http://doi.org/10.4070/kcj.2021.0330
Abstract
- Background and Objectives
This study aimed to investigate the association between cardiovascular events and 2 different levels of elevated on-treatment diastolic blood pressures (DBP) in the presence of achieved systolic blood pressure targets (SBP).
Methods
A nation-wide population-based cohort study comprised 237,592 patients with hypertension treated. The primary endpoint was a composite of cardiovascular death, myocardial infarction, and stroke. Elevated DBP was defined according to the Seventh Report of Joint National Committee (JNC7; SBP <140 mmHg, DBP ≥90 mmHg) or to the 2017 American College of Cardiology/American Heart Association (ACC/AHA) definitions (SBP <130 mmHg, DBP ≥80 mmHg).
Results
During a median follow-up of 9 years, elevated on-treatment DBP by the JNC7 definition was associated with an increased risk of the occurrence of primary endpoint compared with achieved both SBP and DBP (adjusted hazard ratio [aHR], 1.14; 95% confidence interval [CI], 1.05–1.24) but not in those by the 2017 ACC/AHA definition. Elevated ontreatment DBP by the JNC7 definition was associated with a higher risk of cardiovascular mortality (aHR, 1.42; 95% CI, 1.18–1.70) and stroke (aHR, 1.19; 95% CI, 1.08–1.30). Elevated on-treatment DBP by the 2017 ACC/AHA definition was only associated with stroke (aHR, 1.10; 95% CI, 1.04–1.16). Similar results were seen in the propensity-score-matched cohort.
Conclusion
Elevated on-treatment DBP by the JNC7 definition was associated a high risk of major cardiovascular events, while elevated DBP by the 2017 ACC/AHA definition was only associated with a higher risk of stroke. The result of study can provide evidence of DBP targets in subjects who achieved SBP targets.
Keyword
Figure
-
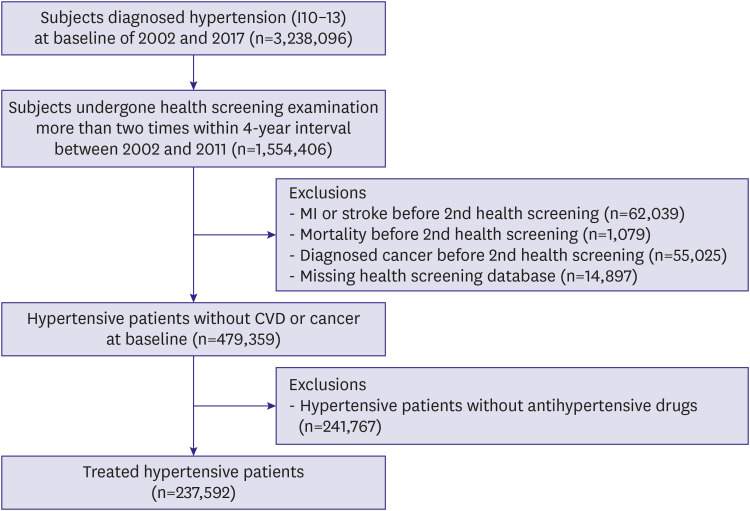
Figure 1 The flow chart of the study population.CVD = cardiovascular disease; MI = myocardial infarction.

Figure 2 Mortality and cardiovascular events in subjects with DBP target by either the JNC7 or the 2017 ACC/AHA definitions. (A) Total study population, (B) After propensity-score matching, and (C) Subgroup analysis for MACE in total study population.ACC = American College of Cardiology; AHA = American Heart Association; CI = confidence interval; DBP = diastolic blood pressure; HR = hazard ratio; JNC7 = The Seventh Report of Joint National Committee; MACE = major adverse cardiac event; MI = myocardial infarction.*The p value <0.05 for hazard ratio. Hazard ratio calculated by Cox proportional hazards regression analysis after adjustments for age, household income, smoking, physical activity, alcohol consumption, body mass index, fasting serum glucose and total cholesterol levels, diabetes mellitus, classes of antihypertensive medications, and Charlson Comorbidity Index.
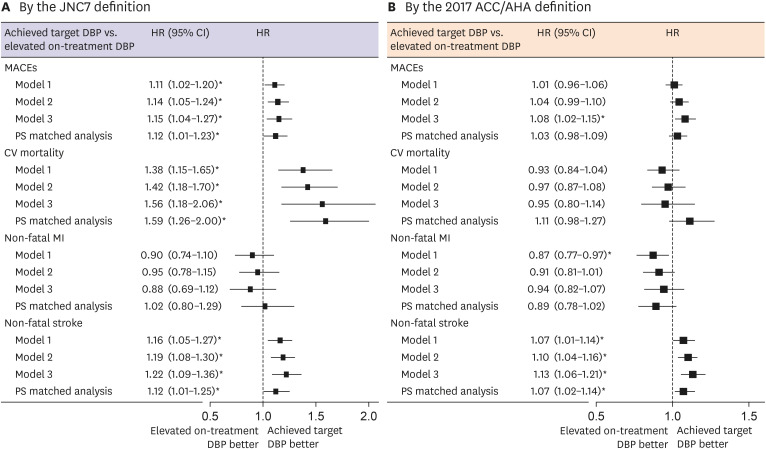
Figure 3 Associations between each endpoint and two different levels of elevated on-treatment DBPs in the presence of achieved SBPs, lowered by either the JNC7 or the 2017 ACC/AHA definition.Model 1 is adjusted for age and sex. Model 2 is adjusted for model 1+ household income, smoking, physical activity, alcohol consumption, body mass index, fasting serum glucose and total cholesterol levels, diabetes mellitus, use of aspirin or statin, classes of antihypertensive medications, and Charlson Comorbidity Index. Model 3 is adjusted for model 2 + time-varying systolic blood pressure.PS matched analysis is adjusted for age, household income, smoking, physical activity, alcohol consumption, body mass index, fasting serum glucose and total cholesterol levels, diabetes mellitus, use of aspirin or statin, classes of antihypertensive medications, and Charlson Comorbidity Index in propensity-score matched cohort.ACC = American College of Cardiology; AHA = American Heart Association; CI = confidence interval; DBP = diastolic blood pressure; HR = hazard ratio; JNC7 = The Seventh Report of Joint National Committee; MACE = major adverse cardiac event; MI = myocardial infarction; PS = propensity-score.*The p value <0.05 for hazard ratio.
Cited by 1 articles
-
On-Treatment Diastolic Blood Pressure: When Is It Too High?
Jin Joo Park
Korean Circ J. 2022;52(6):475-477. doi: 10.4070/kcj.2022.0126.
Reference
-
1. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: Executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018; 71:2199–2269. PMID: 29146533.2. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018; 39:3021–3104. PMID: 30165516.3. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002; 360:1903–1913. PMID: 12493255.
Article4. Yano Y, Reis JP, Tedla YG, et al. Racial differences in associations of blood pressure components in young adulthood with incident cardiovascular disease by middle age: Coronary Artery Risk Development in Young Adults (CARDIA) study. JAMA Cardiol. 2017; 2:381–389. PMID: 28199497.
Article5. Flint AC, Conell C, Ren X, et al. Effect of systolic and diastolic blood pressure on cardiovascular outcomes. N Engl J Med. 2019; 381:243–251. PMID: 31314968.
Article6. Zhang Y, Vittinghoff E, Pletcher MJ, et al. Associations of blood pressure and cholesterol levels during young adulthood with later cardiovascular events. J Am Coll Cardiol. 2019; 74:330–341. PMID: 31319915.
Article7. Thomopoulos C, Parati G, Zanchetti A. Effects of blood pressure lowering on outcome incidence in hypertension: 7. Effects of more vs. less intensive blood pressure lowering and different achieved blood pressure levels - updated overview and meta-analyses of randomized trials. J Hypertens. 2016; 34:613–622. PMID: 26848994.
Article8. Böhm M, Schumacher H, Teo KK, et al. Achieved diastolic blood pressure and pulse pressure at target systolic blood pressure (120-140 mmHg) and cardiovascular outcomes in high-risk patients: results from ONTARGET and TRANSCEND trials. Eur Heart J. 2018; 39:3105–3114. PMID: 29873709.
Article9. Franklin SS. The importance of diastolic blood pressure in predicting cardiovascular risk. J Am Soc Hypertens. 2007; 1:82–93. PMID: 20409835.
Article10. Petrovitch H, Curb JD, Bloom-Marcus E. Isolated systolic hypertension and risk of stroke in Japanese-American men. Stroke. 1995; 26:25–29. PMID: 7839392.
Article11. Strandberg TE, Salomaa VV, Vanhanen HT, Pitkälä K, Miettinen TA. Isolated diastolic hypertension, pulse pressure, and mean arterial pressure as predictors of mortality during a follow-up of up to 32 years. J Hypertens. 2002; 20:399–404. PMID: 11875306.
Article12. Hozawa A, Ohkubo T, Nagai K, et al. Prognosis of isolated systolic and isolated diastolic hypertension as assessed by self-measurement of blood pressure at home: the Ohasama study. Arch Intern Med. 2000; 160:3301–3306. PMID: 11088093.
Article13. Lee H, Yano Y, Cho SM, et al. Cardiovascular risk of isolated systolic or diastolic hypertension in young adults. Circulation. 2020; 141:1778–1786. PMID: 32479205.
Article14. Lee H, Yano Y, Cho SM, Park S, Lloyd-Jones DM, Kim HC. Cardiovascular risk of isolated diastolic hypertension defined by the 2017 American College of Cardiology/American Heart Association blood pressure guideline: a nationwide age-stratified cohort study. Hypertension. 2020; 76:e44–e46. PMID: 33070661.
Article15. McEvoy JW, Daya N, Rahman F, et al. Association of isolated diastolic hypertension as defined by the 2017 ACC/AHA blood pressure guideline with incident cardiovascular outcomes. JAMA. 2020; 323:329–338. PMID: 31990314.
Article16. Cheol Seong S, Kim YY, Khang YH, et al. Data Resource Profile: The National Health Information Database of the National Health Insurance Service in South Korea. Int J Epidemiol. 2017; 46:799–800. PMID: 27794523.
Article17. Seong SC, Kim YY, Park SK, et al. Cohort profile: the National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) in Korea. BMJ Open. 2017; 7:e016640.
Article18. Quan H, Li B, Couris CM, et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011; 173:676–682. PMID: 21330339.
Article19. Park TH, Choi JC. Validation of stroke and thrombolytic therapy in Korean National Health Insurance claim data. J Clin Neurol. 2016; 12:42–48. PMID: 26365022.
Article20. Bangalore S, Guo Y, Samadashvili Z, Blecker S, Xu J, Hannan EL. Everolimus-eluting stents or bypass surgery for multivessel coronary disease. N Engl J Med. 2015; 372:1213–1222. PMID: 25775087.
Article21. Mancia G. Blood pressure reduction and cardiovascular outcomes: past, present, and future. Am J Cardiol. 2007; 100:3J–9J.
Article22. Muntner P, Whelton PK. Using predicted cardiovascular disease risk in conjunction with blood pressure to guide antihypertensive medication treatment. J Am Coll Cardiol. 2017; 69:2446–2456. PMID: 28494981.
Article23. Yano Y, Stamler J, Garside DB, et al. Isolated systolic hypertension in young and middle-aged adults and 31-year risk for cardiovascular mortality: the Chicago Heart Association Detection Project in Industry study. J Am Coll Cardiol. 2015; 65:327–335. PMID: 25634830.
Article24. Choi YJ, Kim SH, Kang SH, et al. Reconsidering the cut-off diastolic blood pressure for predicting cardiovascular events: a nationwide population-based study from Korea. Eur Heart J. 2019; 40:724–731. PMID: 30535368.
Article25. Kannel WB, Gordon T, Schwartz MJ. Systolic versus diastolic blood pressure and risk of coronary heart disease. The Framingham study. Am J Cardiol. 1971; 27:335–346. PMID: 5572576.
Article26. Franklin SS, Larson MG, Khan SA, et al. Does the relation of blood pressure to coronary heart disease risk change with aging? The Framingham Heart Study. Circulation. 2001; 103:1245–1249. PMID: 11238268.
Article27. Fang J, Madhavan S, Cohen H, Alderman MH. Isolated diastolic hypertension. A favorable finding among young and middle-aged hypertensive subjects. Hypertension. 1995; 26:377–382. PMID: 7649569.28. Blank SG, Mann SJ, James GD, West JE, Pickering TG. Isolated elevation of diastolic blood pressure. Real or artifactual? Hypertension. 1995; 26:383–389. PMID: 7649570.
