Reassessing Alberta Stroke Program Early CT Score on Non-Contrast CT Based on Degree and Extent of Ischemia
- Ospel JM1,2
- Menon BK1,3
- Marko M1,4
- Mayank A1
- Ganesh A1
- Nogueira RG5
- McTaggart RA6,7,8
- Demchuk AM1,3
- Poppe AY9
- Rempel JL10
- Joshi M1,4
- Almekhlafi MA1,3
- Zerna C1
- Tymianski M11
- Hill MD1,3
- Goyal M
 1,3
1,3 - the ESCAPE-NA1 investigators1
- Affiliations
-
- 1Department of Clinical Neurosciences, University of Calgary, Calgary, AB, Canada
- 2Department of Neuroradiology, University Hospital of Basel, Basel, Switzerland
- 3Department of Diagnostic Imaging, University of Calgary, Calgary, AB, Canada
- 4Department of Neurology, Medical University of Vienna, Vienna, Austria
- 5Marcus Stroke & Neuroscience Center, Department of Neurology, Grady Memorial Hospital, Emory University School of Medicine, Atlanta, GA, USA
- 6Department of Diagnostic Imaging, Warren Alpert School of Medicine at Brown University, Providence, RI, USA
- 7Department of Neurology, Warren Alpert School of Medicine at Brown University, Providence, RI, USA
- 8Department of Neurosurgery, Warren Alpert School of Medicine at Brown University, Providence, RI, USA
- 9Centre Hospitalier de l’Université de Montréal, Montreal, QC, Canada
- 10University of Alberta Hospital, Edmonton, AB, Canada
- 11NoNo Inc., Toronto, ON, Canada
- KMID: 2520921
- DOI: http://doi.org/10.5853/jos.2021.00458
Figure
-
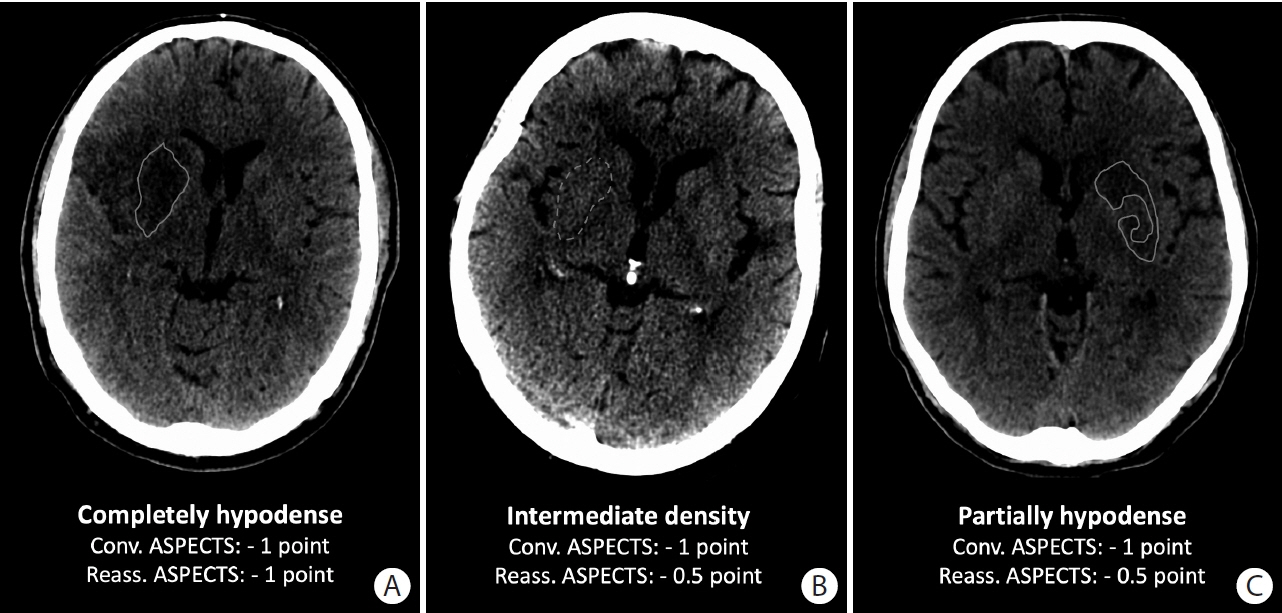
Figure 1. Examples for conventional and reassessed Alberta Stroke Program Early CT Score (ASPECTS). (A) The entire right lentiform nucleus is clearly hypodense (grey line). Thus, a full point would be subtracted in conventional ASPECTS and reassessed ASPECTS. (B) The entire right lentiform nucleus is slightly hypodense compared to the left side (dashed grey line). Thus, a full point would be subtracted in conventional ASPECTS; 0.5 point would be subtracted when reassessing ASPECTS. (C) Some parts of the left lentiform nucleus are clearly hypodense (grey line) while the density in other parts is preserved. Thus, a full point would be subtracted with conventional ASPECTS versus 0.5 point when reassessing ASPECTS.
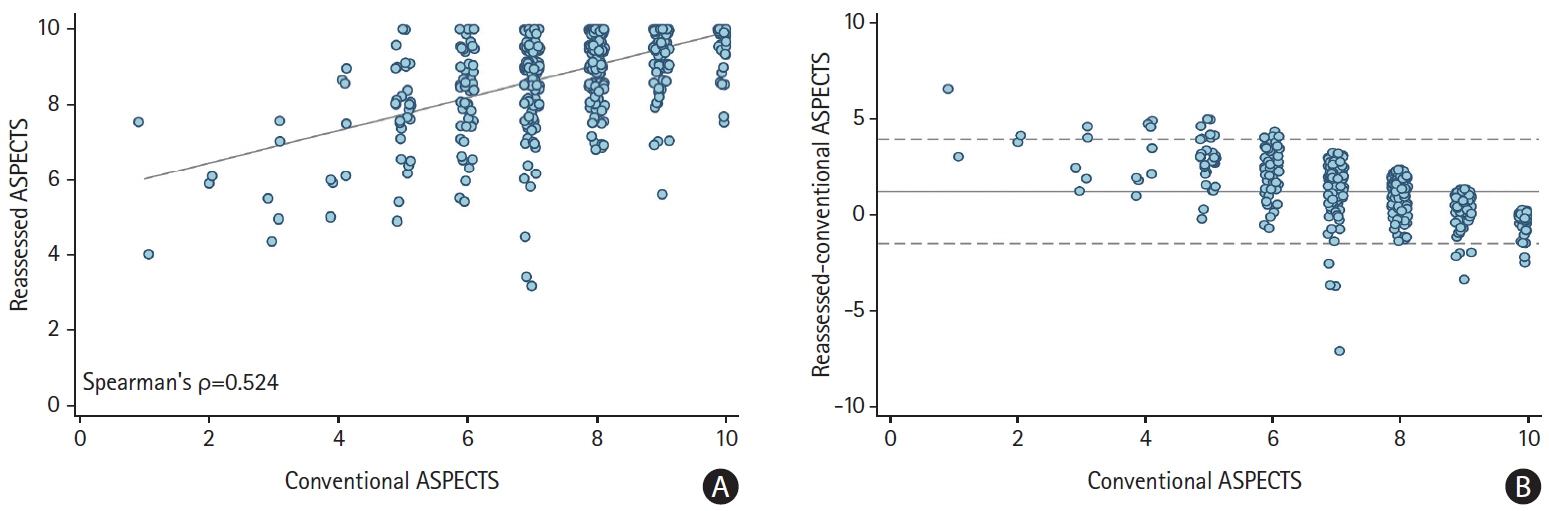
Figure 2. Distribution of conventional and reassessed Alberta Stroke Program Early CT Score (ASPECTS). (A) Scatter-plot showing medians and interquartile ranges of reassessed scores (y-axis) for each ASPECTS value (x-axis). The grey line is fitted from a simple linear regression. (B) Bland Altman plot showing agreement between conventional and reassessed ASPECTS. Central dashed line: average difference (1.2 units) between reassessed and conventional ASPECTS. Lower and upper dashed lines show limits of agreement (–1.5 to 3.9).
Reference
-
References
1. Logan C, Maingard J, Phan K, Motyer R, Barras C, Looby S, et al. Borderline Alberta Stroke Programme Early CT Score patients with acute ischemic stroke due to large vessel occlusion may find benefit with endovascular thrombectomy. World Neurosurg. 2018; 110:e653–e658.
Article2. Hill MD, Goyal M, Menon BK, Nogueira RG, McTaggart RA, Demchuk AM, et al. Efficacy and safety of nerinetide for the treatment of acute ischaemic stroke (ESCAPE-NA1): a multicentre, double-blind, randomised controlled trial. Lancet. 2020; 395:878–887.3. Aarts M, Liu Y, Liu L, Besshoh S, Arundine M, Gurd JW, et al. Treatment of ischemic brain damage by perturbing NMDA receptor- PSD-95 protein interactions. Science. 2002; 298:846–850.
Article4. Menon BK, d’Esterre CD, Qazi EM, Almekhlafi M, Hahn L, Demchuk AM, et al. Multiphase CT angiography: a new tool for the imaging triage of patients with acute ischemic stroke. Radiology. 2015; 275:510–520.
Article5. Saposnik G, Menon BK, Kashani N, Wilson AT, Yoshimura S, Campbell BCV, et al. Factors associated with the decisionmaking on endovascular thrombectomy for the management of acute ischemic stroke. Stroke. 2019; 50:2441–2447.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Alberta Stroke Program Early CT Score in the Prognostication after Endovascular Treatment for Ischemic Stroke: A Meta-analysis
- The S100B Protein Could Be Used as Adjuvant Diagnostic Tool in Acute Ischemic Stroke
- Visibility of CT Early Ischemic Change Is Significantly Associated with Time from Stroke Onset to Baseline Scan beyond the First 3 Hours of Stroke Onset
- Endovascular Treatment in Acute Ischemic Stroke: A Nationwide Survey in Korea
- Penumbral Imaging-Based Thrombolysis with Tenecteplase Is Feasible up to 24 Hours after Symptom Onset
