Ann Rehabil Med.
2021 Oct;45(5):359-367. 10.5535/arm.21124.
Post-stroke Hyperglycemia in Non-diabetic Ischemic Stroke is Related With Worse Functional Outcome: A Cohort Study
- Affiliations
-
- 1Department of Rehabilitation Medicine, Pusan National University School of Medicine and Biomedical Research Institute, Pusan National University Hospital, Busan,
- 22Department of Rehabilitation Medicine, Pusan National University Yangsan Hospital, Pusan National University College of Medicine, Yangsan, Korea
- 3Department and Research Institute of Rehabilitation Medicine, Yonsei University College of Medicine, Seoul, Korea
- 4Department of Rehabilitation Medicine, Chungnam National University School of Medicine, Daejeon, Korea
- 5Department of Rehabilitation Medicine, Konkuk University School of Medicine, Seoul, Korea
- 6Department of Physical and Rehabilitation Medicine, Chonnam National University Medical School, Gwangju, Korea
- 7Department of Rehabilitation Medicine, Kyungpook National University College of Medicine, Daegu, Korea
- 8Department of Rehabilitation Medicine, Jeju National University Hospital, Jeju University College of Medicine, Jeju, Korea
- 9Department of Rehabilitation Medicine, Wonkwang University School of Medicine, Iksan, Korea
- 10Department of Physical and Rehabilitation Medicine, Center for Prevention and Rehabilitation, Heart Vascular and Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- KMID: 2521908
- DOI: http://doi.org/10.5535/arm.21124
Abstract
Objective
To investigate long-term and serial functional outcomes in ischemic stroke patients without diabetes with post-stroke hyperglycemia.
Methods
The Korean Stroke Cohort for Functioning and Rehabilitation (KOSCO) is a large, multi-center, prospective cohort study of stroke patients admitted to participating hospitals in nine areas of Korea. From KOSCO, ischemic stroke patients without diabetes were recruited and divided into two groups: patients without diabetes without (n=779) and with post-stroke hyperglycemia (n=223). Post-stroke hyperglycemia was defined as a glucose level >8 mmol/L. Functional assessments were performed 7 days and 3, 6, and 12 months after stroke onset.
Results
There were no significant differences in baseline characteristics between the groups, except in the age of onset and smoking. Analysis of the linear correlation between the initial National Institutes of Health Stroke Scale (NIHSS) score and glucose level showed no significant difference. Among our functional assessments, NIHSS, Fugl-Meyer Assessment (affected side), Functional Ambulatory Category, modified Rankin Scale, and Korean Mini-Mental State Examination (K-MMSE) showed statistically significant improvements in each group. All functional improvements except K-MMSE were significantly higher in patients without post-stroke hyperglycemia at 7 days and 3, 6, and 12 months.
Conclusion
The glucose level of ischemic stroke patients without diabetes had no significant correlation with the initial NIHSS score. The long-term effects of stress hyperglycemia showed worse functional outcomes in ischemic stroke patients without diabetes with post-stroke hyperglycemia.
Figure
-

Fig. 1. Flow diagram of this study. KOSCO, Korean Stroke Cohort for Functioning and Rehabilitation; IGT, impaired glucose tolerance; HbA1c, glycated hemoglobin.
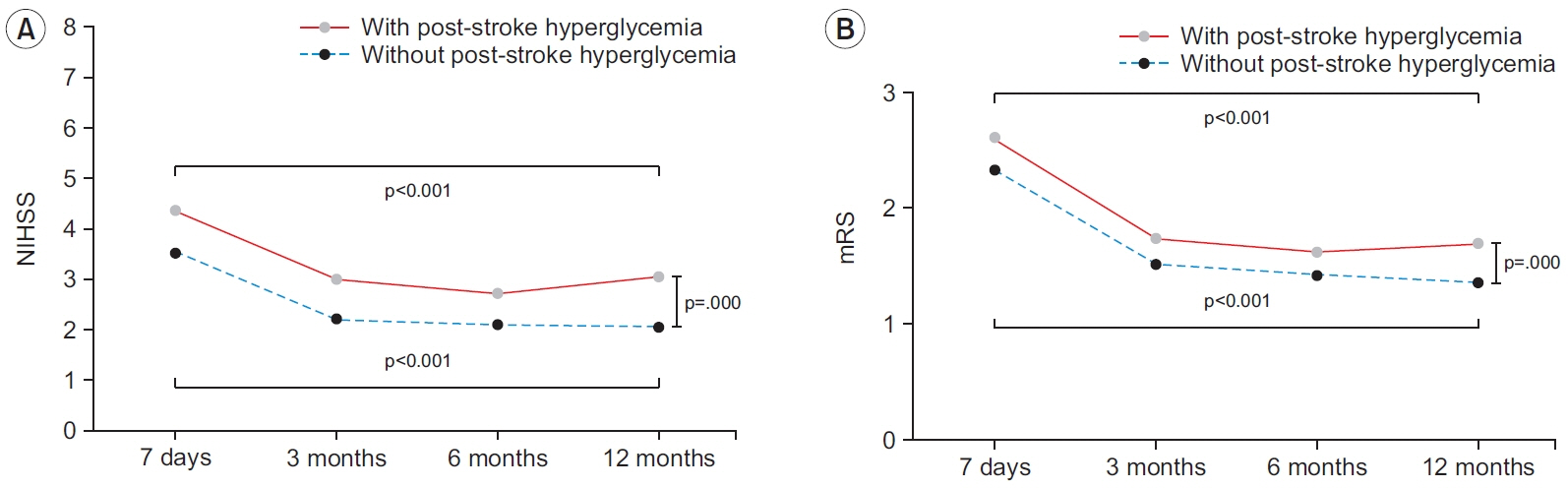
Fig. 2. Comparison of (A) National Institutes of Health Stroke Scale (NIHSS) and (B) modified Rankin Scale (mRS) between the group with or without post-stroke hyperglycemia in non-diabetic ischemic stroke patients.
Cited by 1 articles
-
A Path to Precision Medicine: Incorporating Blood-Based Biomarkers in Stroke Rehabilitation
Byung-Mo Oh
Ann Rehabil Med. 2021;45(5):341-344. doi: 10.5535/arm.21171.
Reference
-
1. Gisselsson L, Smith ML, Siesjo BK. Hyperglycemia and focal brain ischemia. J Cereb Blood Flow Metab. 1999; 19:288–97.
Article2. Kiers L, Davis SM, Larkins R, Hopper J, Tress B, Rossiter SC, et al. Stroke topography and outcome in relation to hyperglycaemia and diabetes. J Neurol Neurosurg Psychiatry. 1992; 55:263–70.
Article3. Alvarez-Sabin J, Molina CA, Montaner J, Arenillas JF, Huertas R, Ribo M, et al. Effects of admission hyperglycemia on stroke outcome in reperfused tissue plasminogen activator: treated patients. Stroke. 2003; 34:1235–41.4. Paolino AS, Garner KM. Effects of hyperglycemia on neurologic outcome in stroke patients. J Neurosci Nurs. 2005; 37:130–5.
Article5. Montori VM, Bistrian BR, McMahon MM. Hyperglycemia in acutely ill patients. JAMA. 2002; 288:2167–9.
Article6. McCowen KC, Malhotra A, Bistrian BR. Stress-induced hyperglycemia. Crit Care Clin. 2001; 17:107–24.
Article7. Weil ZM. Ischemia-induced hyperglycemia: consequences, neuroendocrine regulation, and a role for RAGE. Horm Behav. 2012; 62:280–5.
Article8. Parsons MW, Barber PA, Desmond PM, Baird TA, Darby DG, Byrnes G, et al. Acute hyperglycemia adversely affects stroke outcome: a magnetic resonance imaging and spectroscopy study. Ann Neurol. 2002; 52:20–8.
Article9. Capes SE, Hunt D, Malmberg K, Pathak P, Gerstein HC. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: a systematic overview. Stroke. 2001; 32:2426–32.10. Capes SE, Hunt D, Malmberg K, Gerstein HC. Stress hyperglycaemia and increased risk of death after myocardial infarction in patients with and without diabetes: a systematic overview. Lancet. 2000; 355:773–8.
Article11. Auer RN. Insulin, blood glucose levels, and ischemic brain damage. Neurology. 1998; 51(3 Suppl 3):S39–43.
Article12. Bruno A, Durkalski VL, Hall CE, Juneja R, Barsan WG, Janis S, et al. The Stroke Hyperglycemia Insulin Network Effort (SHINE) trial protocol: a randomized, blinded, efficacy trial of standard vs. intensive hyperglycemia management in acute stroke. Int J Stroke. 2014; 9:246–51.
Article13. Yoon JA, Kim DY, Sohn MK, Lee J, Lee SG, Lee YS, et al. Effect of stress hyperglycemia and intensive rehabilitation therapy in non-diabetic hemorrhagic stroke: Korean Stroke Cohort for Functioning and Rehabilitation. Eur J Neurol. 2016; 23:1658–65.
Article14. Davidson MB. How do we diagnose diabetes and measure blood glucose control? View 1: (Diagnosing) a clinical basis for the diagnosis of diabetes. Diabetes Spectr. 2001; 14:67–71.15. Goldstein LB, Adams R, Alberts MJ, Appel LJ, Brass LM, Bushnell CD, et al. Primary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council. Stroke. 2006; 37:1583–633.16. Bernardini J, Callen S, Fried L, Piraino B. Inter-rater reliability and annual rescoring of the Charlson comorbidity index. Adv Perit Dial. 2004; 20:125–7.17. Oh MS, Yu KH, Lee JH, Jung S, Ko IS, Shin JH, et al. Validity and reliability of a Korean version of the national institutes of health stroke scale. J Clin Neurol. 2012; 8:177–83.
Article18. Amarenco P, Bogousslavsky J, Caplan LR, Donnan GA, Hennerici MG. Classification of stroke subtypes. Cerebrovasc Dis. 2009; 27:493–501.
Article19. Gray CS, French JM, Bates D, Cartlidge NE, Venables GS, James OF. Increasing age, diabetes mellitus and recovery from stroke. Postgrad Med J. 1989; 65:720–4.
Article20. Kang Y, Na DL, Hahn S. A validity study on the Korean Mini-Mental State Examination (K-MMSE) in dementia patients. J Korean Neurol Assoc. 1997; 15:300–8.21. Fugl-Meyer AR, Jaasko L, Leyman I, Olsson S, Steglind S. The post-stroke hemiplegic patient. 1: a method for evaluation of physical performance. Scand J Rehabil Med. 1975; 7:13–31.22. Holden MK, Gill KM, Magliozzi MR, Nathan J, Piehl- Baker L. Clinical gait assessment in the neurologically impaired: reliability and meaningfulness. Phys Ther. 1984; 64:35–40.23. Burn JP. Reliability of the modified Rankin Scale. Stroke. 1992; 23:438.
Article24. Dodds TA, Martin DP, Stolov WC, Deyo RA. A validation of the functional independence measurement and its performance among rehabilitation inpatients. Arch Phys Med Rehabil. 1993; 74:531–6.
Article25. Jung HY, Park BK, Shin HS, Kang YK, Pyun SB, Paik NJ, et al. Development of the Korean version of Modified Barthel Index (K-MBI): multi-center study for subjects with stroke. J Korean Acad Rehabil Med. 2007; 31:283–97.26. Williams LS, Rotich J, Qi R, Fineberg N, Espay A, Bruno A, et al. Effects of admission hyperglycemia on mortality and costs in acute ischemic stroke. Neurology. 2002; 59:67–71.
Article27. McBride DW, Matei N, Camara JR, Louis JS, Oudin G, Walker C, et al. Acute hyperglycemia does not affect brain swelling or infarction volume after middle cerebral artery occlusion in rats. Acta Neurochir Suppl. 2016; 121:251–5.
Article28. Candelise L, Landi G, Orazio EN, Boccardi E. Prognostic significance of hyperglycemia in acute stroke. Arch Neurol. 1985; 42:661–3.
Article29. Melamed E. Reactive hyperglycaemia in patients with acute stroke. J Neurol Sci. 1976; 29:267–75.
Article30. Toni D, Sacchetti ML, Argentino C, Gentile M, Cavalletti C, Frontoni M, et al. Does hyperglycaemia play a role on the outcome of acute ischaemic stroke patients? J Neurol. 1992; 239:382–6.31. Lee TH, Ryu SJ, Chen ST. The prognostic value of blood glucose in patients with acute stroke. J Formos Med Assoc. 1991; 90:465–70.32. Baird TA, Parsons MW, Phan T, Butcher KS, Desmond PM, Tress BM, et al. Persistent poststroke hyperglycemia is independently associated with infarct expansion and worse clinical outcome. Stroke. 2003; 34:2208–14.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Association between Neurological Prognosis and Serum Glucose Level by Stroke Subtype in Acute Ischemic Stroke
- The connection between diabetes mellitus and stroke: a brief review
- Blood-brain barrier dysfunction in ischemic stroke and diabetes: the underlying link, mechanisms and future possible therapeutic targets
- The Effect of Hyperglycemia at Admission on Clinical Outcomes after Acute Stroke
- Diabetes and Stroke
