Oral Administration of Nonionic Water-Soluble Contrast Media to Treat Meconium Obstruction in Premature Infants: A Preliminary Study
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea
- 2Department of Pediatrics, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea
- KMID: 2513355
- DOI: http://doi.org/10.5385/nm.2021.28.1.22
Abstract
- Purpose
Meconium obstruction of prematurity (MOP) predisposes premature infants to intestinal perforation and prolonged hospitalization if not diagnosed and treated promptly. A standard contrast enema is less effective to treat infants with distal ileal obstructions because the contrast may not reach the obstructed areas. In an effort to avoid risky surgery, we administered oral contrast media to seven clinically diagnosed patients with MOP whose obstructions were not relieved via conventional sonography-guided contrast enema. We retrospectively evaluated whether oral nonionic water-soluble contrast media relieves MOP.
Methods
Seven of 67 premature infants with MOP were administered oral contrast media from June 2015 to January 2019. Patients were followed-up radiographically for bowel distention and evacuation of contrast media after oral administration. We recorded radiographic improvements, meconium evacuation, time to first feeding after oral contrast media administration, maternal history, and neonatal clinical factors.
Results
We evaluated five male and two female infants. The median gestational ages and body weights at birth were 27+5 weeks and 890 g, respectively. Radiography in five infants revealed multiple distended intestinal loops without air-fluid interfaces. Two infants had gasless abdomens, in which only stomach gas was visible. Oral contrast media (median, 2.5 mL) were administered at a median age of 7 days; five infants (5/7, 71.4%) responded to this treatment. The remaining two infants, who had ileal stenosis and hypoganglionosis, were surgically managed. Five infants (5/7, 71.4%) had maternal risk factors, and two (28.6%) were small for gestational age.
Conclusion
Nonionic oral water-soluble contrast medium can serve as a valuable adjunct treatment in premature infants with meconium obstruction.
Figure
-
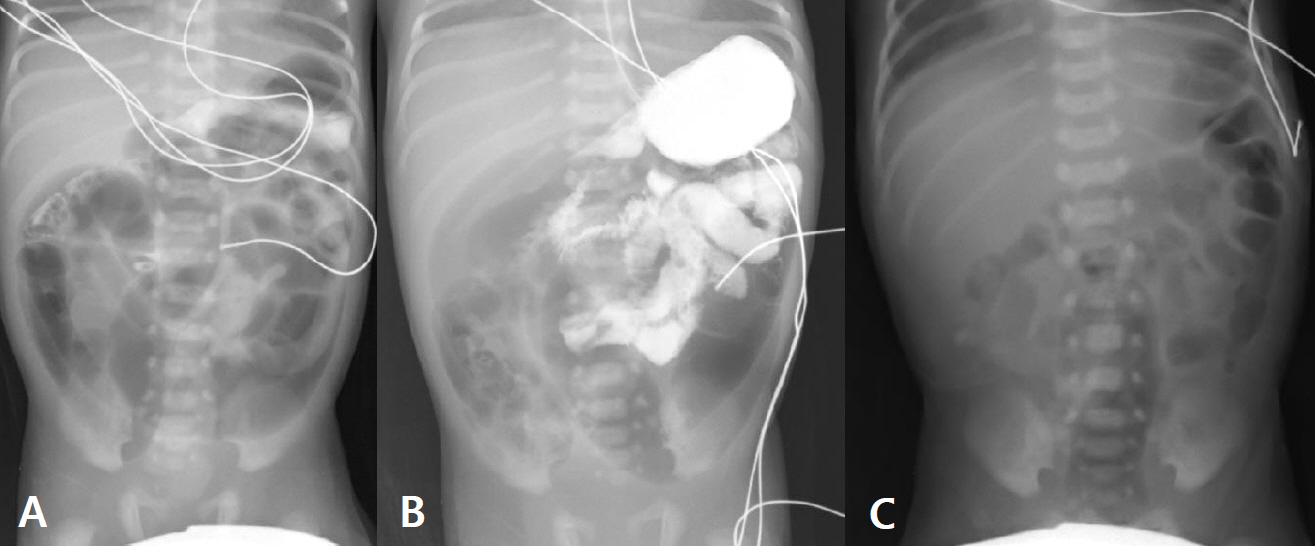
Figure 1. A male infant with a birth weight of 1,490 g was born at 29+3 weeks via emergency cesarean section. He exhibited abdominal distention from the 3rd day after birth. He received daily glycerine enemas and a contrast enema on day 7. The abdominal distention persisted. (A) An abdominal radiograph taken after the contrast enema revealed dilated bowel loops with residual contrast in the colon. (B) Oral omnipaque (10 mL) was given via a gavage tube on day 8 (30+5 gestational weeks, weight 1,440 g). Within 1 day, he passed the meconium and commenced enteral feeding. (C) Two days after oral contrast medium administration, the bowel gas pattern became normal.
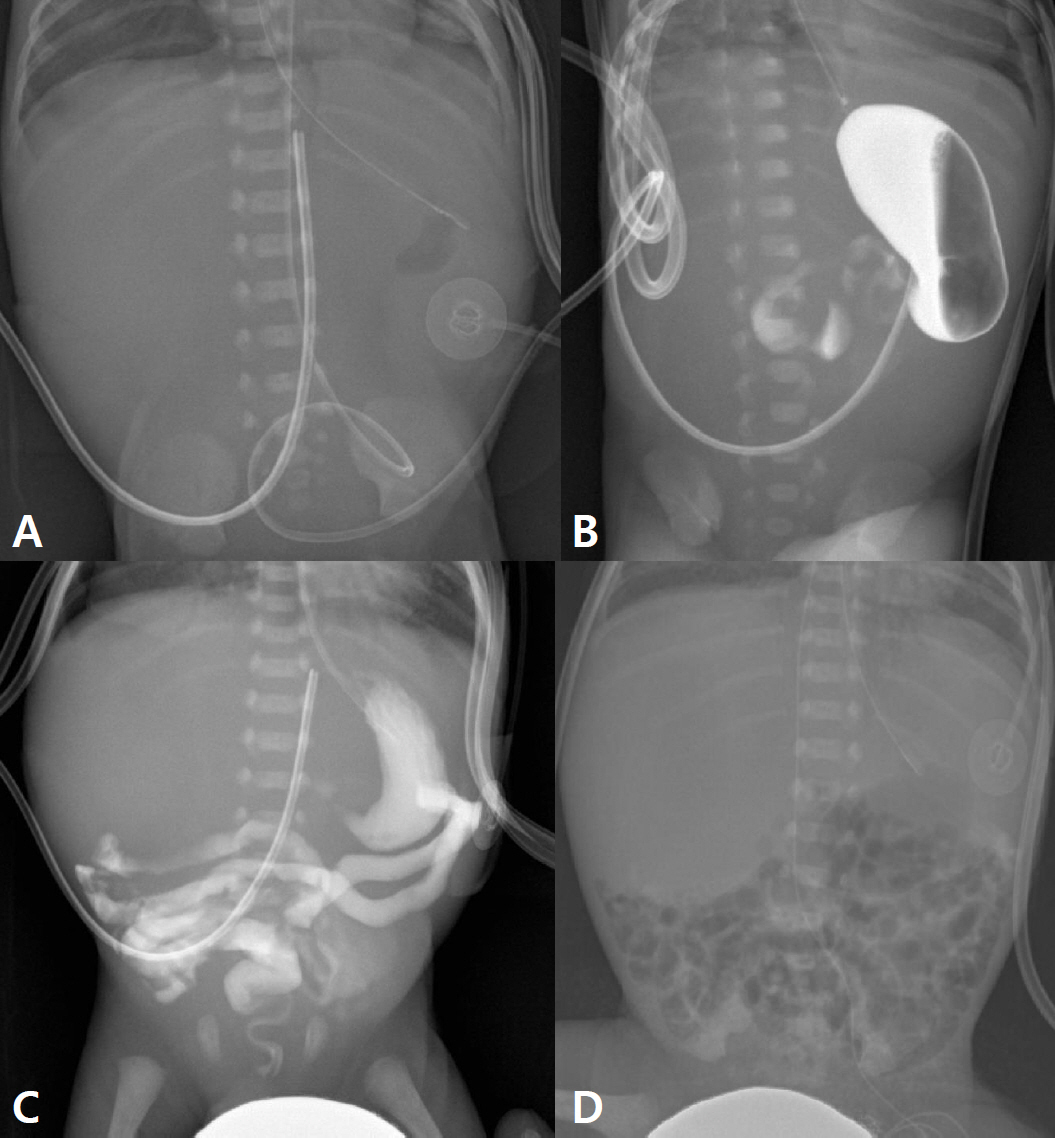
Figure 2. A male infant with a birth weight of 560 g was born at 23+3 weeks via emergency cesarean section. He was not small for gestational age and had no maternal risk factors. After passage of some meconium following a glycerine enema (A), no bowel gas was evident (only stomach gas was present). A degree of abdominal distention, poor meconium passage, and a clinical meconium-associated obstruction were suspected. (B) Approximately 2.5 mL of contrast medium was administrated via a gavage tube on day 13 of life (25 gestational weeks, weight 500 g). (C) A 24-hour follow-up radiograph shows contrast medium into the bowel loops (D) contrast medium was completely evacuated by day 7 after administration, and a follow-up radiograph revealed a normal bowel gas pattern. He passed meconium 2 days after the oral contrast media. Enteral feeding commenced on that day.
Reference
-
1. Garza-Cox S, Keeney SE, Angel CA, Thompson LL, Swischuk LE. Meconium obstruction in the very low birth weight premature infant. Pediatrics. 2004; 114:285–90.2. Greenholz SK, Perez C, Wesley JR, Marr CC. Meconium obstruction in markedly premature infant. J Pediatr Surg. 1996; 31:117–20.3. Vinograd I, Mogle P, Peleg O, Alpan G, Lernau OZ. Meconium disease in premature infants with very low birth weight. J Pediatr. 1983; 103:963–6.4. Amodio J, Berdon W, Abramson S, Stolar C. Microcolon of prematurity: a form of functional obstruction. AJR Am J Roentgenol. 1986; 146:239–44.5. Burge D, Drewett M. Meconium plug obstruction. Pediatr Surg Int. 2004; 20:108–10.6. Keckler SJ, St Peter SD, Spilde TL, Tsao K, Ostlie DJ, Holcomb GW 3rd, et al. Current significance of meconium plug syndrome. J Pediatr Surg. 2008; 43:896–8.7. Kim YJ, Kim EK, Kim ES, Kim HS, Choi JH, Cheon JE, et al. Recognition, diagnosis and treatment of meconium obstruction in extremely low birth weight infants. Neonatology. 2012; 101:172–8.8. Kubota A, Shiraishi J, Kawahara H, Okuyama H, Yoneda A, Nakai H, et al. Meconium-related ileus in extremely low-birthweight neonates: etiological considerations from histology and radiology. Pediatr Int. 2011; 53:887–91.9. Dimmitt RA, Moss RL. Meconium diseases in infants with very low birth weight. Semin Pediatr Surg. 2000; 9:79–83.10. Krasna IH, Rosenfeld D, Salerno P. Is it necrotizing enterocolitis, microcolon of prematurity, or delayed meconium plug? A dilemma in the tiny premature infant. J Pediatr Surg. 1996; 31:855–8.11. Yoo SY, Jung SH, Eom M, Kim IH, Han A. Delayed maturation of interstitial cells of Cajal in meconium obstruction. J Pediatr Surg. 2002; 37:1758–61.12. Chan KL, Ng SP, Chan KW, Wo YH, Tam PK. Pathogenesis of neonatal necrotizing enterocolitis: a study of the role of intraluminal pressure, age and bacterial concentration. Pediatr Surg Int. 2003; 19:573–7.13. Ein SH, Shandling B, Reilly BJ, Stephens CA. Bowel perforation with nonoperative treatment of meconium ileus. J Pediatr Surg. 1987; 22:146–7.14. Noblett HR. Treatment of uncomplicated meconium ileus by Gastrografin enema: a preliminary report. J Pediatr Surg. 1969; 4:190–7.15. Emil S, Nguyen T, Sills J, Padilla G. Meconium obstruction in extremely low-birth-weight neonates: guidelines for diagnosis and management. J Pediatr Surg. 2004; 39:731–7.16. Goo HW, Kim KS, Kim EA, Pi SY, Yoon CH. Sonography-guided gastrografin enema for meconium plug syndrome in premature newborns: preliminary results. J Korean Radiol Soc. 2004; 50:281–8.17. Cho HH, Cheon JE, Choi YH, Lee SM, Kim WS, Kim IO, et al. Ultrasound-guided contrast enema for meconium obstruction in very low birth weight infants: factors that affect treatment success. Eur J Radiol. 2015; 84:2024–31.18. Carroll AG, Kavanagh RG, Ni Leidhin C, Cullinan NM, Lavelle LP, Malone DE. Comparative effectiveness of imaging modalities for the diagnosis of intestinal obstruction in neonates and infants: a critically appraised topic. Acad Radiol. 2016; 23:559–68.19. Haiden N, Norooz F, Klebermass-Schrehof K, Horak AS, Jilma B, Berger A, et al. The effect of an osmotic contrast agent on complete meconium evacuation in preterm infants. Pediatrics. 2012; 130:e1600–6.20. Copeland DR, St Peter SD, Sharp SW, Islam S, Cuenca A, Tolleson JS, et al. Diminishing role of contrast enema in simple meconium ileus. J Pediatr Surg. 2009; 44:2130–2.21. Karimi A, Gorter RR, Sleeboom C, Kneepkens CM, Heij HA. Issues in the management of simple and complex meconium ileus. Pediatr Surg Int. 2011; 27:963–8.22. Burke MS, Ragi JM, Karamanoukian HL, Kotter M, Brisseau GF, Borowitz DS, et al. New strategies in nonoperative management of meconium ileus. J Pediatr Surg. 2002; 37:760–4.23. Carlyle BE, Borowitz DS, Glick PL. A review of pathophysiology and management of fetuses and neonates with meconium ileus for the pediatric surgeon. J Pediatr Surg. 2012; 47:772–81.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Meconium Obstruction in Very Low Birth Weight Infants
- In vitro study on the anticoagulant effect of the water soluble contrast material: diatrizoate, ioxaglate and iopromide
- Meconium Obstruction Syndrome in Two Extremely Low Birth Weight Infants
- Lumbar myelography with amipaque
- Efficacy of Ultrasound-guided Contrast Enema on Meconium Plug Syndrome in Preterm Infants
