Recurrent parvovirus B19 infection-associated pure red cell aplasia in a kidney transplant patient
- Affiliations
-
- 1Department of Surgery, Seoul National University Hospital, Seoul, Korea
- 2Department of Laboratory Medicine, Seoul National University Hospital, Seoul, Korea
- 3Transplantation Research Institute, Seoul National University College of Medicine, Seoul, Korea
- 4Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea
- 5Transplantation Center, Seoul National University Hospital, Seoul, Korea
- KMID: 2507165
- DOI: http://doi.org/10.4285/kjt.2020.34.3.199
Abstract
- Posttransplant anemia is a common complication after kidney transplantation. Parvovirus B19 (PVB19) infection can induce pure red cell aplasia (PRCA) in immunosuppressed transplant patients. We herein report a case of recurrent PVB19-associated PRCA in a kidney transplant patient. A 49-year-old woman presented with anemia and normal renal function 1 year after a deceased-donor kidney transplantation for immunoglobulin A nephropathy-related end-stage renal disease. She received desensitization therapy, and 2 years later, she underwent transplantation with thymoglobulin induction. Despite repeated red cell transfusion and erythropoietin therapy, her anemia aggravated progressively. Bone marrow biopsy revealed normocytic normochromic PRCA. Real-time polymerase chain reaction detected a high plasma load of PVB19. Administration of intravenous immunoglobulin (IVIG) at 2 g/kg with adjuvant reduction of tacrolimus and discontinuation of myfortic acid effectively treated the anemia. However, the PVB19 load remained high, and PRCA recurred 7 months after the initial IVIG treatment. Tacrolimus was switched to cyclosporine in the second IVIG treatment, which successfully improved PRCA and reduced the PVB19 load. Our case suggested that PVB19-associated PRCA should be suspected when persistent anemia is observed in kidney transplant patients with heavy immunosuppression and that PVB19-associated PRCA can recur in the presence of persistent PVB19 viremia.
Keyword
Figure
-
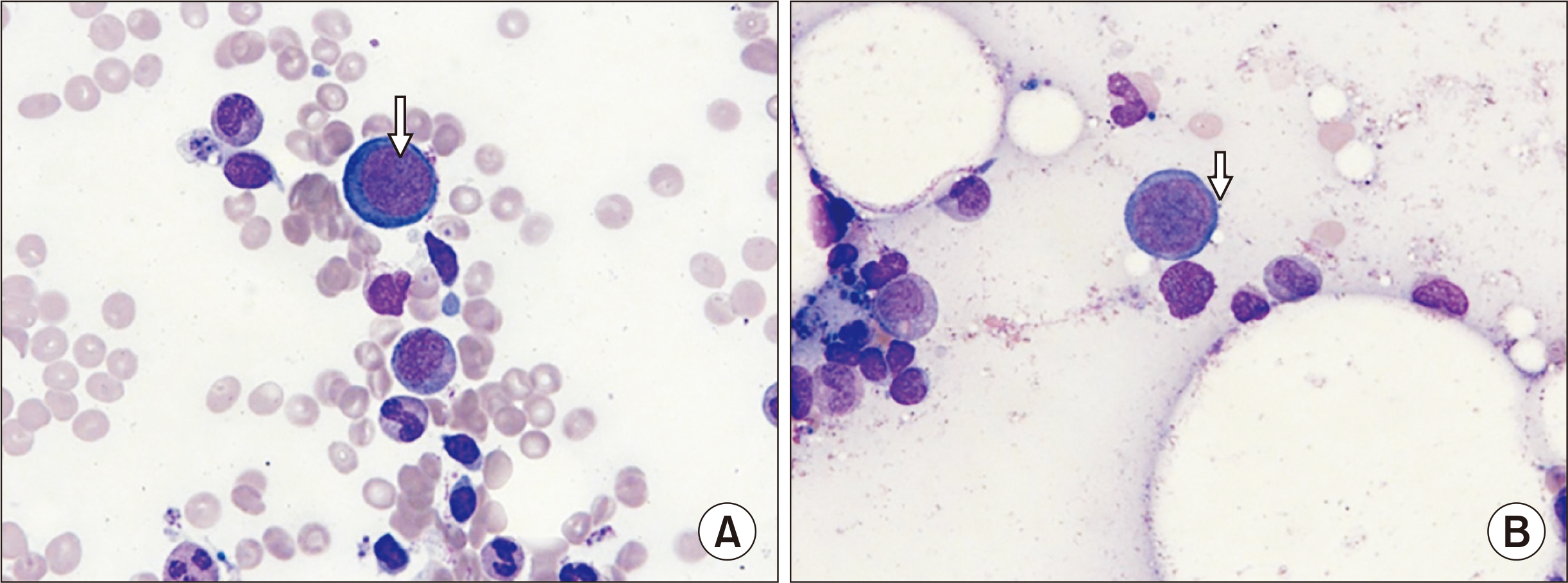
Fig. 1 Bone marrow aspiration findings. Wright-Giemsa staining (×1,000) images of bone marrow aspiration smears showing (A) giant pronormoblasts with nuclear viral inclusion bodies (nucleoli-like, eosinophilic inclusion body, arrow) and (B) giant pronormoblasts with “dog ear” cytoplasmic projections (arrow).
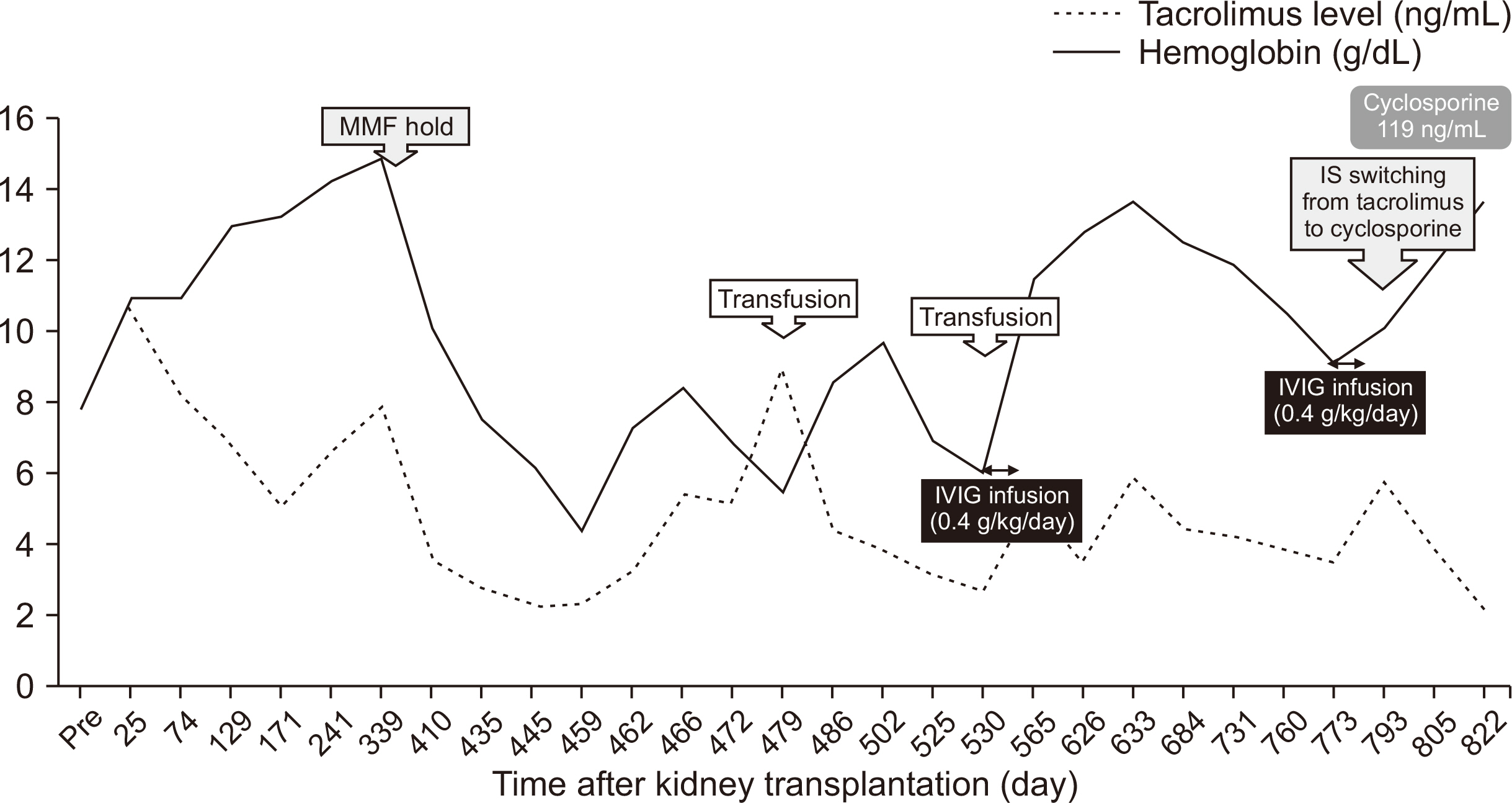
Fig. 2 Changes in blood cell count after kidney transplantation. The patient’s hemoglobin level dropped from 14.0 g/dL at 12 months posttransplant to 7.4 g/dL at 14 months posttransplant. Despite erythropoietin treatment, anemia progressed to 4.2 g/dL, requiring two cycles of red blood cell transfusion. Intravenous immunoglobulin (IVIG) treatment initiated at 17 months posttransplant normalized her hemoglobin level at 19 months posttransplant. However, anemia recurred at 24 months posttransplant, and the second IVIG treatment initiated at 25 months Posttransplant successfully improved her anemia. IS, immunosuppressants; MMF, mycophenolate mofetil.
Reference
-
1. Vanrenterghem Y. 2004; Anaemia after renal transplantation. Nephrol Dial Transplant. 19 Suppl 5:V54–8. DOI: 10.1093/ndt/gfh1057. PMID: 15284361. PMCID: PMC7479824.
Article2. Yorgin PD, Scandling JD, Belson A, Sanchez J, Alexander SR, Andreoni KA. 2002; Late post-transplant anemia in adult renal transplant recipients: an under-recognized problem? Am J Transplant. 2:429–35. DOI: 10.1034/j.1600-6143.2002.20506.x. PMID: 12123208.
Article3. Pabisiak K, Stępniewska J, Ciechanowski K. 2019; Pure red cell aplasia after kidney transplantation: parvovirus B19 culprit or coincidence? Ann Transplant. 24:123–31. DOI: 10.12659/AOT.913663. PMID: 30833537. PMCID: PMC6419532.
Article4. Choi SH, Chang SP, Won JC, Lee JS, Chi HS, Yang WS, et al. 2002; A case of persistent anemia in a renal transplant recipient: association with parvovirus B19 infection. Scand J Infect Dis. 34:71–5. DOI: 10.1080/003655402753395247. PMID: 11874173.
Article5. Ki CS, Kim IS, Kim JW, Lee NY, Kim SH, Lee KW, et al. 2005; Incidence and clinical significance of human parvovirus B19 infection in kidney transplant recipients. Clin Transplant. 19:751–5. DOI: 10.1111/j.1399-0012.2005.00415.x. PMID: 16313320.
Article6. Geetha D, Zachary JB, Baldado HM, Kronz JD, Kraus ES. 2000; Pure red cell aplasia caused by Parvovirus B19 infection in solid organ transplant recipients: a case report and review of literature. Clin Transplant. 14:586–91. DOI: 10.1034/j.1399-0012.2000.140612.x. PMID: 11127313. PMCID: PMC4146984.
Article7. Rao KR, Patel AR, Anderson MJ, Hodgson J, Jones SE, Pattison JR. 1983; Infection with parvovirus-like virus and aplastic crisis in chronic hemolytic anemia. Ann Intern Med. 98:930–2. DOI: 10.7326/0003-4819-98-6-930. PMID: 6859707.
Article8. Ager EA, Chin TD, Poland JD. 1966; Epidemic erythema infectiosum. N Engl J Med. 275:1326–31. DOI: 10.1056/NEJM196612152752402. PMID: 5923532.
Article9. Crabol Y, Terrier B, Rozenberg F, Pestre V, Legendre C, Hermine O, et al. 2013; Intravenous immunoglobulin therapy for pure red cell aplasia related to human parvovirus b19 infection: a retrospective study of 10 patients and review of the literature. Clin Infect Dis. 56:968–77. DOI: 10.1093/cid/cis1046. PMID: 23243178.
Article10. Eid AJ, Brown RA, Patel R, Razonable RR. 2006; Parvovirus B19 infection after transplantation: a review of 98 cases. Clin Infect Dis. 43:40–8. DOI: 10.1086/504812. PMID: 16758416.
Article11. Bonvicini F, Bua G, Manaresi E, Gallinella G. 2015; Antiviral effect of cidofovir on parvovirus B19 replication. Antiviral Res. 113:11–8. DOI: 10.1016/j.antiviral.2014.11.004. PMID: 25446336.
Article12. Baek CH, Kim H, Yang WS, Han DJ, Park SK. 2017; Risk factors and long-term outcomes of parvovirus B19 infection in kidney transplant patients. Transpl Infect Dis. 19:e12754. DOI: 10.1111/tid.12754. PMID: 28741797.
Article13. Kaya B, Paydas S. 2019; Recurrence of pure red cell aplasia in a kidney transplant recipient due to reactivation of parvovirus B19 infection despite two cycles of intravenous immunoglobulin therapy. Exp Clin Transplant. 17(Suppl 1):195–7. DOI: 10.6002/ect.MESOT2018.P63. PMID: 30777553.
Article14. Pinto V, Grandy J, Zambrano P, Corta B, Salas P, Salgado I, et al. 2008; Severe anemia from parvovirus b19 infection in pediatric renal transplant recipients: two case reports. Transplant Proc. 40:3261–4. DOI: 10.1016/j.transproceed.2008.03.127. PMID: 19010248.
Article15. Eid AJ, Chen SF. AST Infectious Diseases Community of Practice. 2013; Human parvovirus B19 in solid organ transplantation. Am J Transplant. 13 Suppl 4:201–5. DOI: 10.1111/ajt.12111. PMID: 23465012.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Parvovirus B19-induced Pure Red Cell Aplasia in a Liver Transplant Recipient
- Spontaneous Subcapsular Hematoma on a Transplanted Kidney
- A Case of Pure Red Cell Aplasia Due to Parvovirus B19 Infection in a Renal Transplant Recipient
- A Case of Immunoglobulin Therapy for Pure Red Cell Aplasia Induced by Parvovirus B19
- Pure Red Cell Aplasia Due to Parvovirus B19 in Renal Transplants
