Sequential treatment from mandibulectomy to reconstruction on mandibular oral cancer – Case review II: mandibular anterior and the floor of the mouth lesion of basaloid squamous cell carcinoma and clear cell odontogenic carcinoma
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, School of Dentistry, Pusan National University, Yangsan, Korea
- KMID: 2517272
- DOI: http://doi.org/10.5125/jkaoms.2021.47.3.216
Abstract
- Preoperative patient analysis for oral cancer involves multiple considerations that are based on multiple factors; these include TNM stages, histopathologic findings, and adjacent anatomical structures. Once the decision is made to excise the lesion, the margin of dissection and its extent should be considered along with the best form of reconstruction and airway management. Treatment methods include surgical resection, radiotherapy, and chemotherapy. Although the combined method of treatment is controversial, surgical resection is considered predominantly, and immediate reconstruction after surgical resection follows. The choice of treatment is dictated by the anticipated functional and esthetic results of treatment and also by the availability of a surgeon with the required expertise. Segmental mandibulectomy with primary reconstruction has been shown to have advantages in both functional and esthetic results. A 52-year-old male patient with basaloid squamous cell carcinoma of the floor of the mouth, and the anterior portion of the mandible was treated with surgical procedures that included segmental mandibulectomy with both supraomohyoid neck dissection (SOHND) at Levels I–III and mandible reconstruction with a left fibula free flap. A 55-year-old male patient with clear cell odontogenic carcinoma of the oral cavity underwent segmental mandibulectomy with both SOHND at Levels I–III and mandible reconstruction with a left fibula free flap. The purpose of this study was to review the anatomic and functional results of patients after immediate reconstruction with a fibula free flap following resection of carcinoma in the anterior portion of the mandible and floor of the mouth.
Keyword
Figure
-
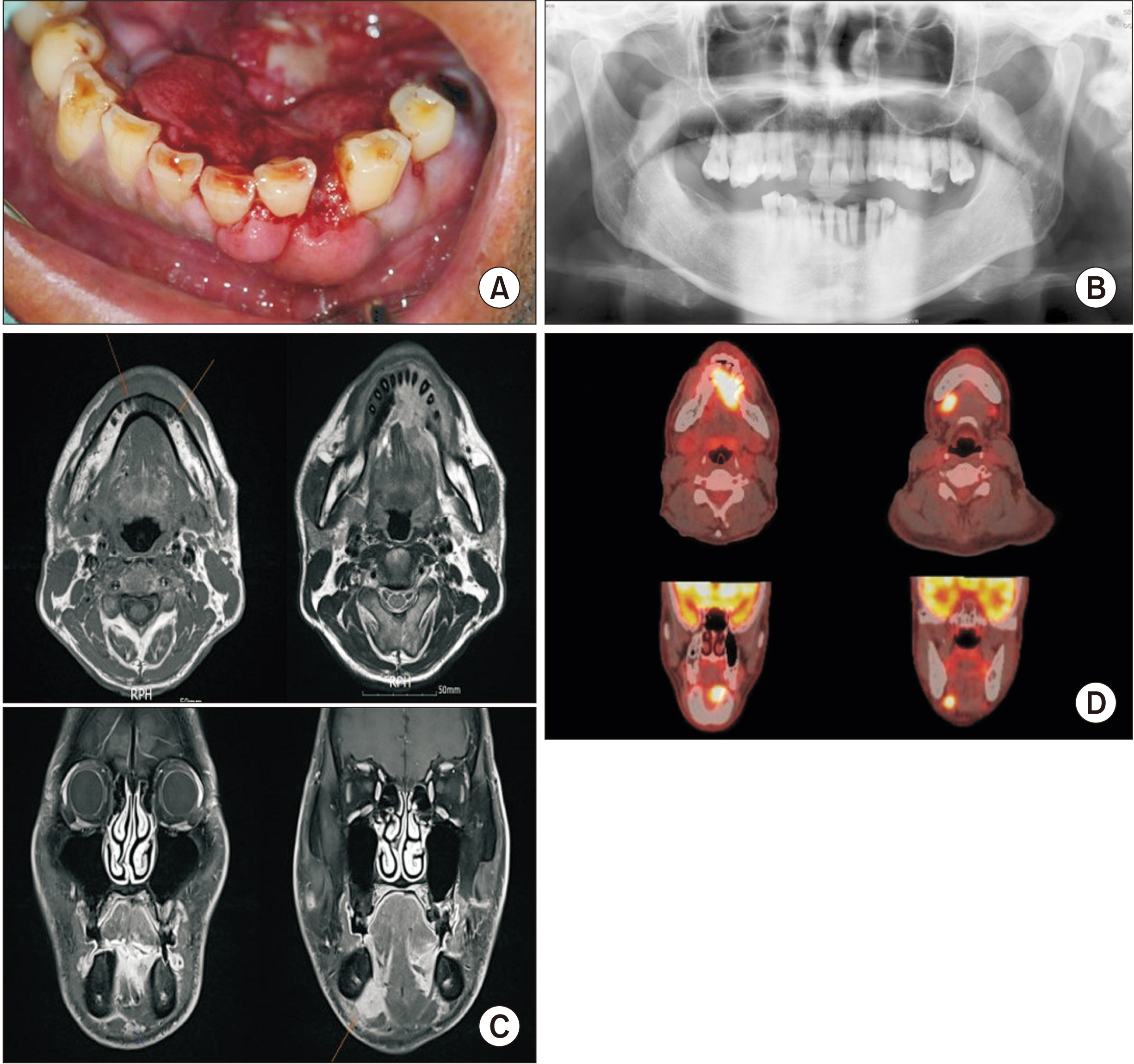
Fig. 1 Preoperative clinical and radiographic features. A. Intraoral feature. Ulcerative and proliferative lesion on the floor of mouth and the anterior of mandible. B. Panoramic radiograph image. Ill-defined osteolytic lesion on mandibular anterior. C. Facial magnetic resonance image showed enhancing soft tissue density around the mandibular anterior, extend to both sublingual space and left tongue base and bony erosive change of mandibular symphysis. Multiple enhancing bilateral lymph nodes (LNs) (Level IA, IB) were observed. D. Abnormally increased fluorodeoxyglucose uptake was observed in the floor of mouth (standardized uptake value [SUV]: 17.1) and in both Level IB LNs (SUV: 11.9 and 3.2, respectively).

Fig. 2 Representative histological section of basaloid squamous cell carcinoma. H&E staining, A: ×0.4 (scale bar=7 mm), B: ×2 (scale bar=2 mm), C: ×12 (scale bar=200 mm), D: ×10 (scale bar=200 mm). A, C. Histopathological examination on the tumor showed cells were forming nodule and growing. There were discrete cell boundaries, abundant eosinophilic cytoplasm, and a large number of tumor cells in which the nucleus was very distinct and the nucleoli were well visible. Nuclear hyperchromatism and pleomorphism were evident and many mitoses were observed. Dysplastic epithelial cells with keratin pearl formation are clearly evident and are considered to be well differentiated squamous cell carcinoma. B, D. Cell nest or lobule, forming infiltrative growth. Characteristically comedo-type necrosis was observed.
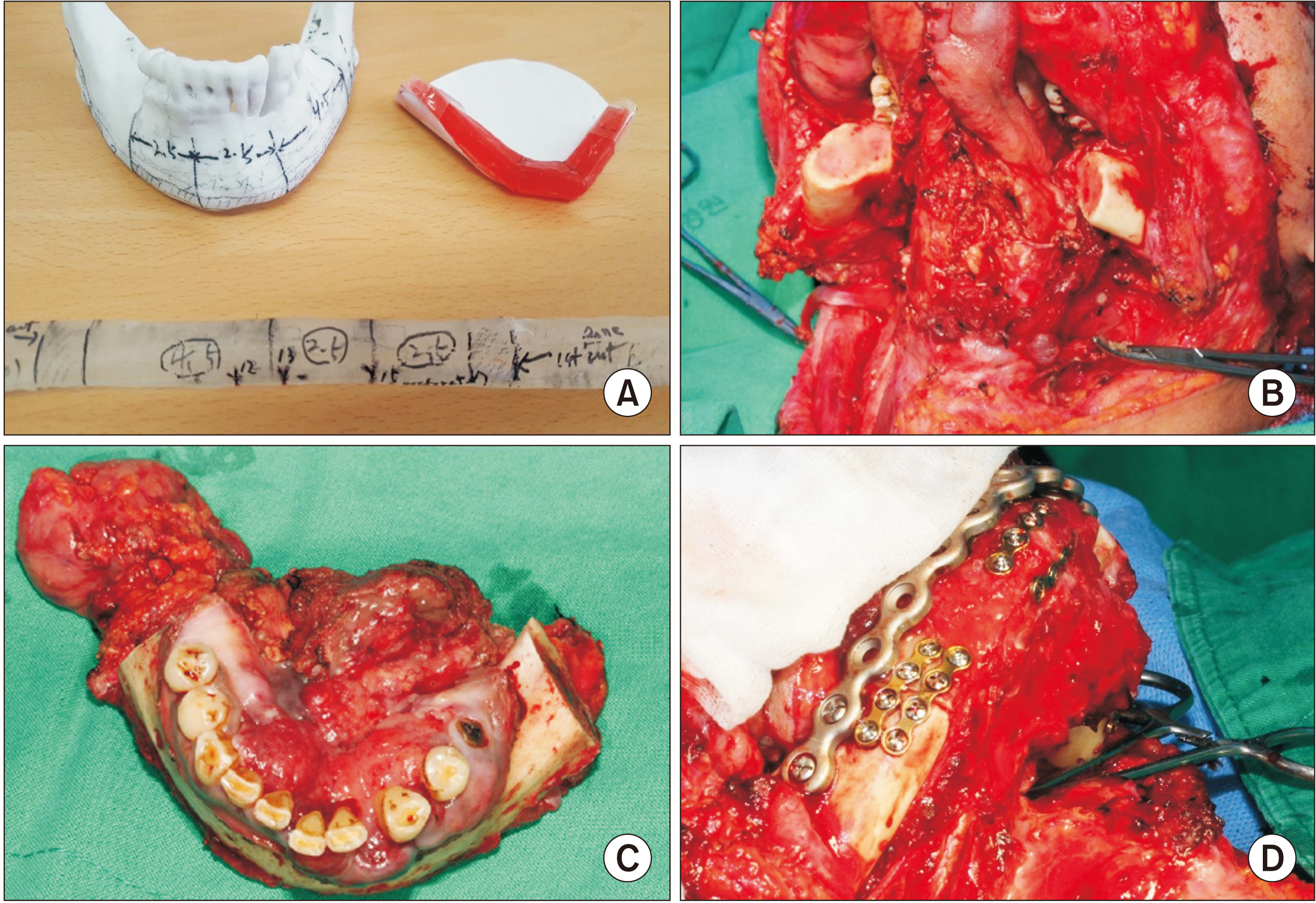
Fig. 3 Intraoperative photographs. A. Rapid prototype model of mandible, resin block for fibula osteotomy. B. Segmental mandibulectomy with supraomohyoid neck dissection. C. Excised tumor mass including mandible, the floor of the mouth, lymph node. D. Mandibular reconstruction with fibula free flap fixed with reconstruct plate and mini plates.
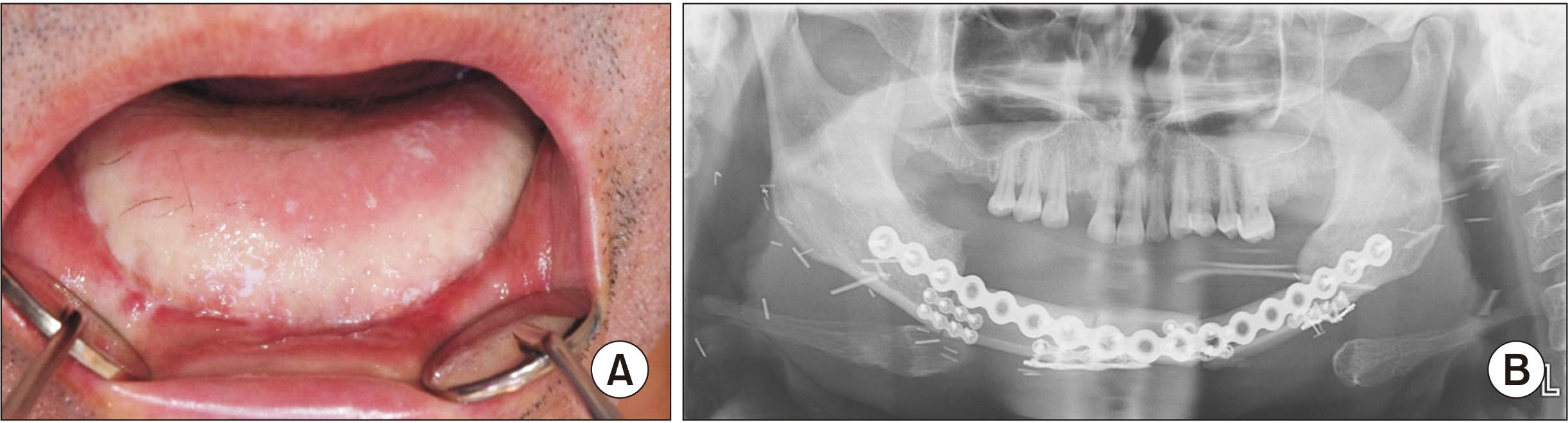
Fig. 4 Postoperative findings. A. Intraoral photograph of the primary site. B. Panoramic radiography. The patient underwent radiotherapy over 6 weeks after surgery and he had a good prognosis and is presently on follow-up.
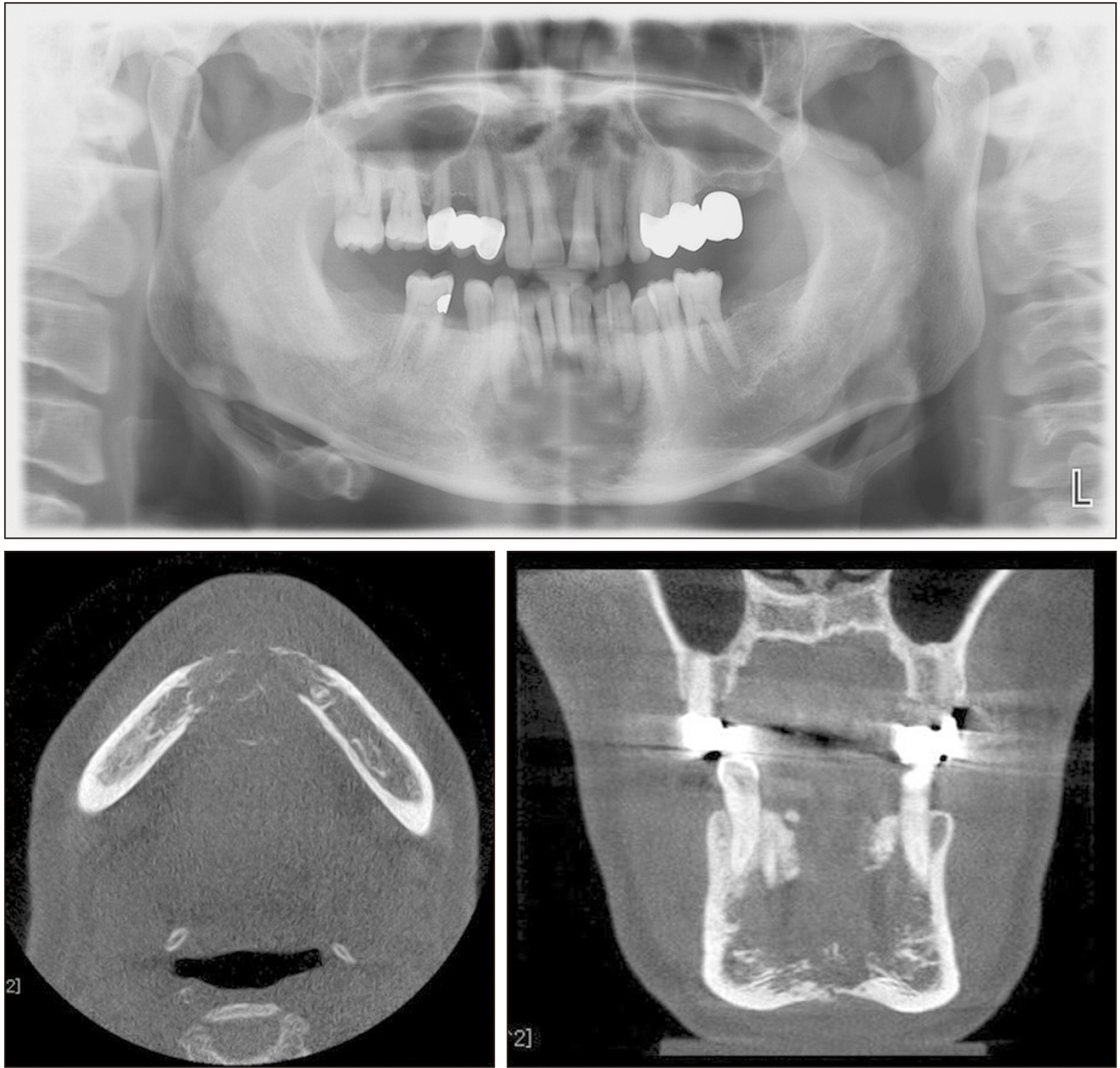
Fig. 5 Preoperative radiographs of panorama & cone-beam computed tomography. In the anterior portion of the mandible, irregularly lesions with a diameter of 3 cm are observed. Perforation of the bucco-lingual cortical bone and root resorption are observed.
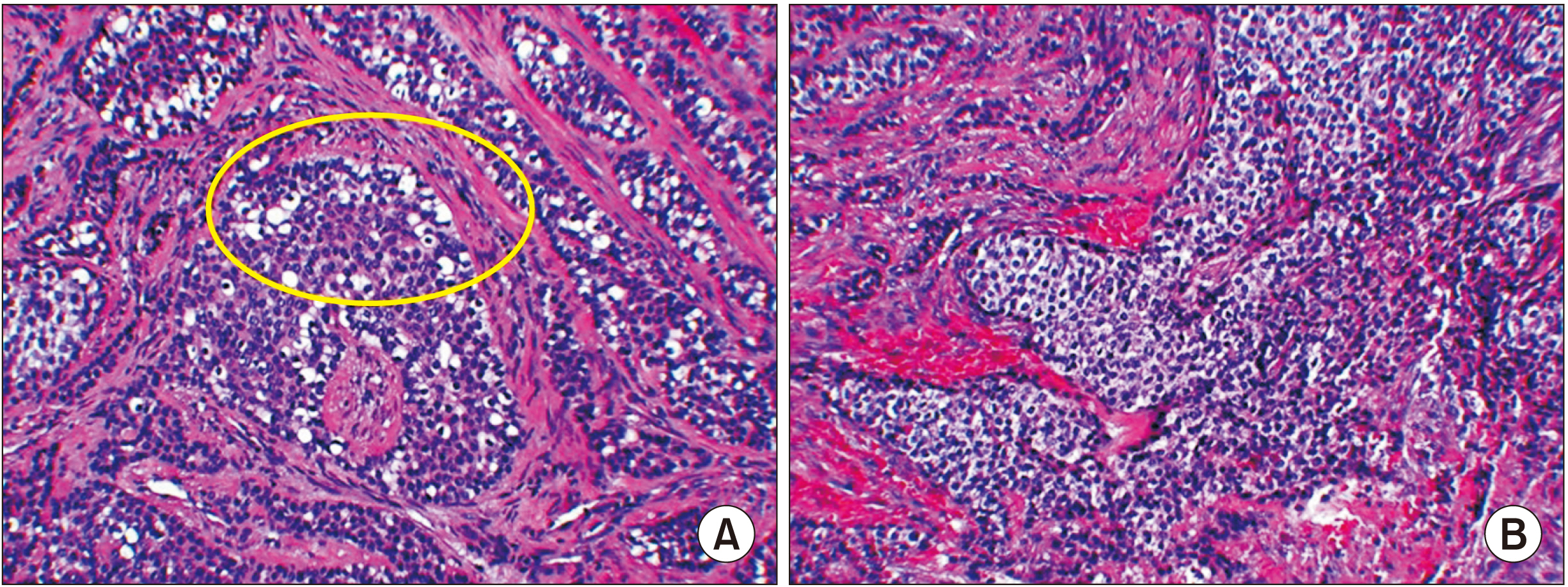
Fig. 6 Histopathologic findings (H&E staining, ×200). A. The ameloblastic basal lamina structure was observed during the presence of clear cells. B. Hyperchromatic islands of basaloid epithelial cell have been demonstrated.
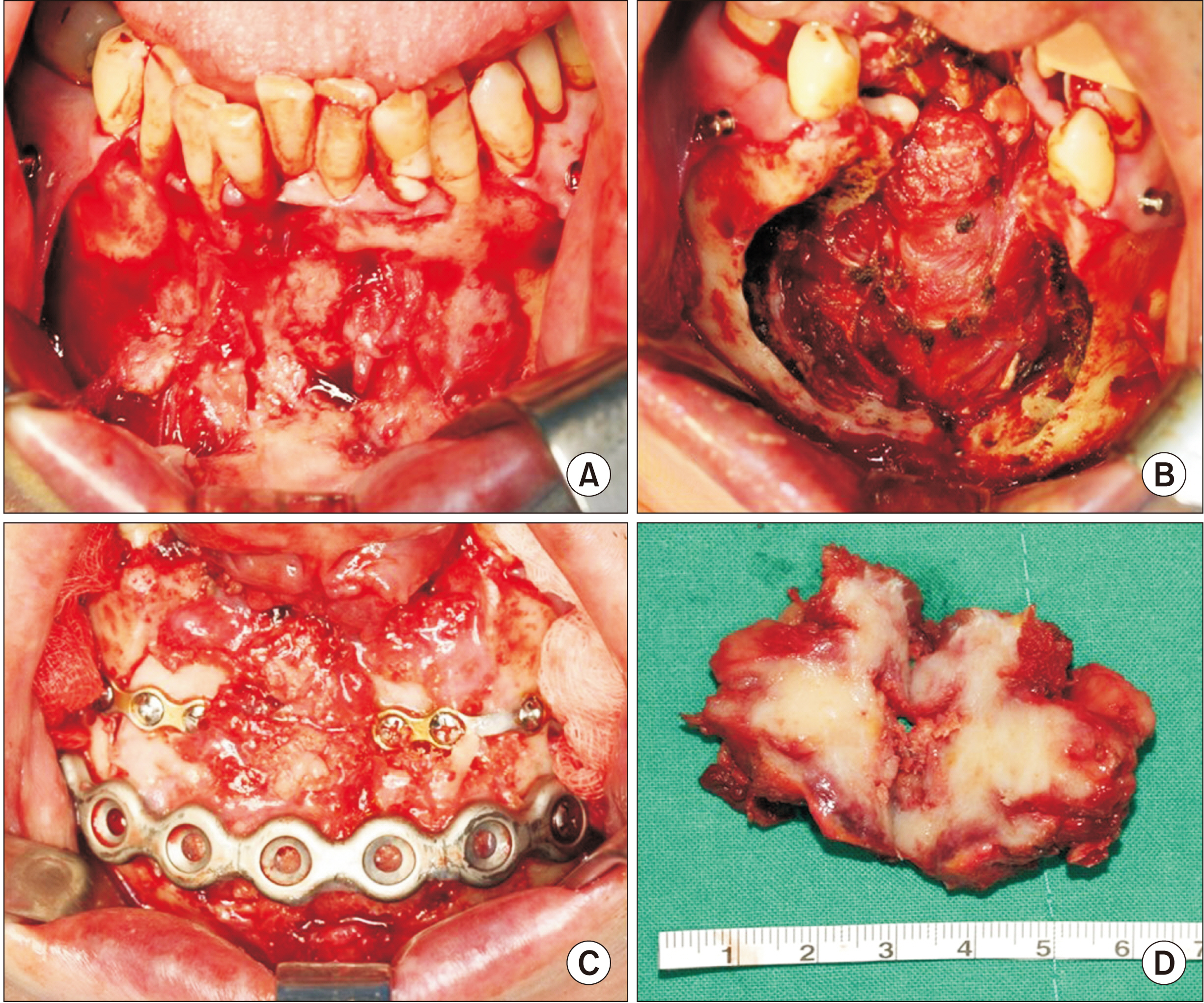
Fig. 7 Photographs of 1st operation. A. Primary site before excision. B. After excision. C. Mandibular reconstruction with immediate iliac block bone graft and reconstruction plate. D. Main mass wide excision and mandibular reconstruction with iliac block bone were performed under general anesthesia.
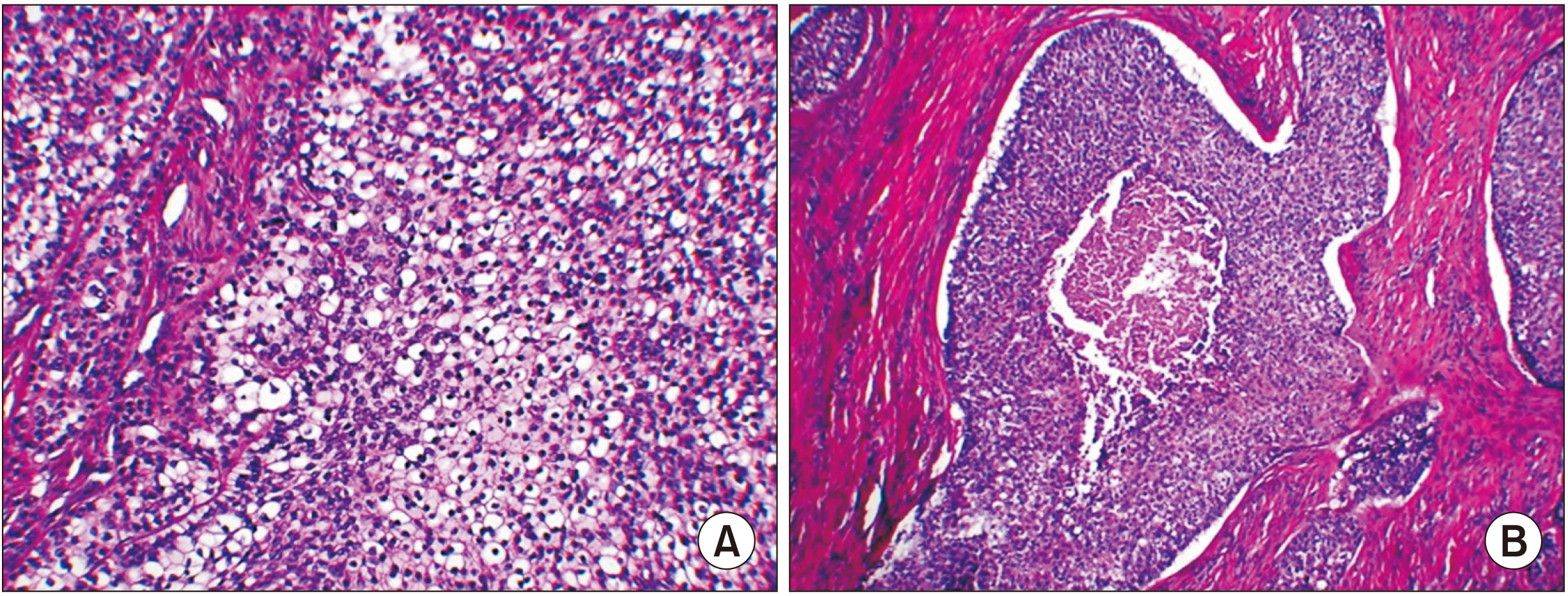
Fig. 8 Histopathologic findings of main mass. A. Abnormal differentiation of cells and cell island patterns was observed. Multiple clear cells showed dynamic mitosis as well as hyperchromatism, which made it possible to diagnose malignant tumors, clear cell odontogenic carcinoma (H&E staining, ×200). B. Histological finding of malignant tumor (H&E staining, ×100).
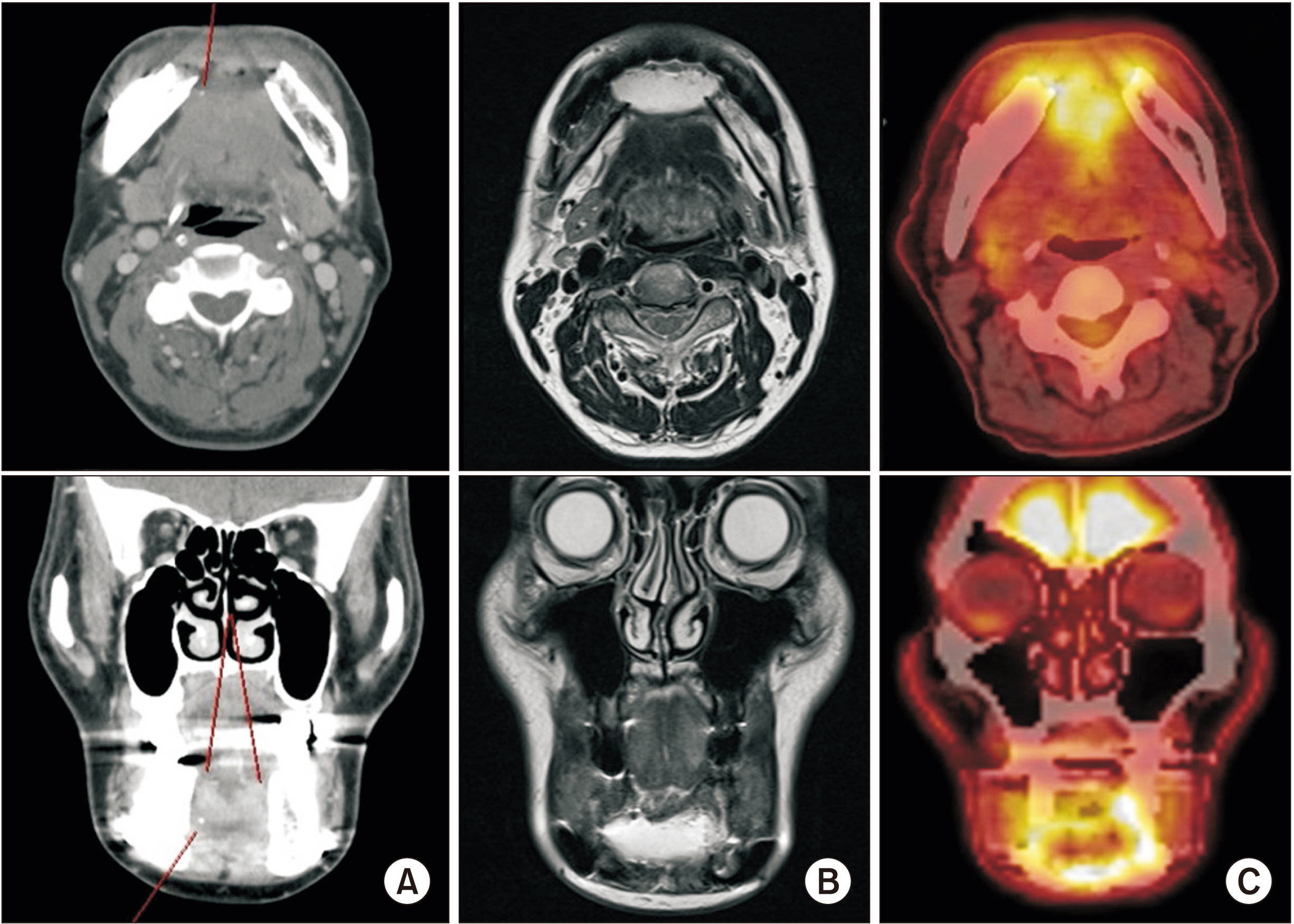
Fig. 9 Radiographs after 1st operation. A. Computed tomography (face) image. Ill-defined enhancing lesion at superior aspect of mandibular anterior, possibly involving both genioglossus muscles. B. Facial magnetic resonance image showed ill-defined enhancement at both genioglossus, hyoglossus muscle and diffuse swelling of the anteior aspect of mandibulectomy site. C. Abnormally increased fluorodeoxyglucose uptake was observed in mandibulectomy site.
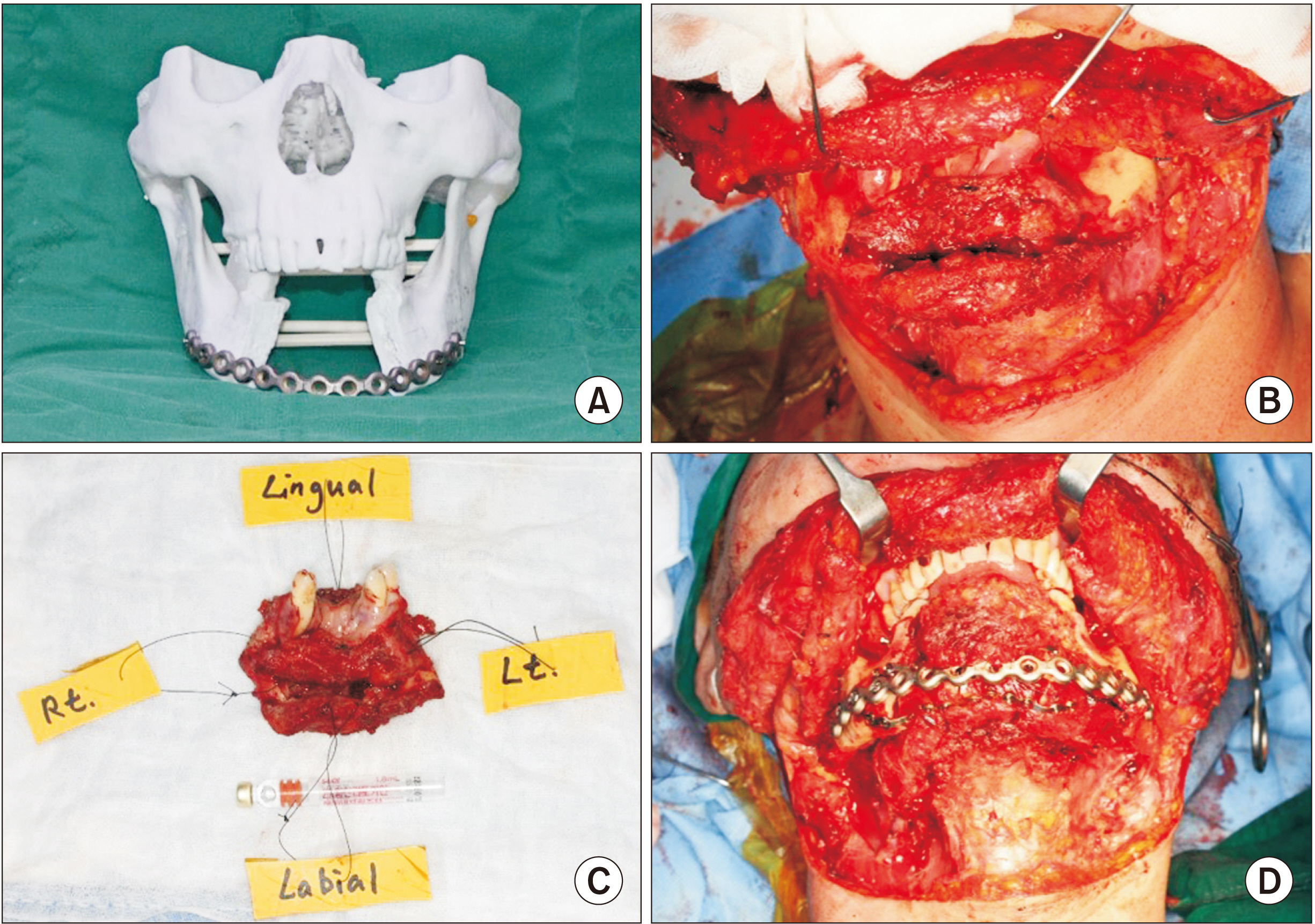
Fig. 10 Surgical procedure of 2nd operation. A. Rapid prototype model of mandible. B. Segmental mandibulectomy with both supraomohyoid neck dissection (SOHND). C. Main mass. D. Mandibular reconstruction with fibula free flap with reconstruction plate and mini plates. Performed with segmental mandibulectomy with both SOHND included Levels I-III and mandible reconstruction with left fibula free flap.
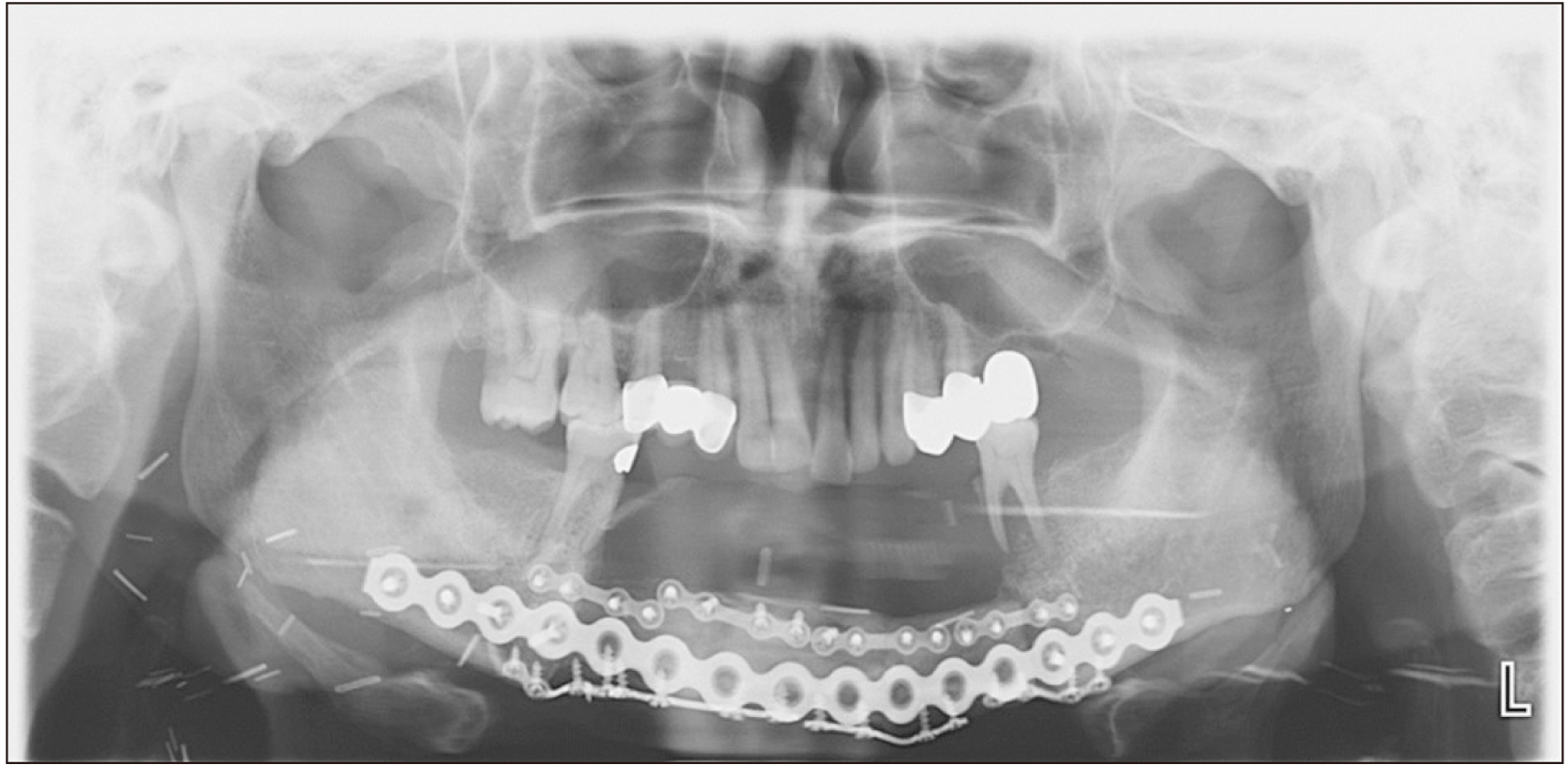
Fig. 11 Panoramic radiograph of after surgery. No recurrence was observed during reconstruction in favor of the mandible.
Reference
-
References
1. Candia J, Fernández A, Kraemer K. 2016; Survival and mortality from oral cancer by anatomical location. A narrative review. J Oral Res. 5:35–42. https://doi.org/10.17126/joralres.2016.007. DOI: 10.17126/joralres.2016.007.
Article2. Sankaranarayanan R. 1990; Oral cancer in India: an epidemiologic and clinical review. Oral Surg Oral Med Oral Pathol. 69:325–30. https://doi.org/10.1016/0030-4220(90)90294-3. DOI: 10.1016/0030-4220(90)90294-3. PMID: 2179801.
Article3. Wu S, Han J, Li WQ, Li T, Qureshi AA. 2013; Basal-cell carcinoma incidence and associated risk factors in U.S. women and men. Am J Epidemiol. 178:890–7. https://doi.org/10.1093/aje/kwt073. DOI: 10.1093/aje/kwt073. PMID: 23828250. PMCID: PMC3775544.
Article4. Woods TR, Cohen DM, Islam MN, Kratochvil FJ, Stewart JC, Reeder SL, et al. 2014; Intraoral basal cell carcinoma, a rare neoplasm: report of three new cases with literature review. Head Neck Pathol. 8:339–48. https://doi.org/10.1007/s12105-013-0505-5. DOI: 10.1007/s12105-013-0505-5. PMID: 24202723. PMCID: PMC4126916.
Article5. Koutlas IG, Koch CA, Vickers RA, Brouwers FM, Vortmeyer AO. 2009; An unusual ostensible example of intraoral basal cell carcinoma. J Cutan Pathol. 36:464–70. https://doi.org/10.1111/j.1600-0560.2008.01059.x. DOI: 10.1111/j.1600-0560.2008.01059.x. PMID: 19278434.
Article6. Kim M, Cho E, Kim JY, Kim HS, Nam W. 2014; Clear cell odontogenic carcinoma mimicking a cystic lesion: a case of misdiagnosis. J Korean Assoc Oral Maxillofac Surg. 40:199–203. https://doi.org/10.5125/jkaoms.2014.40.4.199. DOI: 10.5125/jkaoms.2014.40.4.199. PMID: 25247151. PMCID: PMC4170665.
Article7. Ebert CS Jr, Dubin MG, Hart CF, Chalian AA, Shockley WW. 2005; Clear cell odontogenic carcinoma: a comprehensive analysis of treatment strategies. Head Neck. 27:536–42. https://doi.org/10.1002/hed.20181. DOI: 10.1002/hed.20181. PMID: 15772956.
Article8. Shah JP, Gil Z. 2009; Current concepts in management of oral cancer--surgery. Oral Oncol. 45:394–401. https://doi.org/10.1016/j.oraloncology.2008.05.017. DOI: 10.1016/j.oraloncology.2008.05.017. PMID: 18674952. PMCID: PMC4130348.
Article9. Erdmann D, Giessler GA, Bergquist GE, Bruno W, Young H, Heitmann C, et al. 2004; [Free fibula transfer. Analysis of 76 consecutive microsurgical procedures and review of the literature]. Chirurg. 75:799–809. German. https://doi.org/10.1007/s00104-004-0833-9. DOI: 10.1007/s00104-004-0833-9. PMID: 15138656.
Article10. Wallace CG, Chang YM, Tsai CY, Wei FC. 2010; Harnessing the potential of the free fibula osteoseptocutaneous flap in mandible reconstruction. Plast Reconstr Surg. 125:305–14. https://doi.org/10.1097/PRS.0b013e3181c2bb9d. DOI: 10.1097/PRS.0b013e3181c2bb9d. PMID: 20048622.
Article11. Harjani B, Singh RK, Pal US, Singh G. 2012; Locking v/s non-locking reconstruction plates in mandibular reconstruction. Natl J Maxillofac Surg. 3:159–65. https://doi.org/10.4103/0975-5950.111371. DOI: 10.4103/0975-5950.111371. PMID: 23833491. PMCID: PMC3700150.
Article12. Park HK, Kim TS, Geum DH, Yoon SY, Song JM, Hwang DS, et al. 2015; Mandibular intraosseous squamous cell carcinoma lesion associated with odontogenic keratocyst: a case report. J Korean Assoc Oral Maxillofac Surg. 41:78–83. https://doi.org/10.5125/jkaoms.2015.41.2.78. DOI: 10.5125/jkaoms.2015.41.2.78. PMID: 25922819. PMCID: PMC4411732.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sequential treatment from mandibulectomy to reconstruction on mandibular oral cancer – Case review I: mandibular ramus and angle lesion of primary intraosseous squamous cell carcinoma
- Mandibular intraosseous squamous cell carcinoma lesion associated with odontogenic keratocyst: a case report
- A Case of Basaloid Squamous Cell Carcinoma Occurring in the Mobile Tongue
- Squamous cell carcinoma arising in an odontogenic cyst
- Gasserian Ganglion and Mandibular Nerve Block for the Patient with Mouth Floor Cancer: A case report
