Clin Endosc.
2021 Sep;54(5):701-705. 10.5946/ce.2020.290.
The Learning Curve for Peroral Endoscopic Myotomy in Latin America: A Slide to the Right?
- Kahaleh M
 1
1 - Tyberg A1
- Suresh S2
- Lambroza A2
- Casas FR3
- Rey M3
- Nieto J4
- Martínez GM5
- Zamarripa F5
- Arantes V6
- Porfilio MG7
- Gaidhane M1
- Familiari P8
- Carames JC9
- Vargas-Rubio R10
- Canadas R10
- Hani A10
- Munoz G1
- Castillo B11
- Moura ET12
- Galileu FF12
- Lukashok HP13
- Robles-Medranda C13
- Moura EGd12
- Affiliations
-
- 1Robert Wood Johnson University Hospital, New Brunswick, NJ, USA
- 2Weill Cornell Medical College, New York, NY, USA
- 3La Policia, Bogota, Colombia
- 4Borland-Groover, Jacksonville, FL, USA
- 5Juarez Hospital, Mexico City, Mexico
- 6Belo Horizonte Hospital, Belo Horizonte, Brazil
- 7Hospital Escuela Dr. Ramon Madariaga, Posadas, Argentina
- 8Gemelli University Hospital, Roma, Italy
- 9Santander Hospital, Reynosa, Mexico
- 10San Ignacio University Hospital, Bogota, Columbia
- 11Gastromedica Clinic, Managua, Nicaragua
- 12Gastrointestinal Endoscopy Unit, University of Sao Paulo, Sao Paulo, Brazil
- 13Instituto Ecuatoriano de Enfermedades Digestivas, Guayaquil, Ecuador
- KMID: 2520553
- DOI: http://doi.org/10.5946/ce.2020.290
Abstract
- Background/Aims
Per oral endoscopic myotomy (POEM) has been increasingly used for achalasia in Latin America, where Chagas disease is prevalent, and this makes POEM more challenging. The aim of this study was to determine the learning curve for POEM in Latin America.
Methods
Patients undergoing POEM in Latin America with a single operator were included from a prospective registry over 4 years. Non-linear regression and cumulative sum control chart (CUSUM) analyses were conducted for the learning curve.
Results
A total of 125 patients were included (52% male; mean age, 59 years), of which 80 had type II achalasia (64%), and 38 had Chagas disease (30%). The average pre-procedure and post-procedure Eckardt scores were 6.79 and 1.87, respectively. Technical success was achieved in 93.5% of patients, and clinical success was achieved in 88.8%. Adverse events occurred in 27 patients (22%) and included bleeding (4 patients), pneumothorax (4 patients), mucosal perforation (13 patients), mediastinitis (2 patients), and leakage (4 patients).
The CUSUM chart showed a median procedure time of 97 min (range, 45-196 min), which was achieved at the 61st procedure. Procedure duration progressively decreased, with the last 10 procedures under 50 min approaching a plateau (p-value <0.01).
Conclusions
Mastering POEM in Latin America requires approximately 61 procedures for both POEM efficiency and to accomplish the procedure within 97 minutes.
Figure
-
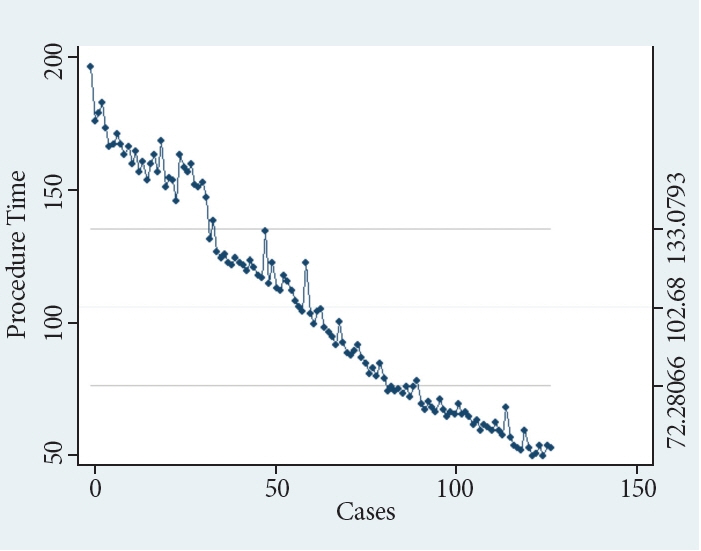
Fig. 1. Cumulative sum control chart shows procedure efficiency duration.
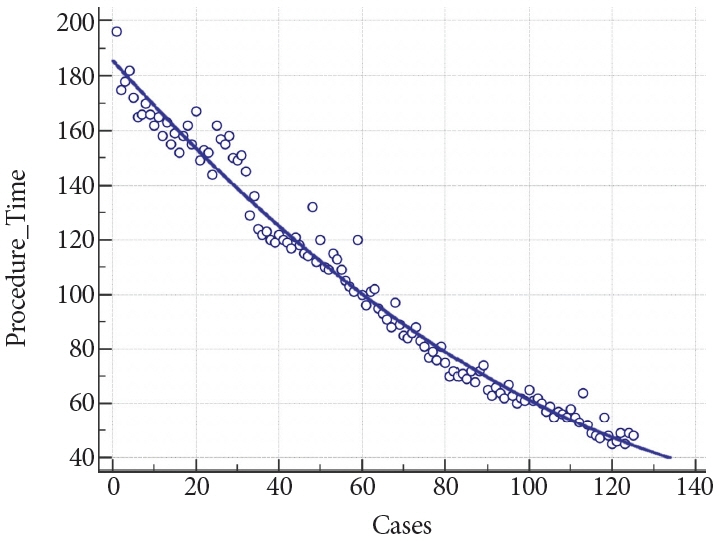
Fig. 2. Inverse curve regression showing procedure time decrease significantly over the course of consecutive procedures.
Cited by 1 articles
-
Issues to be Considered for Learning Curve for Peroral Endoscopic Myotomy
Hironari Shiwaku, Haruhiro Inoue
Clin Endosc. 2021;54(5):625-626. doi: 10.5946/ce.2021.217.
Reference
-
1. Inoue H, Minami H, Kobayashi Y, et al. Peroral endoscopic myotomy (POEM) for esophageal achalasia. Endoscopy. 2010; 42:265–271.
Article2. Stavropoulos SN, Modayil RJ, Friedel D, Savides T. The international per oral endoscopic myotomy survey (IPOEMS): a snapshot of the global POEM experience. Surg Endosc. 2013; 27:3322–3338.
Article3. Crespin OM, Liu LWC, Parmar A, et al. Safety and efficacy of POEM for treatment of achalasia: a systematic review of the literature. Surg Endosc. 2017; 31:2187–2201.
Article4. Li H, Peng W, Huang S, et al. The 2years’ long-term efficacy and safety of peroral endoscopic myotomy for the treatment of achalasia: a systematic review. J Cardiothorac Surg. 2019; 14:1.
Article5. Stavropoulos SN, Modayil R, Friedel D. Per oral endoscopic myotomy for the treatment of achalasia. Curr Opin Gastroenterol. 2015; 31:430–440.
Article6. Tantau M, Crisan D. Peroral endoscopic myotomy: time to change our opinion regarding the treatment of achalasia? World J Gastrointest Endosc. 2015; 7:237–246.
Article7. von Rahden BHA. [Current treatment of achalasia 2019]. Zentralbl Chir. 2019; 144:163–170.8. Pescarus R, Shlomovitz E, Swanstrom LL. Per-oral endoscopic myotomy (POEM) for esophageal achalasia. Curr Gastroenterol Rep. 2014; 16:369.
Article9. Liu Z, Zhang X, Zhang W, et al. Comprehensive evaluation of the learning curve for peroral endoscopic myotomy. Clin Gastroenterol Hepatol. 2018; 16:1420–1426.e2.
Article10. Tanţău M, Buzaş C, Tefas C, Groza A, Tanţău A. “Learning curve” for the POEM procedure. J Gastrointestin Liver Dis. 2015; 24:536–537.11. Kurian AA, Dunst CM, Sharata A, Bhayani NH, Reavis KM, Swanström LL. Peroral endoscopic esophageal myotomy: defining the learning curve. Gastrointest Endosc. 2013; 77:719–725.
Article12. Patel KS, Calixte R, Modayil RJ, Friedel D, Brathwaite CE, Stavropoulos SN. The light at the end of the tunnel: a single-operator learning curve analysis for per oral endoscopic myotomy. Gastrointest Endosc. 2015; 81:1181–1187.
Article13. El Zein M, Kumbhari V, Ngamruengphong S, et al. Learning curve for peroral endoscopic myotomy. Endosc Int Open. 2016; 4:E577–E582.
Article14. Zaninotto G, Bennett C, Boeckxstaens G, et al. The 2018 ISDE achalasia guidelines. Dis Esophagus. 2018; 31:1–29.15. Kahaleh M, Xu M-M, Zamarripa F, et al. POEM in Latin America: the rise of a new standard. J Clin Gastroenterol. 2019; 53:e352–e355.16. Teitelbaum EN, Soper NJ, Arafat FO, et al. Analysis of a learning curve and predictors of intraoperative difficulty for peroral esophageal myotomy (POEM). J Gastrointest Surg. 2014; 18:92–98. discussion 98-99.
Article17. Nabi Z, Reddy DN, Ramchandani M. Adverse events during and after per-oral endoscopic myotomy: prevention, diagnosis, and management. Gastrointest Endosc. 2018; 87:4–17.18. Wang Y, Liu Z-Q, Xu M-D, et al. Clinical and endoscopic predictors for intraprocedural mucosal injury during per-oral endoscopic myotomy. Gastrointest Endosc. 2019; 89:769–778.
Article19. Hungness ES, Sternbach JM, Teitelbaum EN, Kahrilas PJ, Pandolfino JE, Soper NJ. Per-oral endoscopic myotomy (POEM) after the learning curve: durable long-term results with a low complication rate. Ann Surg. 2016; 264:508–517.20. Lv H, Zhao N, Zheng Z, et al. Analysis of the learning curve for peroral endoscopic myotomy for esophageal achalasia: single-center, two-operator experience. Dig Endosc. 2017; 29:299–306.
Article21. Vaz Â, Ferrari TA, Gomes RV, Arantes VN. Peroral endoscopic myotomy for management of megaesophagus due to Chagas disease. Relatos Casos Cir. 2016; 1:1–3.22. Kahaleh M, Tyberg A, Suresh S, et al. How does per-oral endoscopic myotomy compare to Heller myotomy? The Latin American perspective. Endosc Int Open. 2020; 8:E1392–E1397.
Article23. Biau DJ, Williams SM, Schlup MM, Nizard RS, Porcher R. Quantitative and individualized assessment of the learning curve using LC-CUSUM. Br J Surg. 2008; 95:925–929.
Article24. Akintoye E, Kumar N, Obaitan I, Alayo QA, Thompson CC. Peroral endoscopic myotomy: a meta-analysis. Endoscopy. 2016; 48:1059–1068.
Article25. Tefas C, Boroș C, Ciobanu L, Surdea-Blaga T, Tanțău A, Tanțău M. POEM: five years of experience in a single east european center. J Gastrointestin Liver Dis. 2020; 29:323–328.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Issues to be Considered for Learning Curve for Peroral Endoscopic Myotomy
- Current Status of Peroral Endoscopic Myotomy
- Perspective on Peroral Endoscopic Myotomy for Achalasia: Zhongshan Experience
- Double-Scope Peroral Endoscopic Myotomy (POEM) for Esophageal Achalasia: The First Trial of a New Double-Scope POEM
- Two-Stage Peroral Endoscopic Myotomy for Sigmoid-Type Achalasia
