Fecal microbiota transplantation for induction of remission, maintenance and rescue in patients with corticosteroid-dependent ulcerative colitis: a long-term follow-up real-world cohort study
- Affiliations
-
- 1Department of Gastroenterology and Hepatobiliary Sciences, Fortis Memorial Research Institute, Gurugram, India
- 2Department of Histopathology, Fortis Memorial Research Institute, Gurugram, India
- KMID: 2529571
- DOI: http://doi.org/10.5217/ir.2021.00069
Abstract
- Background/Aims
To study role of fecal microbiota transplantation (FMT) in induction, maintenance, and rescue in patients with corticosteroid-dependent ulcerative colitis (CDUC).
Methods
Patients with active CDUC received 3 fortnightly sessions of colonoscopic induction FMT (iFMT) in addition to standard of care. In patients who achieved clinical remission (CR) or response, prednisolone was tapered from week 4 and azathioprine from week 12. Responders were advised maintenance FMT (mFMT) every 6 months. Those with relapse were offered rescue FMT (rFMT), and low dose prednisolone was added if there was no improvement in 2 weeks.
Results
All 27 patients enrolled completed iFMT and were followed up for 39 months (range, 9–71 months). The mean Mayo score decreased from 6.4±2.5 at baseline to 2.6±3.7 at week 4, 2.6±3.4 at week 12, and 2.8±3.8 at week 24 (P<0.05). Corticosteroid-free CR and clinical response at week 12 were seen in 13 patients (48%) and 1 patient (3.7%), respectively. Corticosteroid and azathioprine-free CR at week 24 was seen in 13 patients (48%) and in them histological response was seen in 2 patients (15.2%) at week 4, 5 patients (38.4%) at week 12, and 10 patients (76.9%) at week 24. First relapse was seen in 10 of 13 responders (76.9%) at a median of 14.8 months (range, 6–34 months) after iFMT and was less frequent in patients on mFMT. Relapse was treated successfully with rFMT alone in 4 patients (40%) and rFMT with low dose steroids in 5 patients (50%).
Conclusions
iFMT, mFMT, and rFMT may have a role in treatment of selected patients with CDUC.
Figure
-
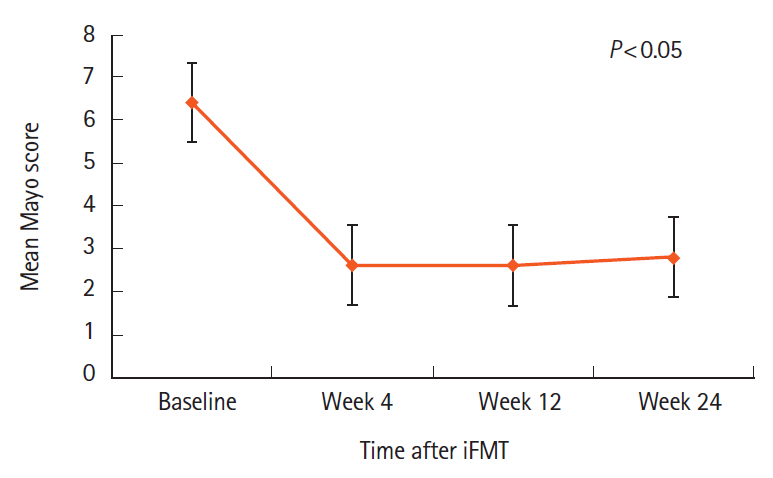
Fig. 1. Reduction in Mayo score after induction fecal microbiota transplantation (iFMT).
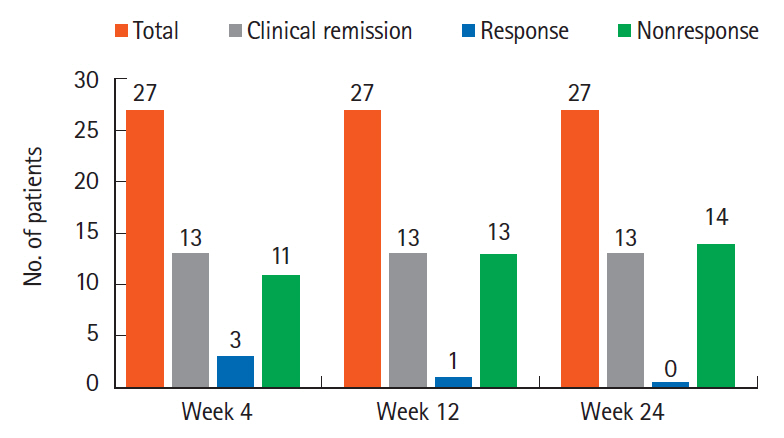
Fig. 2. Clinical remission and clinical response at weeks 4, 12, and 24 following induction fecal microbiota transplantation.
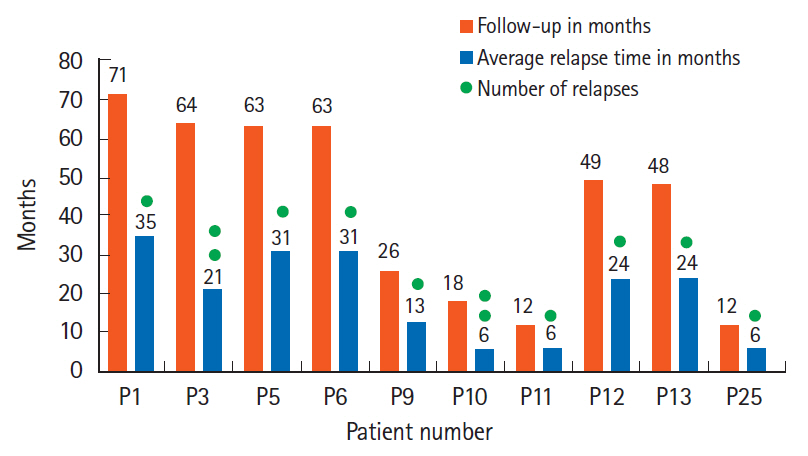
Fig. 3. Average relapse time and number of relapses in 10 out of 13 patients who achieved clinical remission at 24 weeks.
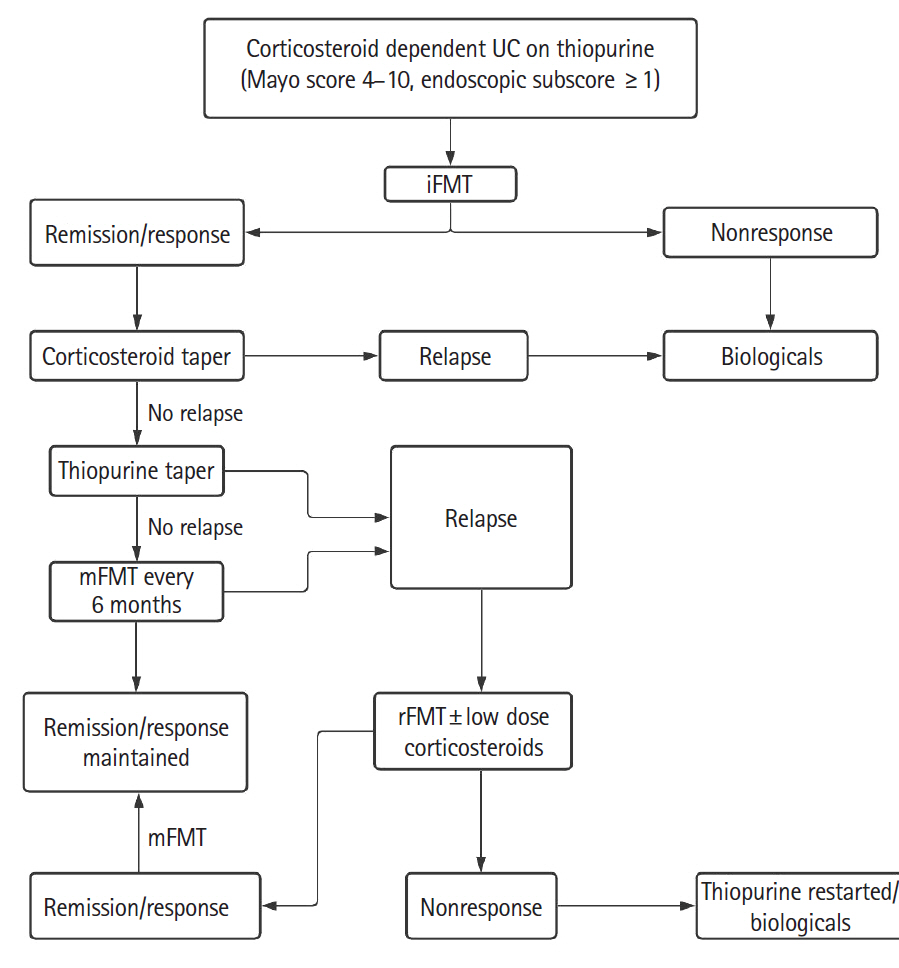
Fig. 4. Algorithm showing possible role of iFMT, mFMT, and rFMT in the treatment of corticosteroid dependent ulcerative colitis (UC) on thiopurines. FMT, fecal microbiota transplantation; iFMT, induction FMT; mFMT, maintenance FMT; rFMT, rescue FMT.
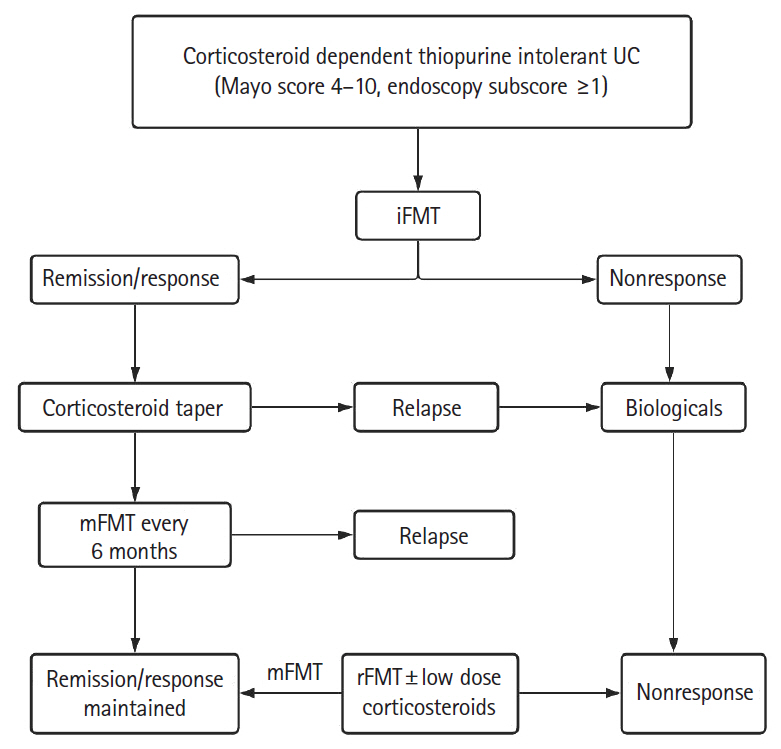
Fig. 5. Algorithm showing possible role of iFMT, mFMT and rFMT in the treatment of corticosteroid dependent ulcerative colitis (UC) who are thiopurine intolerant. FMT, fecal microbiota transplantation; iFMT, induction FMT; mFMT, maintenance FMT; rFMT, rescue FMT.

Cited by 1 articles
-
The practice of fecal microbiota transplantation in inflammatory bowel disease
Umang Arora, Saurabh Kedia, Vineet Ahuja
Intest Res. 2024;22(1):44-64. doi: 10.5217/ir.2023.00085.
Reference
-
1. Bejaoui M, Sokol H, Marteau P. Targeting the microbiome in inflammatory bowel disease: critical evaluation of current concepts and moving to new horizons. Dig Dis. 2015; 33 Suppl 1:105–112.
Article2. McDonald LC, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis. 2018; 66:e1–e48.3. Mcilroy JR, Nalagatla N, Hansen R, Hart A, Hold GL. Faecal microbiota transplantation as a treatment for inflammatory bowel disease: a national survey of adult and paediatric gastroenterologists in the UK. Frontline Gastroenterol. 2018; 9:250–255.
Article4. Lamb CA, Kennedy NA, Raine T, et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut. 2019; 68(Suppl 3):s1–s106.
Article5. Seth AK, Rawal P, Bagga R, Jain P. Successful colonoscopic fecal microbiota transplantation for active ulcerative colitis: first report from India. Indian J Gastroenterol. 2016; 35:393–395.
Article6. Seth AK, Jain P. Colonoscopic fecal microbiota transplantation for patients with ulcerative colitis with failure of 5-amino salicylates and dependence on corticosteroids and/or thiopurine intolerance: 30-month follow up of first pilot study in India. Indian J Gastroenterol. 2017; 36:S1–S105.7. Lennard-Jones JE. Classification of inflammatory bowel disease. Scand J Gastroenterol. 1989; 24:2–6.
Article8. Cammarota G, Ianiro G, Tilg H, et al. European consensus conference on faecal microbiota transplantation in clinical practice. Gut. 2017; 66:569–580.
Article9. Geboes K, Riddell R, Ost A, Jensfelt B, Persson T, Löfberg R. A reproducible grading scale for histological assessment of inflammation in ulcerative colitis. Gut. 2000; 47:404–409.
Article10. Moayyedi P, Surette MG, Kim PT, et al. Fecal microbiota transplantation induces remission in patients with active ulcerative colitis in a randomized controlled trial. Gastroenterology. 2015; 149:102–109.
Article11. Rossen NG, Fuentes S, van der Spek MJ, et al. Findings from a randomized controlled trial of fecal transplantation for patients with ulcerative colitis. Gastroenterology. 2015; 149:110–118.
Article12. Paramsothy S, Kamm MA, Kaakoush NO, et al. Multidonor intensive faecal microbiota transplantation for active ulcerative colitis: a randomised placebo-controlled trial. Lancet. 2017; 389:1218–1228.
Article13. Crothers J, Kassam Z, Smith M, et al. A double-blind, randomized, placebo-control pilot trial of fecal microbiota transplantation capsules from rationally selected donors in active ulcerative colitis. Gastroenterology. 2018; 154:S-1050–S-1051.14. Costello SP, Hughes PA, Waters O, et al. Effect of fecal microbiota transplantation on 8-week remission in patients with ulcerative colitis: a randomized clinical trial. JAMA. 2019; 321:156–164.
Article15. Costello SP, Soo W, Bryant RV, Jairath V, Hart AL, Andrews JM. Systematic review with meta-analysis: faecal microbiota transplantation for the induction of remission for active ulcerative colitis. Aliment Pharmacol Ther. 2017; 46:213–224.
Article16. Narula N, Kassam Z, Yuan Y, et al. Systematic review and meta-analysis: fecal microbiota transplantation for treatment of active ulcerative colitis. Inflamm Bowel Dis. 2017; 23:1702–1709.17. Lam WC, Zhao C, Ma WJ, Yao L. The clinical and steroid-free remission of fecal microbiota transplantation to patients with ulcerative colitis: a meta-analysis. Gastroenterol Res Pract. 2019; 2019:1287493.
Article18. Tang LL, Feng WZ, Cheng JJ, Gong YN. Clinical remission of ulcerative colitis after different modes of faecal microbiota transplantation: a meta-analysis. Int J Colorectal Dis. 2020; 35:1025–1034.
Article19. Sood A, Mahajan R, Juyal G, et al. Efficacy of fecal microbiota therapy in steroid dependent ulcerative colitis: a real world intention-to-treat analysis. Intest Res. 2019; 17:78–86.
Article20. Garza-González E, Mendoza-Olazarán S, Morfin-Otero R, et al. Intestinal microbiome changes in fecal microbiota transplant (FMT) vs. FMT enriched with Lactobacillus in the treatment of recurrent Clostridioides difficile infection. Can J Gastroenterol Hepatol. 2019; 2019:4549298.21. Sood A, Mahajan R, Singh A, et al. Role of faecal microbiota transplantation for maintenance of remission in patients with ulcerative colitis: a pilot study. J Crohns Colitis. 2019; 13:1311–1317.
Article22. Qazi T, Amaratunga T, Barnes EL, Fischer M, Kassam Z, Allegretti JR. The risk of inflammatory bowel disease flares after fecal microbiota transplantation: systematic review and metaanalysis. Gut Microbes. 2017; 8:574–588.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multi-session fecal microbiota transplantation using colonoscopy has favorable outcomes for the treatment of steroid-dependent ulcerative colitis
- Efficacy of fecal microbiota therapy in steroid dependent ulcerative colitis: a real world intention-to-treat analysis
- Fecal Microbiota Transplantation to Patients with Refractory Very Early Onset Ulcerative Colitis
- Coordinated Hospital-Home Fecal Microbiota Transplantation via Percutaneous Endoscopic Cecostomy for Recurrent Steroid-Dependent Ulcerative Colitis
- Failure of Fecal Microbiota Transplantation in a Three-Year-Old Child with Severe Refractory Ulcerative Colitis
