Incidence of Infection among Subjects with Helicobacter pylori Seroconversion
- Affiliations
-
- 1Department of Internal Medicine, Konkuk University School of Medicine, Seoul, Korea
- 2Department of Internal Medicine, Chonnam University School of Medicine, Gwangju, Korea
- KMID: 2525052
- DOI: http://doi.org/10.5946/ce.2020.299
Abstract
- Background/Aims
Helicobacter pylori (H. pylori) seroconversion may occur during screening for gastric cancer. Our study aimed to assess the number of seroconverted subjects with H. pylori and their results in follow-up tests.
Methods
Data were consecutively collected on subjects who were H. pylori-seronegative and presented for gastric cancer screening. Subjects who were followed up using the same serology test and pepsinogen (PG) assays on the day of endoscopy were included in the study.
Results
During the follow-up of 57.7 ± 21.4 months, 61 (15.0%) of 407 seronegative subjects showed seroconversion. H. pylori infection was detected in six (9.8%) of 61 seroconverted subjects. A diffuse red fundal appearance, with a significant increase in the Kyoto classification scores for gastritis, was observed in the infected subjects (p<0.001). Compared to the false-seropositive subjects, infected subjects showed higher serology titers (p<0.001) and PG II levels (p<0.001), and lower PG I/II ratios (p=0.002), in the follow-up tests.
Conclusions
Seroconversion occurred in 3.3% of seronegative subjects per year; however, only 9.8% had H. pylori infection. The majority (90.2%) of the seroconverted subjects showed false seropositivity without significant changes in the follow-up test results. The diffuse red fundal appearance could be an indicator of H. pylori infection.
Figure
-

Fig. 1. Flowchart of this study. A total of 407 consecutive Helicobacter pylori (H. pylori)-seronegative subjects were included in our study. During the mean follow-up period of 57.7±21.4 months, 61 subjects showed seroconversion; meanwhile, seronegative results persisted in 346 subjects. H. pylori infection was observed in six (9.8%) of 61 seroconverted subjects.
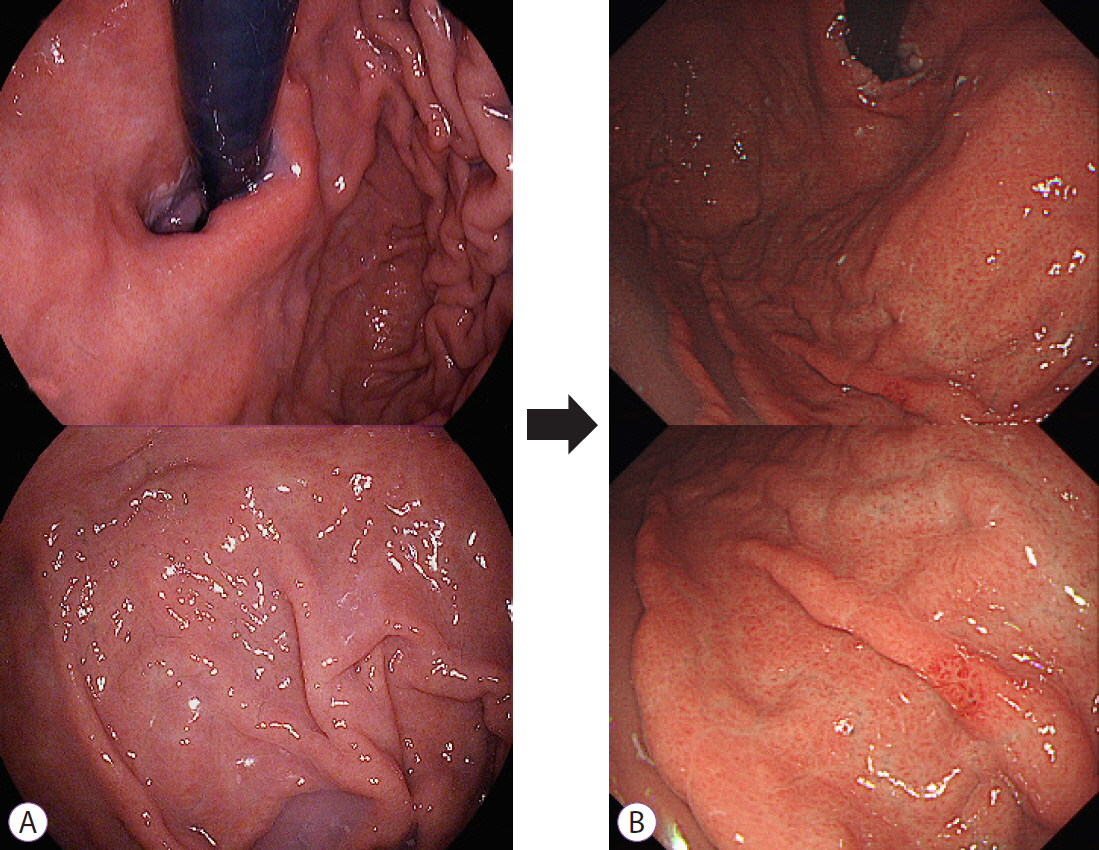
Fig. 2. Development of diffuse red fundal appearance on follow-up endoscopy in an Helicobacter pylori (H. pylori)-naïve subject with new infection. (A) Initial endoscopic findings of the fundus and cardia. The Kyoto classification score was 0 (A0, IM0, H0, N0 DR0). Serum pepsinogen (PG) and serology assays showed normal results, as summarized in Table 2. (B) Findings of follow-up endoscopy performed after four years. Multiple tiny hemorrhagic spots were observed in the fundus with positive Giemsa staining. The Kyoto classification score increased from 0 to 2 (A0 IM0 H0 N0 DR2). Seroconversion in H. pylori antibodies (6.4 → 21.7 AU/mL) was reported with higher serum PG I (69.5 → 85.1 ng/ml) and PG II (18.9 → 22.5 ng/ml) levels compared to the initial test findings.
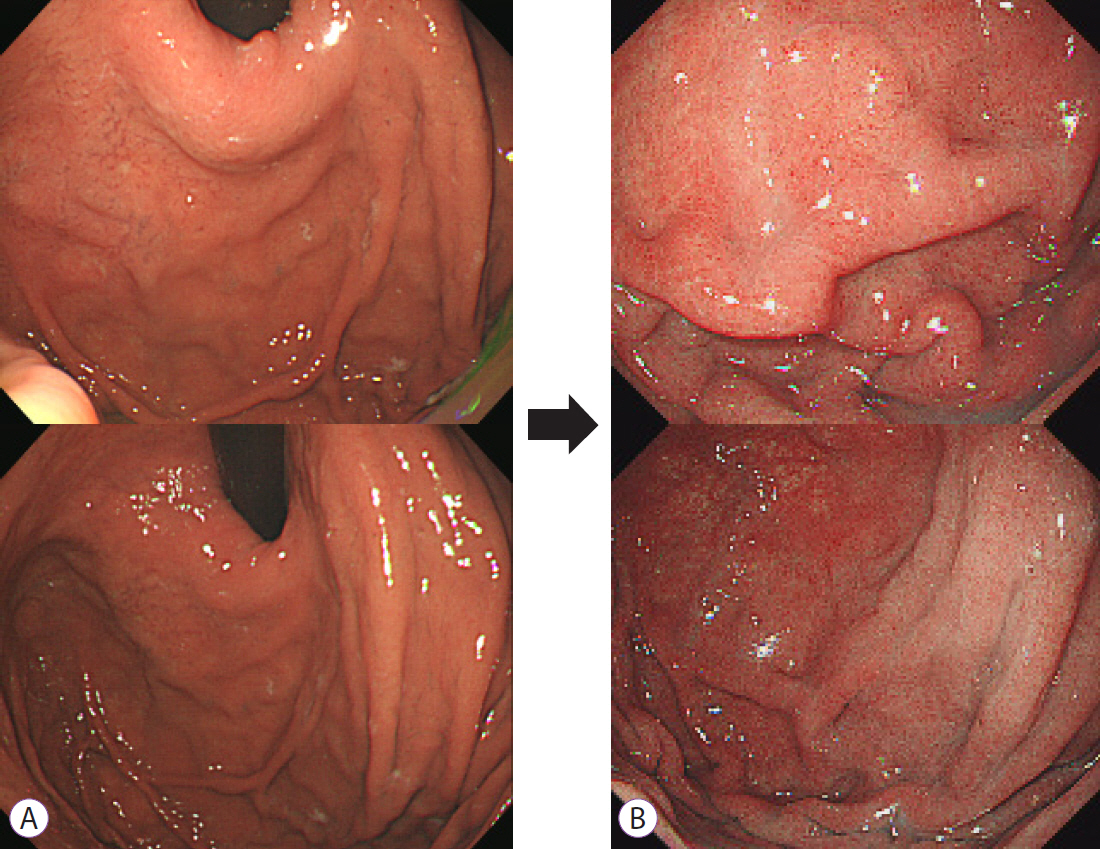
Fig. 3. Changes in the endoscopic findings of a subject who had a history of successful eradication four years prior to the initial visit. (A) Endoscopic findings of the fundus at the initial visit. The Kyoto classification score was 3 (A1 IM2 H0 N0 DR0). Successful eradication was confirmed by negative 13C-urea breath test findings. (B) Findings of follow-up endoscopy performed after six years. The development of diffuse red fundal appearance and positive Giemsa staining were observed. The Kyoto classification score increased from 3 to 5 (A1 IM2 H0 N0 DR2) with seroconversion (9.4 → 161.5 AU/mL). The serum pepsinogen (PG) I (46.4 → 97.2 ng/ml) and PG II (10.3 → 29.8 ng/ml) levels were higher compared to the initial test results, whereas the PG I/II ratio was lower (4.5 → 3.3).
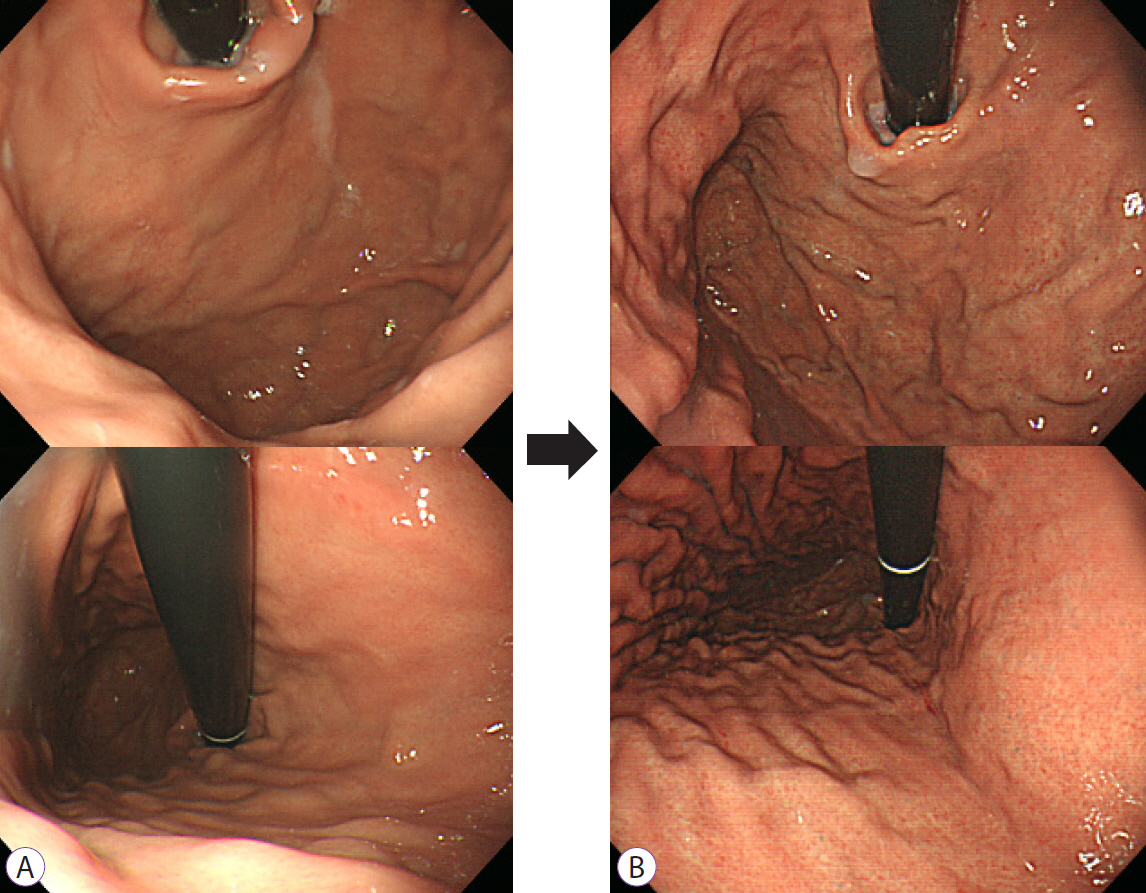
Fig. 4. Findings of initial and follow-up endoscopy in a subject with unintended eradication prior to the initial visit. (A) Initial endoscopic findings of the fundus. Unintended eradication of Helicobacter pylori was considered in this study since intestinal metaplasia was observed in the biopsied specimens obtained from the antrum. Serum pepsinogen and serology assays showed normal findings, and the Kyoto classification score was 1 (A0, IM1, H0, N0, DR0). (B) Follow-up endoscopy performed after four years revealed diffuse red fundal appearance and enlarged gastric pit openings in the fundus. Positive Giemsa staining results were obtained with seroconversion (<5 → 158.1). The Kyoto gastritis classification score increased to two (A0 IM1 H0 N0 DR1).
Cited by 1 articles
-
위바닥샘형 선암의 내시경 절제에 대한 증례 시리즈
Hwa Jin Lee, Gwang Ha Kim, Dong Chan Joo, Moon Won Lee, Bong Eun Lee, Kyungbin Kim
Korean J Gastroenterol. 2023;81(6):259-264. doi: 10.4166/kjg.2023.019.
Reference
-
1. Shin CM, Kim N, Lee HS, et al. Validation of diagnostic tests for Helicobacter pylori with regard to grade of atrophic gastritis and/or intestinal metaplasia. Helicobacter. 2009; 14:512–519.2. Kim JH, Lee SY, Lee SP, et al. The histologic detection of Helicobacter pylori in seropositive subjects is affected by pathology and secretory ability of the stomach. Helicobacter. 2018; 23:e12480.3. Tu H, Sun L, Dong X, et al. Serum anti-Helicobacter pylori immunoglobulin G titer correlates with grade of histological gastritis, mucosal bacterial density, and levels of serum biomarkers. Scand J Gastroenterol. 2014; 49:259–266.4. Bosch DE, Krumm N, Wener MH, et al. Serology is more sensitive than urea breath test or stool antigen for the initial diagnosis of Helicobacter pylori gastritis when compared with histopathology. Am J Clin Pathol. 2020; 154:255–265.5. Lee SP, Lee SY, Kim JH, Sung IK, Park HS, Shim CS. Link between serum pepsinogen concentrations and upper gastrointestinal endoscopic findings. J Korean Med Sci. 2017; 32:796–802.6. Kwon H, Lee SY, Kim JH, et al. ABC classification is less useful for older Koreans born before 1960. Gut Liver. 2019; 13:522–530.7. Kishino T, Oyama T, Tomori A, Takahashi A, Shinohara T. Usefulness and limitations of a serum screening system to predict the risk of gastric cancer. Intern Med. 2020; 59:1473–1480.8. Yoshii S, Mabe K, Watano K, et al. Validity of endoscopic features for the diagnosis of Helicobacter pylori infection status based on the Kyoto classification of gastritis. Dig Endosc. 2020; 32:74–83.9. Jung JH, Choi KD, Han S, et al. Seroconversion rates of Helicobacter pylori infection in Korean adults. Helicobacter. 2013; 18:299–308.10. Choi HS, Lee SY, Kim JH, et al. Combining the serum pepsinogen level and Helicobacter pylori antibody test for predicting the histology of gastric neoplasm. J Dig Dis. 2014; 15:293–298.11. Kim GH. Endoscopic findings of Kyoto classification of gastritis. Korean J Helicobacter Up Gastrointest Res. 2019; 19:88–93.12. Han HS, Lee SY, Oh SY, Moon HW, Cho H, Kim JH. Correlations of the gastric and duodenal microbiota with histological, endoscopic, and symptomatic gastritis. J Clin Med. 2019; 8:312.13. Sugimoto M, Ban H, Ichikawa H, et al. Efficacy of the Kyoto classification of gastritis in identifying subjects at high risk for gastric cancer. Intern Med. 2017; 56:579–586.14. Lee SY, Moon HW, Hur M, Yun YM. Validation of western Helicobacter pylori IgG antibody assays in Korean adults. J Med Microbiol. 2015; 64:513–518.15. Seo TH, Lee SY, Uchida T, et al. The origin of non-Helicobacter pylori-related positive Giemsa stain in human gastric biopsy specimens. Dig Liver Dis. 2011; 43:23–27.16. Inoue M, Sawada N, Goto A, JPHC Study Group, et al. High-negative anti-Helicobacter pylori IgG antibody titers and long-term risk of gastric cancer: Results from a large-scale population-based cohort study in Japan. Cancer Epidemiol Biomarkers Prev. 2020; 29:420–426.17. Lee JH, Kim N, Chung JI, et al. Long-term follow up of Helicobacter pylori IgG serology after eradication and reinfection rate of H. pylori in South Korea. Helicobacter. 2008; 13:288–294.18. Massarrat S, Haj-Sheykholeslami A, Mohamadkhani A, et al. Pepsinogen II can be a potential surrogate marker of morphological changes in corpus before and after H. pylori eradication. Biomed Res Int. 2014; 2014:481607.19. Shan J, Lei H, Shi W, Sun X, Tang Y, Ren C. High serum pepsinogen I and beta Helicobacter pylori infection are risk factors for aspirin-induced gastroduodenal injury. Dig Dis. 2018; 36:66–71.20. Noh G, Kim N, Choi Y, et al. Long-term follow up of serum pepsinogens in subjects with gastric cancer or dysplasia after Helicobacter pylori eradication. J Gastroenterol Hepatol. 2020; 35:1540–1548.21. Iijima K, Koike T, Ara N, et al. Identification of a high-risk group for low-dose aspirin-induced gastropathy by measuring serum pepsinogen in H. pylori-infected subjects. J Gastroenterol. 2015; 50:305–312.22. Song HJ, Jang SJ, Yun SC, et al. Low levels of pepsinogen I and pepsinogen I/II ratio are valuable serologic markers for predicting extensive gastric corpus atrophy in patients undergoing endoscopic mucosectomy. Gut Liver. 2010; 4:475–480.23. Lee SY. Helicobacter pylori-negative gastric cancer. Korean J Helicobacter Up Gastrointest Res. 2020; 21:10–21.24. Kato M, Terao S, Adachi K, Study Group for Establishing Endoscopic Diagnosis of Chronic Gastritis, et al. Changes in endoscopic findings of gastritis after cure of H.pylori infection: multicenter prospective trial. Dig Endosc. 2013; 25:264–273.25. Kato T, Yagi N, Kamada T, Shimbo T, Watanabe H, Ida K; Study Group for Establishing Endoscopic Diagnosis of Chronic Gastritis. Diagnosis of Helicobacter pylori infection in gastric mucosa by endoscopic features: a multicenter prospective study. Dig Endosc. 2013; 25:508–518.26. Toyoshima O, Nishizawa T, Arita M, et al. Helicobacter pylori infection in subjects negative for high titer serum antibody. World J Gastroenterol. 2018; 24:1419–1428.27. Otani K, Watanabe T, Kosaka S, et al. Utility of Kyoto classification of gastritis in subjects with a high-negative titer of anti-Helicobacter pylori antibody during a medical check-up. J Clin Biochem Nutr. 2020; 67:317–322.28. Toyoshima O, Nishizawa T, Yoshida S, et al. Endoscopy-based Kyoto classification score of gastritis related to pathological topography of neutrophil activity. World J Gastroenterol. 2020; 26:5146–5155.29. Nishizawa T, Sakitani K, Suzuki H, et al. A combination of serum anti-Helicobacter pylori antibody titer and Kyoto classification score could provide a more accurate diagnosis of H. pylori. United European Gastroenterol J. 2019; 7:343–348.30. Osawa H, Miura Y, Takezawa T, et al. Linked color imaging and blue laser imaging for upper gastrointestinal screening. Clin Endosc. 2018; 51:513–526.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Helicobacter pylori Infection and Cardiovascular Disease
- Treatment of Helicobacter pylori infection
- Treatment of Helicobacter pylori infection in functional dyspepsia
- Serological Changes after Equivocal Helicobacter pylori-serology Test Findings Dependent on Gastric Secreting Ability
- Indications for Helicobacter pylori Eradication Therapy
