Contralateral Suppression at Adrenal Venous Sampling Is Associated with Renal Impairment Following Adrenalectomy for Unilateral Primary Aldosteronism
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea
- 2Department of Internal Medicine, Uijeongbu St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea
- 3Division of Endocrinology and Metabolism, Department of Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 4Division of Endocrinology and Metabolism, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 5Department of Internal Medicine, Mediplex Sejong Hospital, Incheon, Korea
- 6Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea
- 7Department of Internal Medicine, Chungbuk National University Hospital, Cheongju, Korea
- 8Division of Endocrinology and Metabolism, Seoul Metropolitan Government Seoul National University Boramae Medical Center, Seoul, Korea
- KMID: 2519675
- DOI: http://doi.org/10.3803/EnM.2021.1047
Abstract
- Background
Adrenal venous sampling (AVS) is performed to distinguish the subtype of primary aldosteronism (PA). The clinical implication of contralateral suppression (CS; aldosterone/cortisolnondominantperipheral) at AVS remains unclear. We aimed to investigate the clinical significance of CS and its impact on postoperative outcomes after unilateral adrenalectomy.
Methods
In this retrospective observational multi-center study, we analyzed PA patients who underwent both successful adrenocorticotropin hormone-stimulated AVS and unilateral adrenalectomy. Successful cannulation was defined as the selectivity index (cortisoladrenal/ cortisolperipheral) ≥3. Clinical and biochemical outcomes after unilateral adrenalectomy were evaluated based on the international Primary Aldosteronism Surgical Outcome consensus.
Results
Among 263 patients analyzed, 247 had CS (93.9%). Patients with CS had lower serum potassium levels, higher plasma aldosterone concentration, higher aldosterone-to-renin ratio (ARR), and larger adenoma size than those without CS. Those with CS showed significantly higher lateralization index than those without CS (P<0.001). Although postoperative blood pressure and ARR significantly decreased in those with CS, clinical and biochemical outcomes were comparable in both groups. When the cut-off value of age was determined using receiver operating characteristic (ROC) analysis, patients aged ≥50 years old with contralateral suppression index (CSI; the ratio between aldosterone/cortisolnondominant and aldosterone/cortisolperipheral) ≤0.26 had greater odds ratio (6.43; 95% confidence interval, 1.30 to 31.69) of incident chronic kidney disease than those aged <50 years with CSI >0.26 after adjusting for other factors.
Conclusion
CS may not predict postoperative clinical and biochemical outcomes in subjects with unilateral aldosterone excess, but it is associated with postsurgical deterioration of renal function in subjects over 50 years with CSI ≤0.26.
Keyword
Figure
-
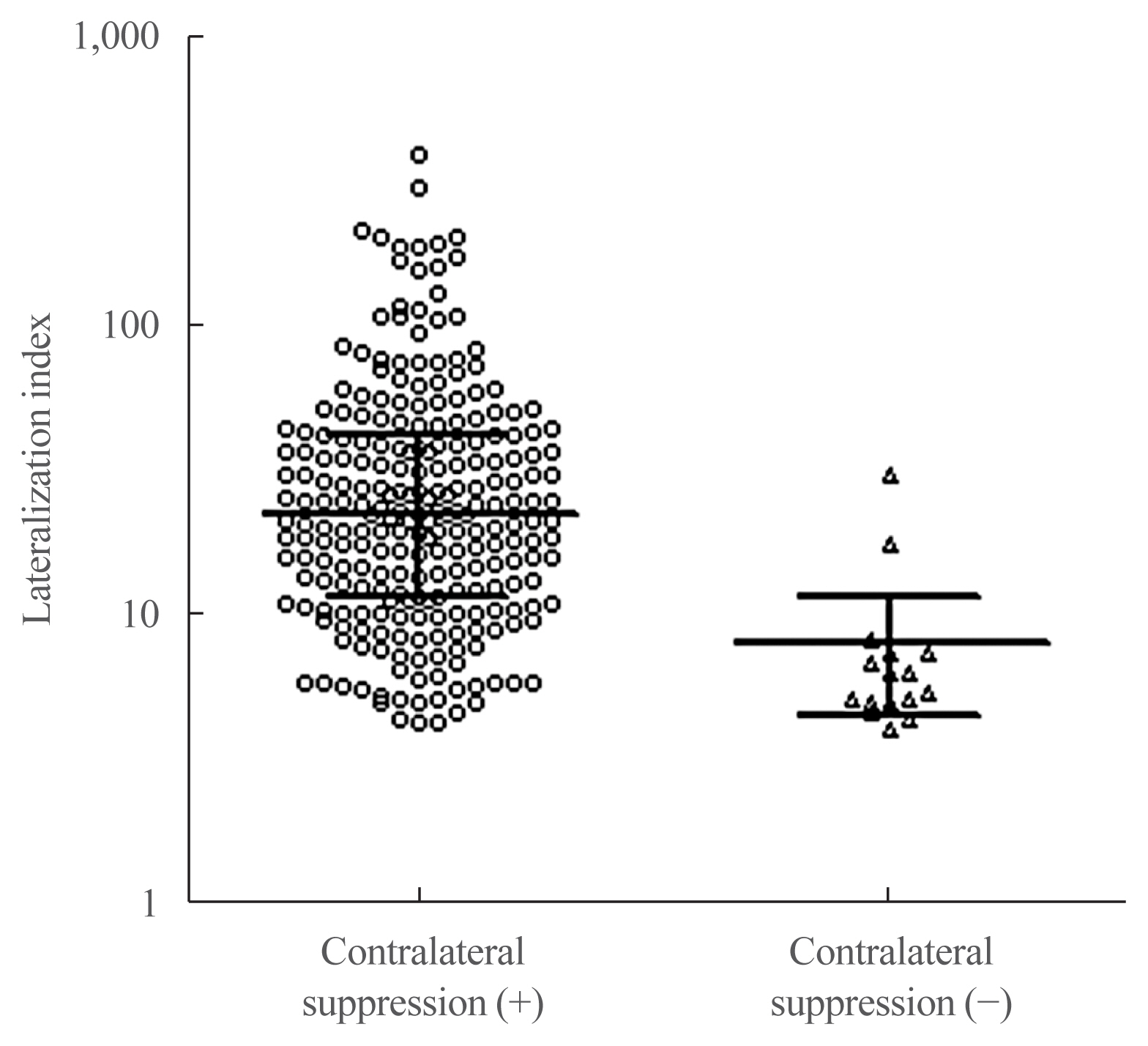
Fig. 1 Lateralization index between patients with and without contralateral suppression. Data are median with interquartile range. Using a Mann-Whitney U test, P<0.001.
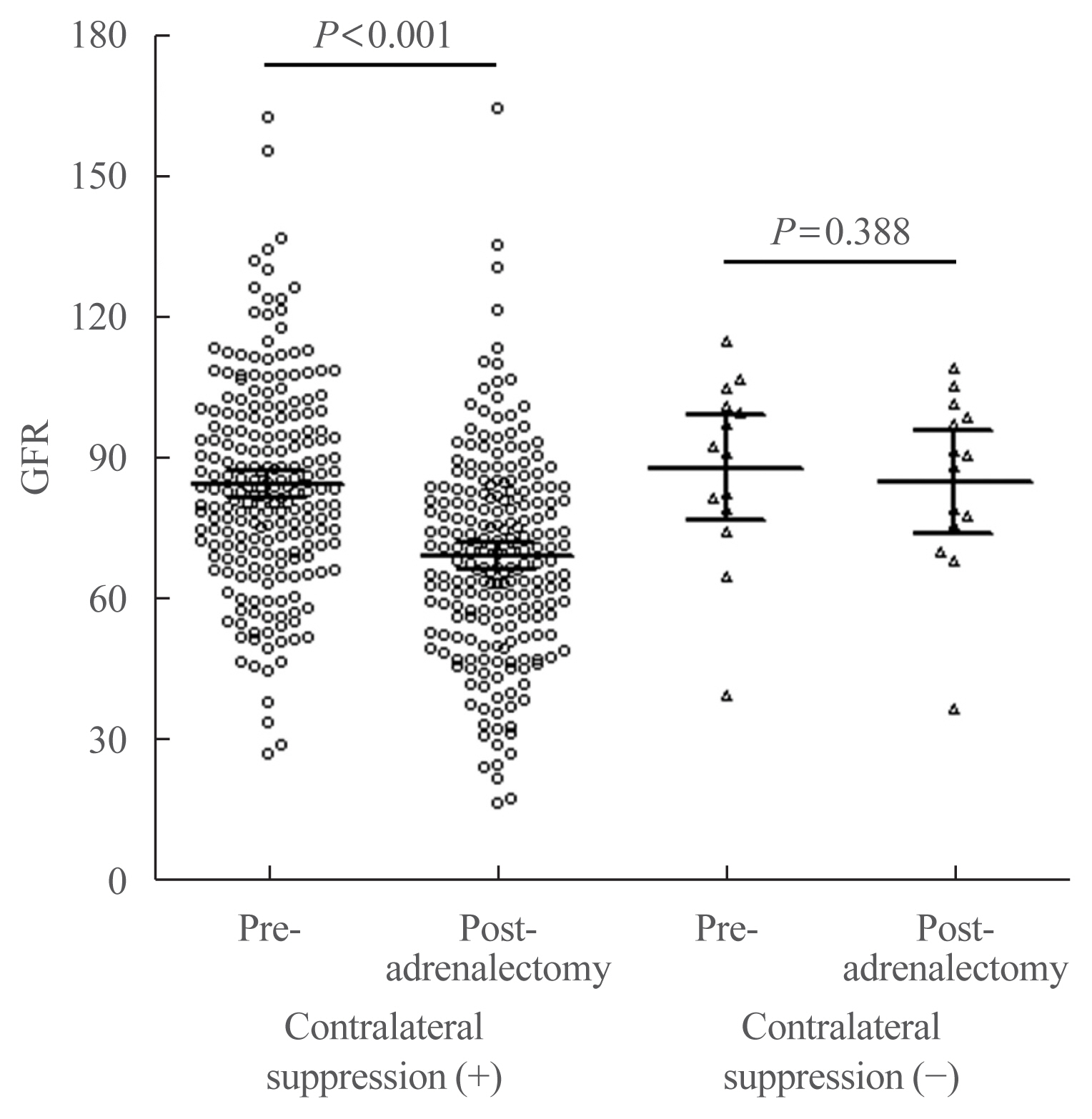
Fig. 2 Changes of glomerular filtration rate after adrenalectomy according to the presence or absence of contralateral suppression. Data are mean with 95% confidence intervals. A decrease of glomerular filtration rate (GFR) after adrenalectomy within each group was analyzed using paired t test.
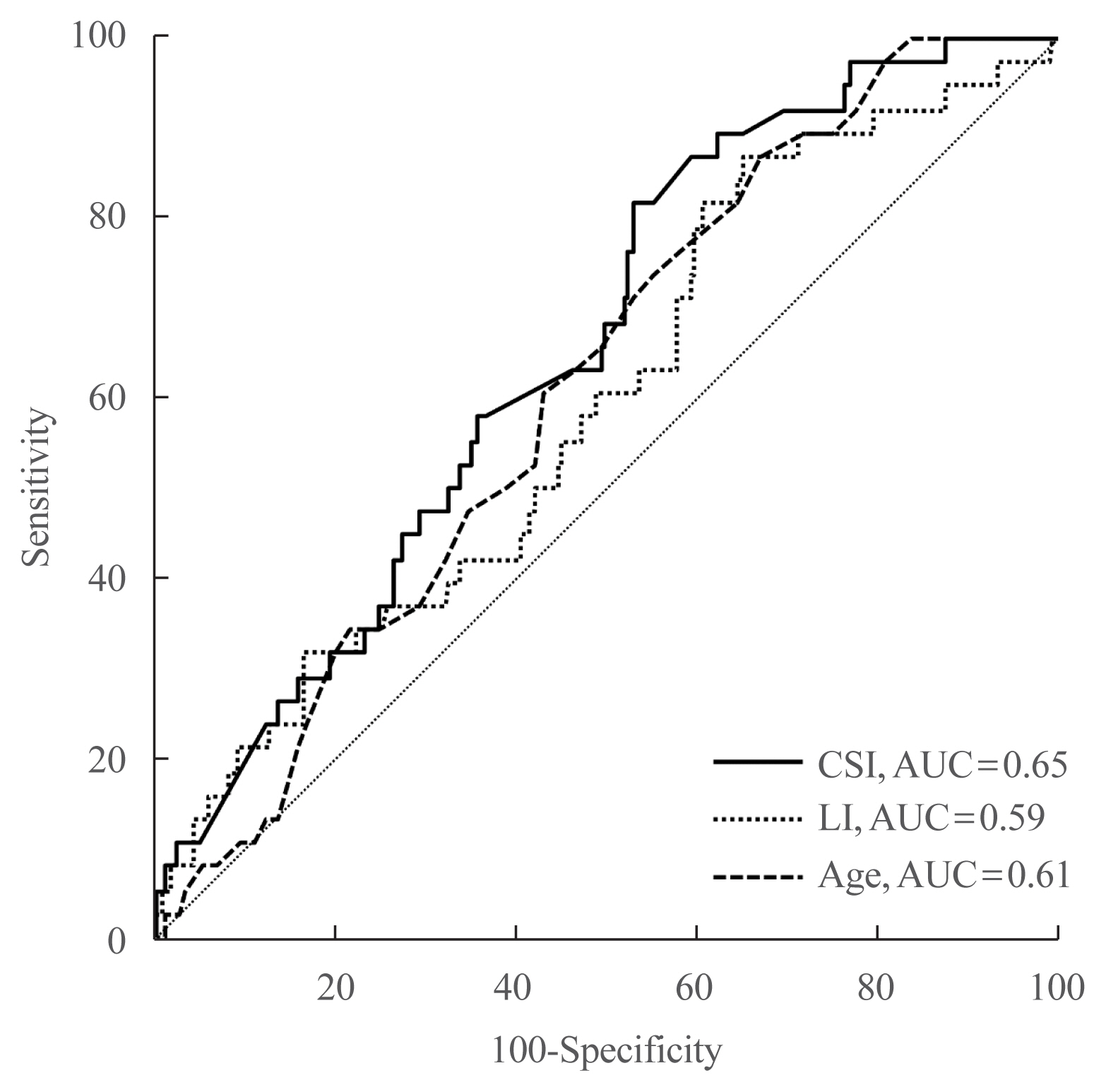
Fig. 3 Receiver operating characteristic curves of contralateral suppression index (CSI), lateralization index (LI), and age as predictors of incident chronic kidney disease after adrenalectomy. AUC, area under the curve.
Cited by 2 articles
-
Contralateral Suppression at Adrenal Venous Sampling Is Associated with Renal Impairment Following Adrenalectomy for Unilateral Primary Aldosteronism (
Endocrinol Metab 2021;36:875-84, Ye Seul Yang et al.)
Ye Seul Yang, Sang Wan Kim
Endocrinol Metab. 2022;37(6):953-954. doi: 10.3803/EnM.2022.603.Contralateral Suppression at Adrenal Venous Sampling Is Associated with Renal Impairment Following Adrenalectomy for Unilateral Primary Aldosteronism (
Endocrinol Metab 2021;36:875-84, Ye Seul Yang et al.)
Zhimin Tan, Qiyu He, Liang Zhou
Endocrinol Metab. 2022;37(6):951-952. doi: 10.3803/EnM.2022.1606.
Reference
-
1. Rossi GP, Bernini G, Calitype C, Desideri G, Fabris B, Ferri C, et al. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol. 2006; 48:2293–300.
Article2. Kayser SC, Dekkers T, Groenewoud HJ, van der Wilt GJ, Carel Bakx J, van der Wel MC, et al. Study heterogeneity and estimation of prevalence of primary aldosteronism: a systematic review and meta-regression analysis. J Clin Endocrinol Metab. 2016; 101:2826–35.
Article3. Funder JW, Carey RM, Mantero F, Murad MH, Reincke M, Shibata H, et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2016; 101:1889–916.
Article4. Monticone S, Viola A, Rossato D, Veglio F, Reincke M, Gomez-Sanchez C, et al. Adrenal vein sampling in primary aldosteronism: towards a standardised protocol. Lancet Diabetes Endocrinol. 2015; 3:296–303.
Article5. Umakoshi H, Tsuiki M, Yokomoto-Umakoshi M, Takeda Y, Takashi Y, Kurihara I, et al. Correlation between lateralization index of adrenal venous sampling and standardized outcome in primary aldosteronism. J Endocr Soc. 2018; 2:893–902.
Article6. Tagawa M, Ghosn M, Wachtel H, Fraker D, Townsend RR, Trerotola S, et al. Lateralization index but not contralateral suppression at adrenal vein sampling predicts improvement in blood pressure after adrenalectomy for primary aldosteronism. J Hum Hypertens. 2017; 31:444–9.
Article7. Williams TA, Reincke M. Management of endocrine disease: diagnosis and management of primary aldosteronism: the Endocrine Society guideline 2016 revisited. Eur J Endocrinol. 2018; 179:R19–29.
Article8. Wolley MJ, Gordon RD, Ahmed AH, Stowasser M. Does contralateral suppression at adrenal venous sampling predict outcome following unilateral adrenalectomy for primary aldosteronism?: a retrospective study. J Clin Endocrinol Metab. 2015; 100:1477–84.
Article9. Umakoshi H, Tanase-Nakao K, Wada N, Ichijo T, Sone M, Inagaki N, et al. Importance of contralateral aldosterone suppression during adrenal vein sampling in the subtype evaluation of primary aldosteronism. Clin Endocrinol (Oxf). 2015; 83:462–7.
Article10. Monticone S, Satoh F, Viola A, Fischer E, Vonend O, Bernini G, et al. Aldosterone suppression on contralateral adrenal during adrenal vein sampling does not predict blood pressure response after adrenalectomy. J Clin Endocrinol Metab. 2014; 99:4158–66.
Article11. Shin SY, Park YR, Shin Y, Choi HJ, Park J, Lyu Y, et al. A de-identification method for bilingual clinical texts of various note types. J Korean Med Sci. 2015; 30:7–15.
Article12. Williams TA, Lenders JW, Mulatero P, Burrello J, Rottenkolber M, Adolf C, et al. Outcomes after adrenalectomy for unilateral primary aldosteronism: an international consensus on outcome measures and analysis of remission rates in an international cohort. Lancet Diabetes Endocrinol. 2017; 5:689–99.
Article13. Hundemer GL, Curhan GC, Yozamp N, Wang M, Vaidya A. Renal outcomes in medically and surgically treated primary aldosteronism. Hypertension. 2018; 72:658–66.
Article14. Chen ZW, Hung CS, Wu VC, Lin YH. TAIPAI Study Group. Primary aldosteronism and cerebrovascular diseases. Endocrinol Metab (Seoul). 2018; 33:429–34.
Article15. Sechi LA, Colussi G, Di Fabio A, Catena C. Cardiovascular and renal damage in primary aldosteronism: outcomes after treatment. Am J Hypertens. 2010; 23:1253–60.
Article16. Sechi LA, Novello M, Lapenna R, Baroselli S, Nadalini E, Colussi GL, et al. Long-term renal outcomes in patients with primary aldosteronism. JAMA. 2006; 295:2638–45.
Article17. Sechi LA, Di Fabio A, Bazzocchi M, Uzzau A, Catena C. Intrarenal hemodynamics in primary aldosteronism before and after treatment. J Clin Endocrinol Metab. 2009; 94:1191–7.
Article18. Park KS, Kim JH, Yang YS, Hong AR, Lee DH, Moon MK, et al. Outcomes analysis of surgical and medical treatments for patients with primary aldosteronism. Endocr J. 2017; 64:623–32.
Article19. Park KS, Kim JH, Ku EJ, Hong AR, Moon MK, Choi SH, et al. Clinical risk factors of postoperative hyperkalemia after adrenalectomy in patients with aldosterone-producing adenoma. Eur J Endocrinol. 2015; 172:725–31.
Article20. Shariq OA, Bancos I, Cronin PA, Farley DR, Richards ML, Thompson GB, et al. Contralateral suppression of aldosterone at adrenal venous sampling predicts hyperkalemia following adrenalectomy for primary aldosteronism. Surgery. 2018; 163:183–90.
Article21. Tahir A, McLaughlin K, Kline G. Severe hyperkalemia following adrenalectomy for aldosteronoma: prediction, pathogenesis and approach to clinical management: a case series. BMC Endocr Disord. 2016; 16:43.
Article22. Sukor N, Gordon RD, Ku YK, Jones M, Stowasser M. Role of unilateral adrenalectomy in bilateral primary aldosteronism: a 22-year single center experience. J Clin Endocrinol Metab. 2009; 94:2437–45.
Article23. Omata K, Satoh F, Morimoto R, Ito S, Yamazaki Y, Nakamura Y, et al. Cellular and genetic causes of idiopathic hyperaldosteronism. Hypertension. 2018; 72:874–80.
Article24. Rossitto G, Amar L, Azizi M, Riester A, Reincke M, Degenhart C, et al. Subtyping of primary aldosteronism in the avis-2 study: assessment of selectivity and lateralization. J Clin Endocrinol Metab. 2020; 105:dgz017.
Article25. Rossi GP, Seccia TM, Pessina AC. A diagnostic algorithm: the holy grail of primary aldosteronism. Nat Rev Endocrinol. 2011; 7:697–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Factors Associated with Resolution of Hypertension after Adrenalectomy in Patients with Primary Aldosteronism
- Primary Aldosteronism Due to Aldosterone Producing Adenama in the Presence of Contralateral Nonfunctioning Adenama
- Contralateral Suppression at Adrenal Venous Sampling Is Associated with Renal Impairment Following Adrenalectomy for Unilateral Primary Aldosteronism (Endocrinol Metab 2021;36:875-84, Ye Seul Yang et al.)
- Contralateral Suppression at Adrenal Venous Sampling Is Associated with Renal Impairment Following Adrenalectomy for Unilateral Primary Aldosteronism (Endocrinol Metab 2021;36:875-84, Ye Seul Yang et al.)
- Anesthetic Management of a patient with Primary Aldosteronism caused by Adrenal Adenoma
