A case of autoimmune enteropathy with CTLA4 haploinsufficiency
- Miyazaki H
 1
1 - Hoshi N1
- Kohashi M1,2
- Tokunaga E1
- Ku Y1
- Takenaka H1
- Ooi M1
- Yamamoto N3
- Uemura S3
- Nishimura N4
- Iijima K3
- Jimbo K5
- Okano T6
- Hoshino A6
- Imai K7
- Kanegane H8
- Kobayashi I9
- Kodama Y1
- Affiliations
-
- 1Division of Gastroenterology, Department of Internal Medicine, Kobe University Hospital, Kobe, Japan
- 2Department of Gastroenterology, Kakogawa Central City Hospital, Kakogawa, Japan
- 3Department of Pediatrics, Kobe University Graduate School of Medicine, Kobe, Japan
- 4Department of Public Health, Kobe University Graduate School of Health Sciences, Kobe, Japan
- 5Department of Pediatrics, Juntendo University Faculty of Medicine, Tokyo, Japan
- 6Department of Pediatrics and Developmental Biology, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University (TMDU), Tokyo, Japan
- 7Department of Community Pediatrics, Perinatal and Maternal Medicine, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University (TMDU), Tokyo, Japan
- 8Department of Child Health and Development, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University (TMDU), Tokyo, Japan
- 9Center for Pediatric Allergy and Rheumatology, KKR Sapporo Medical Center, Sapporo, Japan
- KMID: 2525081
- DOI: http://doi.org/10.5217/ir.2020.00041
Abstract
- Autoimmune enteropathy (AIE) is a rare disease, characterized by intractable diarrhea, villous atrophy of the small intestine, and the presence of circulating anti-enterocyte autoantibodies. Immune dysregulation, polyendocrinopathy, enteropathy, X-linked (IPEX) syndrome, and mutations in FOXP3, which is a master gene of regulatory T cells (Tregs), are major causes of AIE. Recent studies have demonstrated that mutations in other Treg-associated genes, such as CD25 and CTLA4, show an IPEX-like phenotype. We present the case of a 13-year-old girl with CTLA4 haploinsufficiency, suffering from recurrent immune thrombocytopenic purpura and intractable diarrhea. We detected an autoantibody to the AIE-related 75 kDa antigen (AIE-75), a hallmark of the IPEX syndrome, in her serum. She responded well to a medium dose of prednisolone and a controlled dose of 6-mercaptopurine (6-MP), even after the cessation of prednisolone administration. Serum levels of the soluble interleukin-2 receptor and immunoglobulin G (IgG) were useful in monitoring disease activity during 6-MP therapy. In conclusion, autoimmune-mediated mechanisms, similar to the IPEX syndrome, may be involved in the development of enteropathy in CTLA4 haploinsufficiency. Treatment with 6-MP and monitoring of disease activity using serum levels of soluble interleukin-2 receptor and IgG is suggested for such cases.
Figure
-
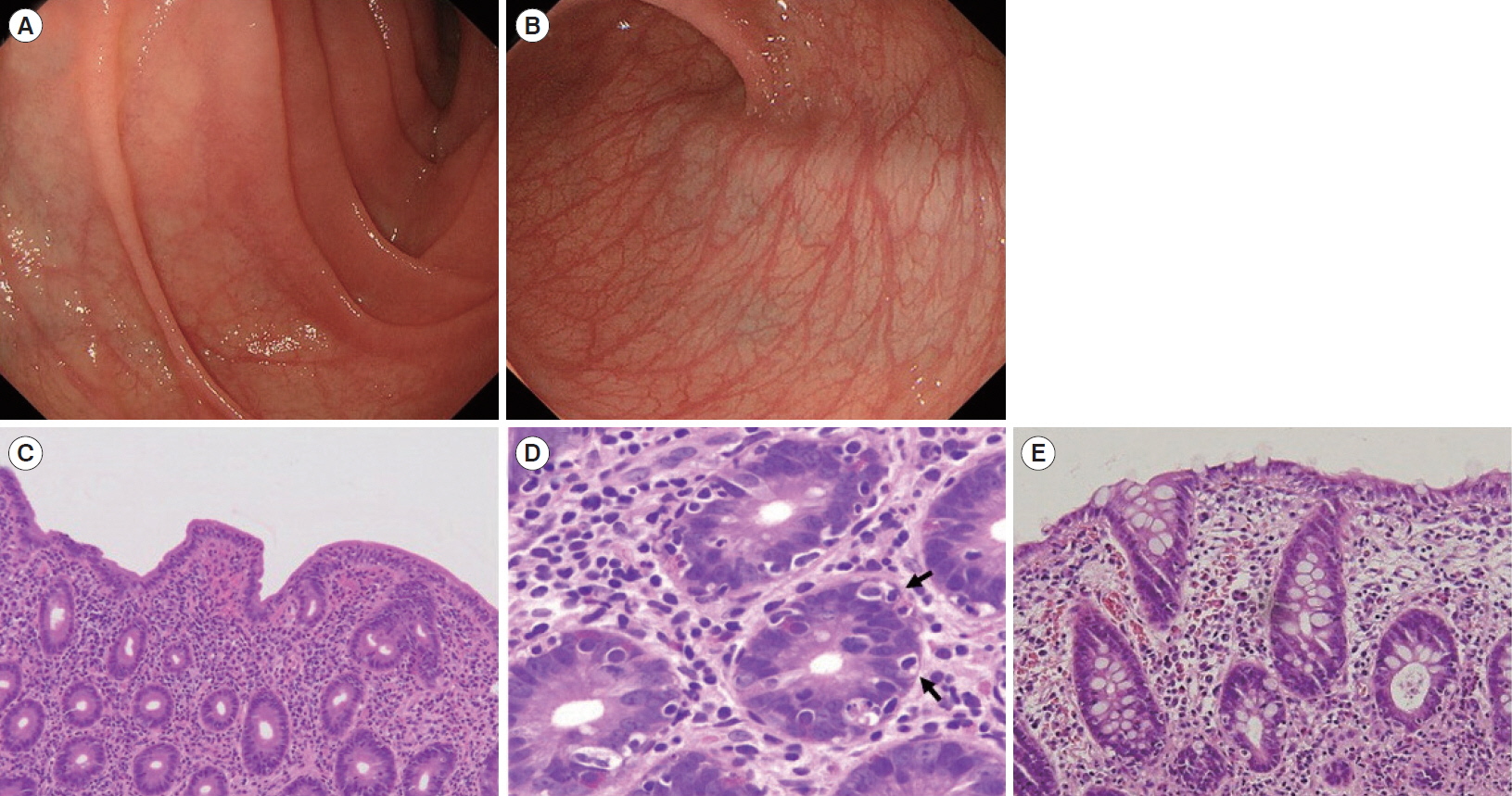
Fig. 1. Endoscopic and histopathological findings. Initial endoscopy showed villous atrophy of duodenum (A: duodenal second portion). Colon was intact endoscopically (B). Pathology of the duodenum demonstrated severe villous atrophy, infiltration of lymphocytes and plasma cells (C: H&E, ×4), and crypt apoptosis (arrows) (D: H&E, ×40). Pathology of the colon also showed infiltration of lymphocytes and plasma cells and crypt apoptosis (E: H&E, ×20).
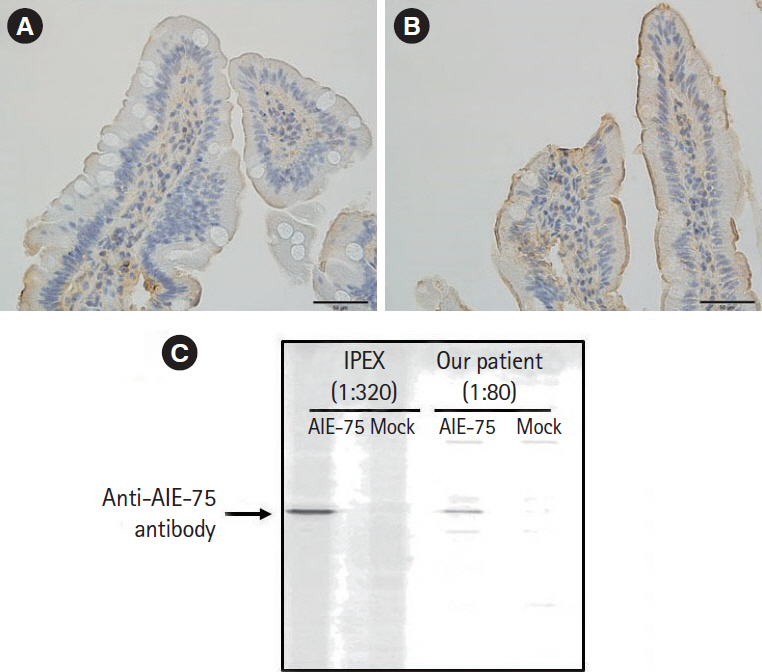
Fig. 2. Results of immunostaining and Western blotting. Immunostaining was performed using the serum of healthy donor (A) and our patient (B). Immunostaining of the normal small intestine tissue with the patient’s serum showed positive staining, which was seen as a thick band along the intestinal epithelium (×200). (C) Western blotting using our patient’s serum showed positive band. Serum from an immune dysregulation, polyendocrinopathy, enteropathy, X-linked (IPEX) patient with autoimmune enteropathy (AIE) was used as positive control.
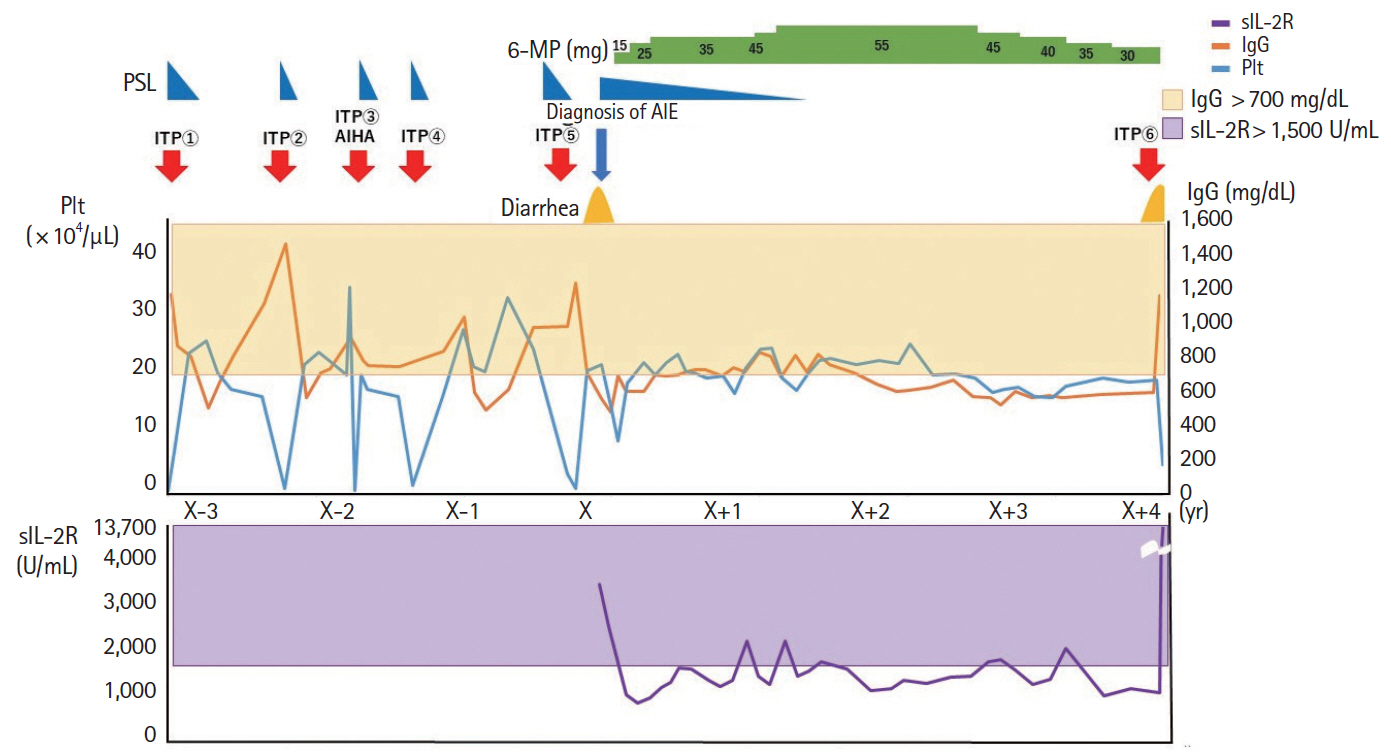
Fig. 3. The correlation of the platelet count, IgG levels, sIL2R levels, symptoms, dose of PSL and 6-MP. sIL-2 was not recorded before the onset of AIE. 6-MP, 6-mercaptopurine; AIE, autoimmune enteropathy; AIHA, autoimmune hemolytic anemia; IgG, immunoglobulin G; ITP, immune thrombocytopenic purpura; Plt, platelet count, PSL, prednisolone; sIL-2R, soluble interleukin-2 receptor.
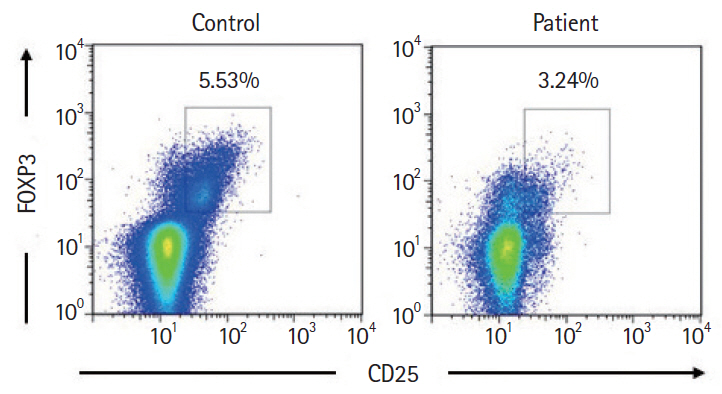
Fig. 4. Flow cytometry analysis. Expression of CD25+ FOXP3+ T cells gated on CD4+ T cells. CD4+ CD25+ FOXP3+ T cells in the patient were reduced than those in the control.
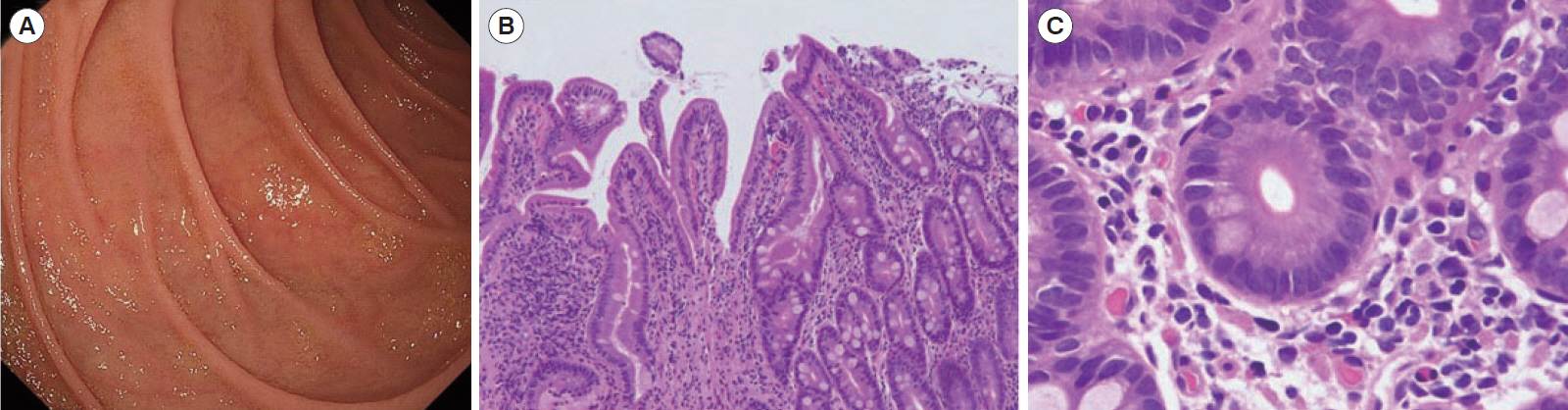
Fig. 5. Endoscopic and histopathological findings. Three years after the diagnosis, atrophy of the duodenum was improved (A: duodenal second portion). Villous atrophy also improved pathologically (B: H&E, ×4), and crypt apoptosis disappeared (C: H&E, ×40).
Reference
-
1. Unsworth DJ, Walker-Smith JA. Autoimmunity in diarrhoeal disease. J Pediatr Gastroenterol Nutr. 1985; 4:375–380.
Article2. Sakaguchi S. Naturally arising Foxp3-expressing CD25+CD4+ regulatory T cells in immunological tolerance to self and nonself. Nat Immunol. 2005; 6:345–352.
Article3. Barzaghi F, Amaya Hernandez LC, Neven B, et al. Long-term follow-up of IPEX syndrome patients after different therapeutic strategies: an international multicenter retrospective study. J Allergy Clin Immunol. 2018; 141:1036–1049.4. Kobayashi I, Imamura K, Kubota M, et al. Identification of an autoimmune enteropathy-related 75-kilodalton antigen. Gastroenterology. 1999; 117:823–830.
Article5. Kobayashi I, Kubota M, Yamada M, et al. Autoantibodies to villin occur frequently in IPEX, a severe immune dysregulation, syndrome caused by mutation of FOXP3. Clin Immunol. 2011; 141:83–89.
Article6. Schubert D, Bode C, Kenefeck R, et al. Autosomal dominant immune dysregulation syndrome in humans with CTLA4 mutations. Nat Med. 2014; 20:1410–1416.
Article7. Kuehn HS, Ouyang W, Lo B, et al. Immune dysregulation in human subjects with heterozygous germline mutations in CTLA4. Science. 2014; 345:1623–1627.8. Gambineri E, Ciullini Mannurita S, Hagin D, et al. Clinical, immunological, and molecular heterogeneity of 173 patients with the phenotype of immune dysregulation, polyendocrinopathy, enteropathy, X-linked (IPEX) syndrome. Front Immunol. 2018; 9:2411.
Article9. Singhi AD, Goyal A, Davison JM, Regueiro MD, Roche RL, Ranganathan S. Pediatric autoimmune enteropathy: an entity frequently associated with immunodeficiency disorders. Mod Pathol. 2014; 27:543–553.
Article10. Kanegane H, Hoshino A, Okano T, et al. Flow cytometry-based diagnosis of primary immunodeficiency diseases. Allergol Int. 2018; 67:43–54.
Article11. Schwab C, Gabrysch A, Olbrich P, et al. Phenotype, penetrance, and treatment of 133 cytotoxic T-lymphocyte antigen 4-insufficient subjects. J Allergy Clin Immunol. 2018; 142:1932–1946.
Article12. Greil C, Roether F, La Rosée P, Grimbacher B, Duerschmied D, Warnatz K. Rescue of cytokine storm due to hlh by hemoadsorption in a CTLA4-deficient patient. J Clin Immunol. 2017; 37:273–276.
Article13. Masia R, Peyton S, Lauwers GY, Brown I. Gastrointestinal biopsy findings of autoimmune enteropathy: a review of 25 cases. Am J Surg Pathol. 2014; 38:1319–1329.14. Sansom DM, Walker LS. The role of CD28 and cytotoxic T-lymphocyte antigen-4 (CTLA-4) in regulatory T-cell biology. Immunol Rev. 2006; 212:131–148.
Article15. Wing K, Onishi Y, Prieto-Martin P, et al. CTLA-4 control over Foxp3+ regulatory T cell function. Science. 2008; 322:271–275.
Article16. Chida N, Kobayashi I, Takezaki S, et al. Disease specificity of anti-tryptophan hydroxylase-1 and anti-AIE-75 autoantibodies in APECED and IPEX syndrome. Clin Immunol. 2015; 156:36–42.
Article17. Bertrand A, Kostine M, Barnetche T, Truchetet ME, Schaeverbeke T. Immune related adverse events associated with antiCTLA-4 antibodies: systematic review and meta-analysis. BMC Med. 2015; 13:211.
Article18. Adler BL, Pezhouh MK, Kim A, et al. Histopathological and immunophenotypic features of ipilimumab-associated colitis compared to ulcerative colitis. J Intern Med. 2018; 283:568–577.
Article19. Cuffari C, Hunt S, Bayless T. Utilisation of erythrocyte 6-thioguanine metabolite levels to optimise azathioprine therapy in patients with inflammatory bowel disease. Gut. 2001; 48:642–646.
Article20. D’Halluin PN, Tribut O, Branger B, et al. RBC 6-TGN and hematological parameters in patients with Crohn’s disease treated by azathioprine. Gastroenterol Clin Biol. 2005; 29:1264–1269.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Autoimmune Enteropathy Treated with Corticosteroid and FK506
- A Case of Primary Sjogren's Syndrome with Protein-losing Enteropathy
- Polymorphism of CTLA4 Gene in Schizophrenia
- CTLA4 expression profiles and their association with clinical outcomes of breast cancer: a systemic review
- A case of systemic lupus erythematosus with chylothorax, chronic interstitial cystitis and protein-losing enteropathy
