Brain Tumor Res Treat.
2021 Apr;9(1):16-20. 10.14791/btrt.2021.9.e5.
Delayed Hyponatremia after Transsphenoidal Surgery for Pituitary Adenomas: A Single Institutional Experience
- Affiliations
-
- 1Department of Neurosurgery, Yonsei University College of Medicine, Seoul, Korea
- 2Department of Neurosurgery, Ewha Woman’s University College of Medicine, Seoul, Korea
- 3Pituitary Tumor Center, Severance Hospital, Seoul, Korea
- 4Yonsei Endocrine Research Institute, Yonsei University College of Medicine, Seoul, Korea
- KMID: 2515077
- DOI: http://doi.org/10.14791/btrt.2021.9.e5
Abstract
- Background
Hyponatremia is a common complication after transsphenoidal surgery (TSS) for pituitary adenomas. This study retrospectively reviewed various clinical factors of pituitary adenoma patients who underwent TSS and aimed to identify possible risk factors of postoperative hyponatremia.
Methods
Total 1,343 patients who underwent TSS for their pituitary adenomas in a single institution were enrolled to this study. We identified and analyzed 93 patients (6.9%) with postoperative hyponatremia and compared them with other 1,250 patients in a control group. Patients’ age, sex, tumor extent based on the modified Hardy classification, tumor size and hormonal type of the tumors were analyzed in comparison between two groups. The results of pre- and post-operative combined pituitary function test and their comparison were analyzed to elucidate a possible association between postoperative hyponatremia and hypopituitarism.
Results
The onset of postoperative hyponatremia was 7.8 days after surgery (range: postoperative day 3-13). The initial level of serum sodium (Na) level at the start of treatment was 123.5 mmol/L (range: 114-131 mmol/L) and the duration of treatment was 2.7 days (range: 1-9 days). Female predominance was evident in the hyponatremia group (77.4% vs. 61.4%, p=0.02). Preoperative hypopituitarism (58.5% vs. 71.5%, p=0.007) and postoperative hypocortisolism (33.7% vs. 23.4%, p=0.029) were related to postoperative hyponatremia. Other pre- and post-operative clinical factors were not associated with postoperative hyponatremia.
Conclusion
Postoperative hyponatremia is a common complication after TSS and is potentially fatal. Female patients were more likely to develop delayed hyponatremia. We demonstrated possible associations of delayed postoperative hyponatremia with preoperative and postoperative pituitary functions, but the mechanism behind it should be further investigated.
Figure
-
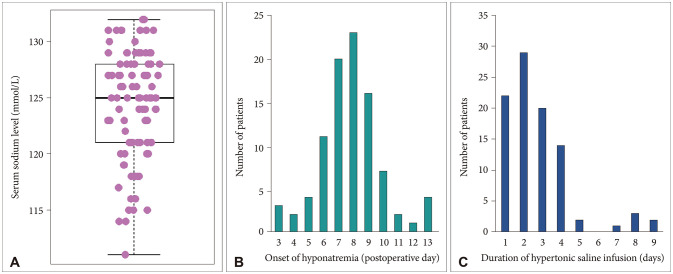
Fig. 1 Characteristics of hyponatremia patients. A: Initial serum sodium level right at the onset of postoperative hyponatremia is 124.3±4.8 mmol/L. B: Onset of delayed hyponatremia is 7.8 days after surgery. C: Hypertonic saline infusion is administrated for 2.7 days.
Reference
-
1. Olson BR, Gumowski J, Rubino D, Oldfield EH. Pathophysiology of hyponatremia after transsphenoidal pituitary surgery. J Neurosurg. 1997; 87:499–507. PMID: 9322839.2. Olson BR, Rubino D, Gumowski J, Oldfield EH. Isolated hyponatremia after transsphenoidal pituitary surgery. J Clin Endocrinol Metab. 1995; 80:85–91. PMID: 7829644.3. Sane T, Rantakari K, Poranen A, Tähtelä R, Välimäki M, Pelkonen R. Hyponatremia after transsphenoidal surgery for pituitary tumors. J Clin Endocrinol Metab. 1994; 79:1395–1398. PMID: 7962334.4. Sata A, Hizuka N, Kawamata T, Hori T, Takano K. Hyponatremia after transsphenoidal surgery for hypothalamo-pituitary tumors. Neuroendocrinology. 2006; 83:117–122. PMID: 16864995.5. Taylor SL, Tyrrell JB, Wilson CB. Delayed onset of hyponatremia after transsphenoidal surgery for pituitary adenomas. Neurosurgery. 1995; 37:649–653. discussion 653–4. PMID: 8559292.6. Zada G, Liu CY, Fishback D, Singer PA, Weiss MH. Recognition and management of delayed hyponatremia following transsphenoidal pituitary surgery. J Neurosurg. 2007; 106:66–71. PMID: 17236489.7. Cusick JF, Hagen TC, Findling JW. Inappropriate secretion of antidiuretic hormone after transsphenoidal surgery for pituitary tumors. N Engl J Med. 1984; 311:36–38. PMID: 6727963.8. Murty GE, Lamballe P, Welch AR. Early inappropriate secretion of antidiuretic hormone after trans-sphenoidal pituitary adenomectomy. J Laryngol Otol. 1990; 104:894–895. PMID: 2266317.9. Whitaker SJ, Meanock CI, Turner GF, et al. Fluid balance and secretion of antidiuretic hormone following transsphenoidal pituitary surgery. A preliminary series. J Neurosurg. 1985; 63:404–412. PMID: 4020468.10. Hensen J, Henig A, Fahlbusch R, Meyer M, Boehnert M, Buchfelder M. Prevalence, predictors and patterns of postoperative polyuria and hyponatraemia in the immediate course after transsphenoidal surgery for pituitary adenomas. Clin Endocrinol (Oxf). 1999; 50:431–439. PMID: 10468901.11. Kelly DF, Laws ER Jr, Fossett D. Delayed hyponatremia after transsphenoidal surgery for pituitary adenoma. Report of nine cases. J Neurosurg. 1995; 83:363–367. PMID: 7616287.12. Kinoshita Y, Tominaga A, Arita K, et al. Post-operative hyponatremia in patients with pituitary adenoma: post-operative management with a uniform treatment protocol. Endocr J. 2011; 58:373–379. PMID: 21467692.13. Lee JI, Cho WH, Choi BK, Cha SH, Song GS, Choi CH. Delayed hyponatremia following transsphenoidal surgery for pituitary adenoma. Neurol Med Chir (Tokyo). 2008; 48:489–492. discussion 492–4. PMID: 19029775.14. Kim EH, Oh MC, Kim SH. Application of low-field intraoperative magnetic resonance imaging in transsphenoidal surgery for pituitary adenomas: technical points to improve the visibility of the tumor resection margin. Acta Neurochir (Wien). 2013; 155:485–493. PMID: 23318686.15. Kim J, Yoon SJ, Moon JH, et al. Clinical significance of radical surgery in the treatment of silent corticotroph adenoma. J Korean Neurosurg Soc. 2019; 62:114–122. PMID: 30630298.16. Oh MC, Kim EH, Kim SH. Coexistence of intracranial aneurysm in 800 patients with surgically confirmed pituitary adenoma. J Neurosurg. 2012; 116:942–947. PMID: 22304451.17. Spasovski G, Vanholder R, Allolio B, et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Nephrol Dial Transplant. 2014; 29 Suppl 2:i1–i39.18. Verbalis JG, Goldsmith SR, Greenberg A, et al. Diagnosis, evaluation, and treatment of hyponatremia: expert panel recommendations. Am J Med. 2013; 126(10 Suppl 1):S1–S42.19. Adrogué HJ, Madias NE. Hyponatremia. N Engl J Med. 2000; 342:1581–1589. PMID: 10824078.20. Adams JR, Blevins LS Jr, Allen GS, Verity DK, Devin JK. Disorders of water metabolism following transsphenoidal pituitary surgery: a single institution's experience. Pituitary. 2006; 9:93–99. PMID: 16832585.21. Raff H. Glucocorticoid inhibition of neurohypophysial vasopressin secretion. Am J Physiol. 1987; 252(4 Pt 2):R635–R644. PMID: 3032001.22. Lester MC, Nelson PB. Neurological aspects of vasopressin release and the syndrome of inappropriate secretion of antidiuretic hormone. Neurosurgery. 1981; 8:735–740. PMID: 7279164.23. Ultmann MC, Hoffman GE, Nelson PB, Robinson AG. Transient hyponatremia after damage to the neurohypophyseal tracts. Neuroendocrinology. 1992; 56:803–811. PMID: 1369588.24. Diringer M, Ladenson PW, Borel C, Hart GK, Kirsch JR, Hanley DF. Sodium and water regulation in a patient with cerebral salt wasting. Arch Neurol. 1989; 46:928–930. PMID: 2757534.25. Kern PA, Robbins RJ, Bichet D, Berl T, Verbalis JG. Syndrome of inappropriate antidiuresis in the absence of arginine vasopressin. J Clin Endocrinol Metab. 1986; 62:148–152. PMID: 3940262.26. Wijdicks EF, Ropper AH, Hunnicutt EJ, Richardson GS, Nathanson JA. Atrial natriuretic factor and salt wasting after aneurysmal subarachnoid hemorrhage. Stroke. 1991; 22:1519–1524. PMID: 1835809.27. Kröll M, Juhler M, Lindholm J. Hyponatraemia in acute brain disease. J Intern Med. 1992; 232:291–297. PMID: 1328460.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Experiences of Three Cases of Giant Pituitary Adenoma
- Microsurgical Transsphenoidal Approach for Pituitary Denomas
- Deliberate Two-Staged Endoscopic Endonasal Transsphenoidal Surgery in Large Pituitary Adenomas
- Microsurgical Transsphenoidal Approach in Sellar and Parasellar Lesions
- Incidental Superior Hypophygeal Artery Aneurysm Embedded within Pituitary Adenoma
