Biomechanical considerations for uprighting impacted mandibular molars
- Affiliations
-
- 1Department of Orthodontics and Dentofacial Orthopedics, Nagasaki University Graduate School of Biomedical Sciences, Nagasaki, Japan
- KMID: 2504144
- DOI: http://doi.org/10.4041/kjod.2020.50.4.268
Abstract
- This case report demonstrates two different uprighting mechanics separately applied to mesially tipped mandibular first and second molars. The biomechanical considerations for application of these mechanisms are also discussed. For repositioning of the first molar, which was severely tipped and deeply impacted, a novel cantilever mechanics was used. The molar tube was bonded in the buccolingual direction to facilitate insertion of a cantilever from the buccal side. By twisting the distal end of the cantilever, sufficient uprighting moment was generated. The mesial end of the cantilever was hooked over the miniscrew placed between the canine and first premolar, which could prevent exertion of an intrusive force to the anterior portion of the dentition as a side effect. For repositioning of the second molar, an uprighting mechanics using a compression force with two step bends incorporated into a nickel-titanium archwire was employed. This generated an uprighting moment as well as a distal force acting on the tipped second molar to regain the lost space for the first molar and bring it into its normal position. This epoch-making uprighting mechanics could also minimize the extrusion of the molar, thereby preventing occlusal interference by increasing interocclusal clearance between the inferiorly placed two step bends and the antagonist tooth. Consequently, the two step bends could help prevent occlusal interference. After 2 years and 11 months of active treatment, a desirable Class I occlusion was successfully achieved without permanent tooth extraction.
Figure
-
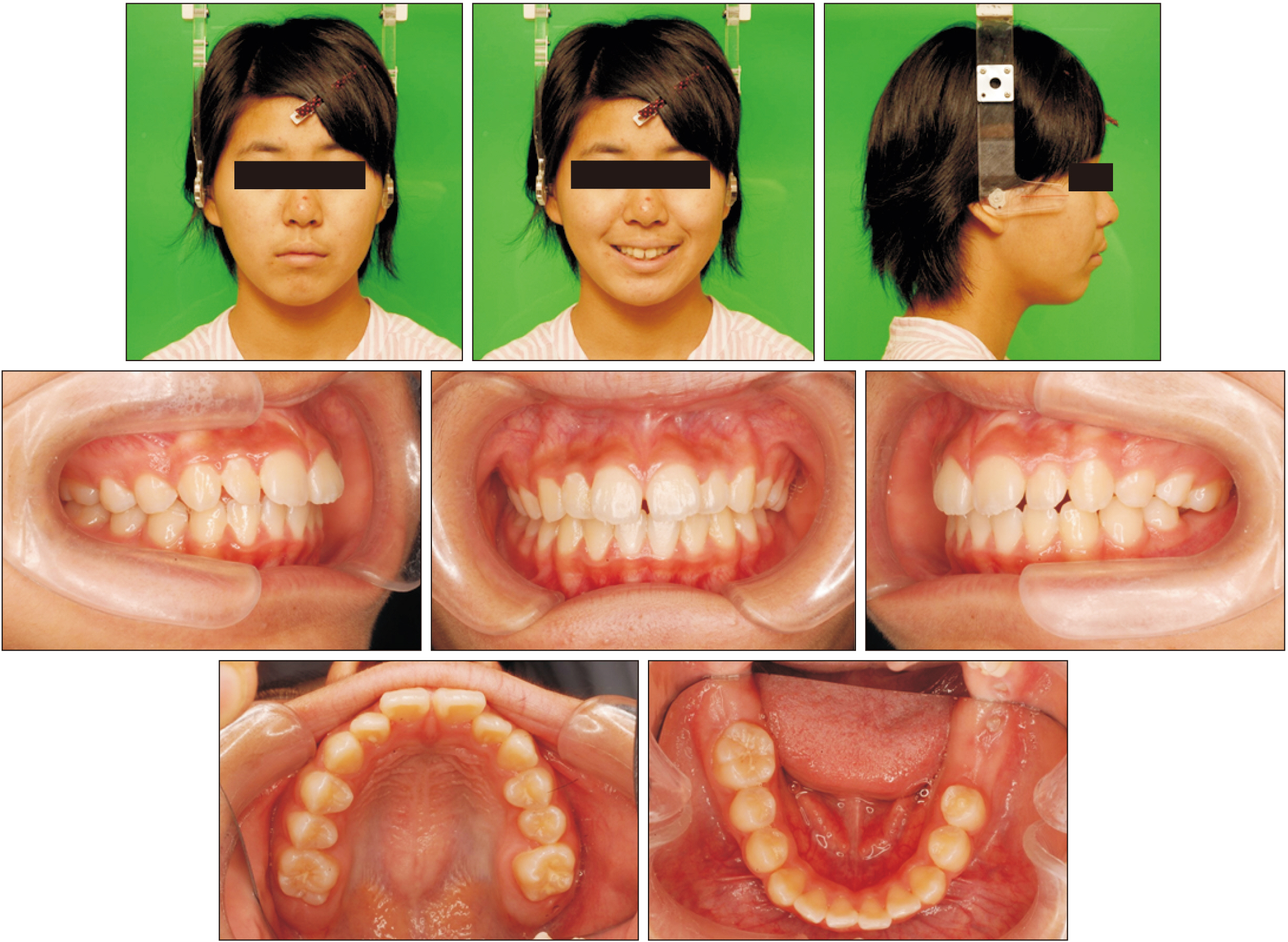
Figure 1 Pretreatment facial and intraoral photographs.
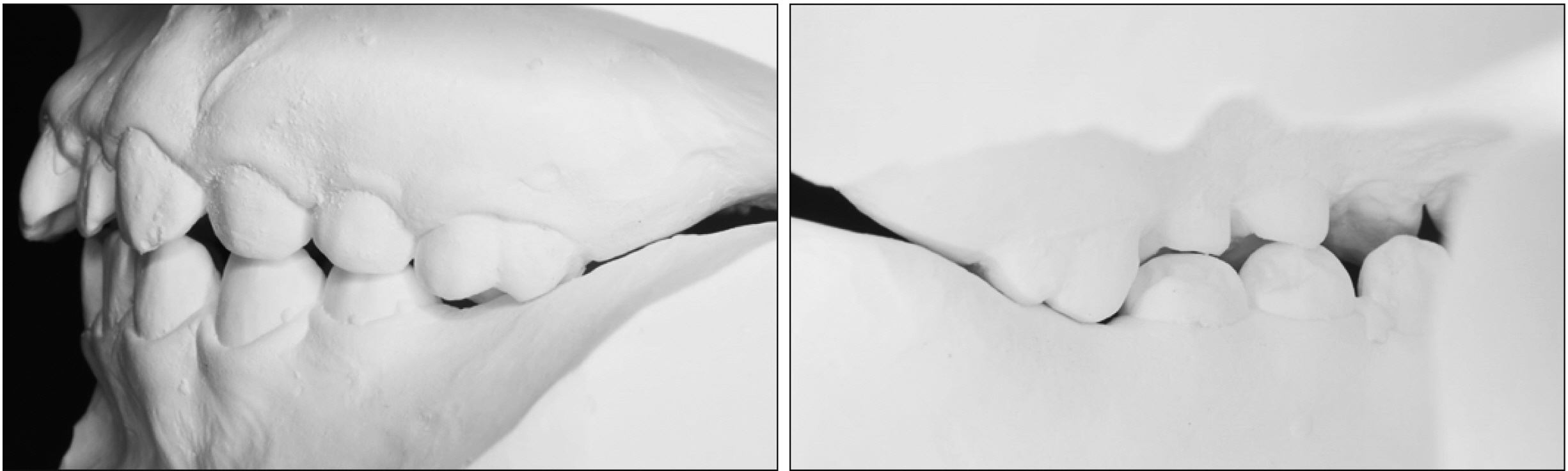
Figure 2 Pretreatment study model: over-erupted maxillary left first molar occluding onto the mandibular gingiva.

Figure 3 Pretreatment. A, Panoramic radiograph; B, lateral cephalometric radiographs; C, cephalometric superimposition.

Figure 4 Treatment objectives. A, Treatment plan for repositioning of the molars. B, Schematic diagram of treatment objectives. The maxillary first molar is intruded by 3 mm. The mandibular first and second molars are uprighted by 60° and 30°, and extruded by 6 mm and 1 mm, respectively. U6, Upper first molar; L6, lower first molar; L7, lower second molar; CR, center of resistance.
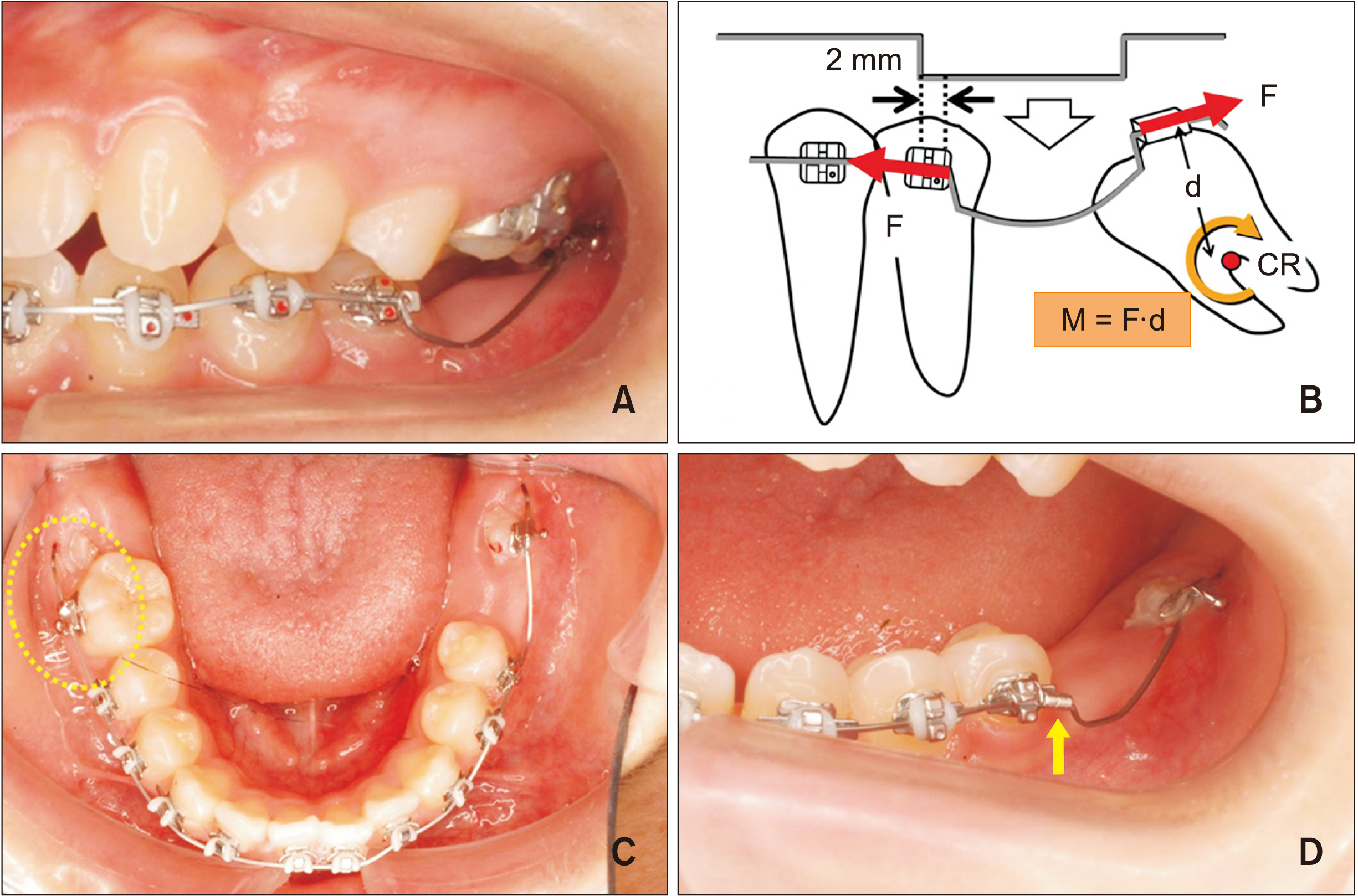
Figure 5 Progress and force system for uprighting the mandibular second molar. A, Left mandibular second molar uprighting using a 0.016 × 0.016-inch (in) square nickel-titanium (NiTi) archwire with two step bends whose distance was 2 mm wider than the inter-bracket distance between the left second premolar and the second molar. B, Force system acting on the second molar when the uprighting mechanics using a compression force is employed. Two step bends, whose distance is 2 mm wider than the inter-bracket distance between the second premolar and second molar, are incorporated into a 0.016 × 0.016-in square NiTi archwire. When the two step bends incorporated into the archwire are squeezed and engaged into the brackets, a mesial force to the second premolar and a distal force to the second molar are generated. Then, an uprighting moment (M), whose magnitude is the product of the magnitude of the distal force (F) and the perpendicular distance (d) from its line of force to the center of resistance (CR), is produced. C, The length of the excess wire distal to the buccal tube on the right first molar was used to shift the archwire to the left to reactivate the two step bends without removing the archwire (circle). D, A crimpable stop placed on the archwire just mesial to the anterior step bend (arrow).

Figure 6 Treatment mechanics for uprighting of the left mandibular first molar. A, B, A small molar tube bonded buccolingually and an arrow indicates the insertion direction of the cantilever. C, Force system acting on the first molar and miniscrew when the cantilever mechanics is employed. A dotted line indicates the cantilever in its passive state, and a solid line in its active state. When the cantilever is activated, a moment of couple (MC) to tip the molar distally, an extrusive force on the molar tube, and an intrusive force on the miniscrew are generated. The uprighting moment acting on the molar is the sum of MC and the moment of force (MF). D, The cantilever passes under the main archwire to avoid slipping buccally and the mesial end of the cantilever hooked over the miniscrew (circle).
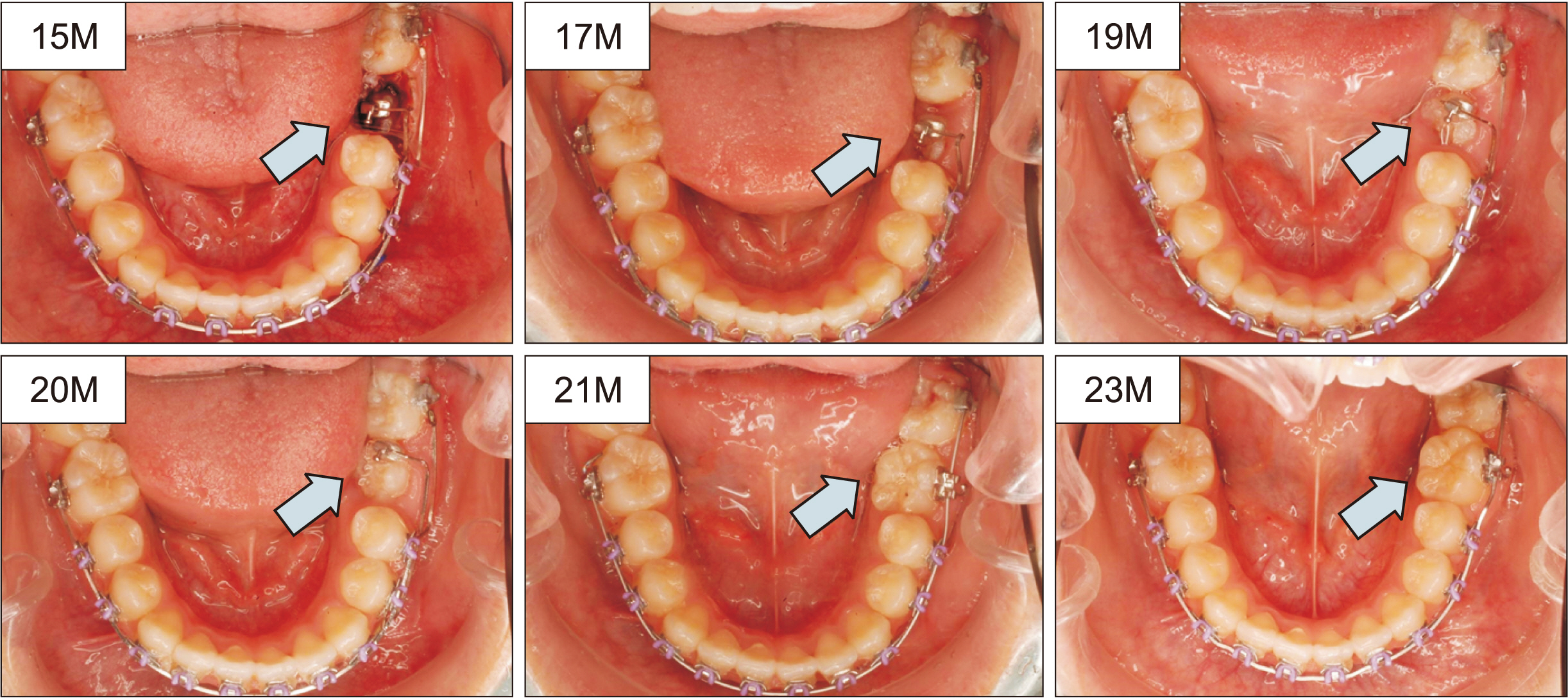
Figure 7 The treatment sequence for uprighting of the left mandibular first molar (the blue arrow indicated) (15M; 15 months after orthodontic treatment started). Progress is shown at treatment times in months. The archwire was 0.017 × 0.022-inch (in) Elgiloy and a 0.016 × 0.022-in stainless steel cantilever was used for uprighting the left mandibular first molar. At 21 months, a molar tube was bonded on the buccal surface of the first molar and the 0.018-in nickel-titanium archwire was engaged for its alignment.
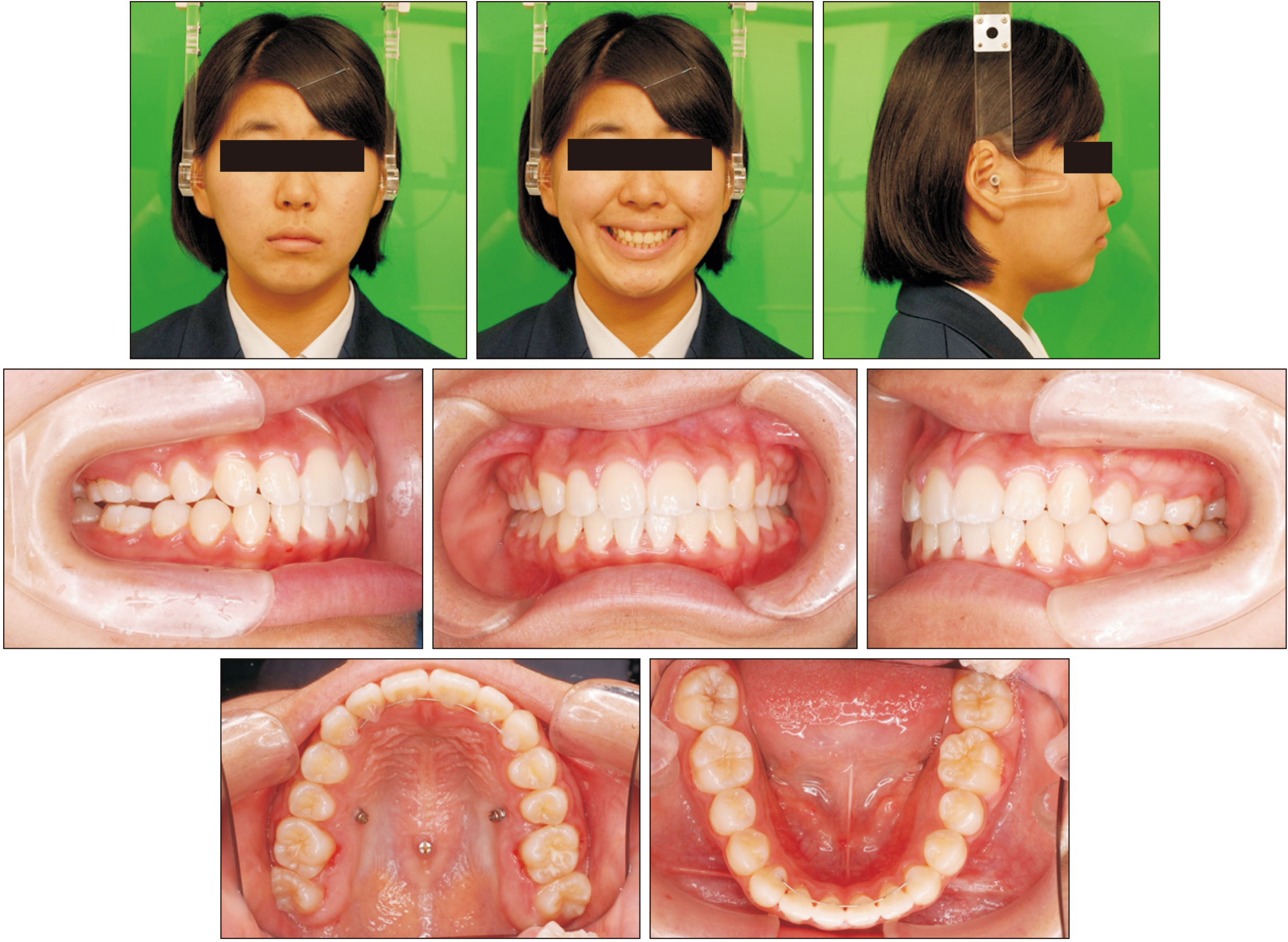
Figure 8 Posttreatment facial and intraoral photographs.

Figure 9 Posttreatment study model: the left posterior occlusion is normalized.
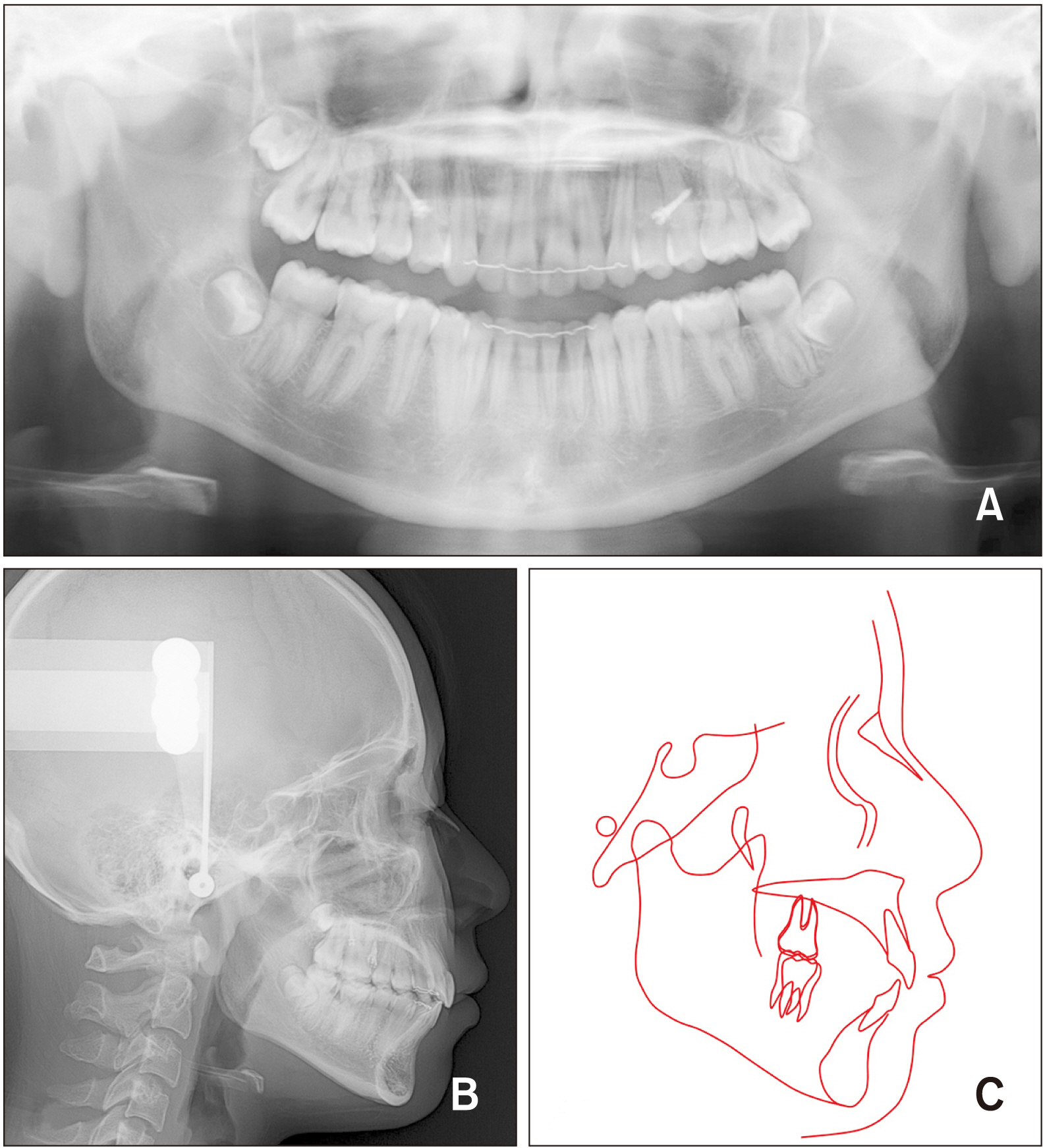
Figure 10 Posttreatment. A, Panoramic radiograph; B, lateral cephalometric radiograph; C, tracing.

Figure 11 Superimposition of the pretreatment and posttreatment lateral cephalometric radiographs. A, On the sella-nasion plane at sella; B, on the palatal plane at anterior nasal spine; C, on the mandibular plane at the menton. Black line, Pretreatment; Red line, posttreatment.

Figure 12 Intraoral photographs obtained 2 years after orthodontic treatment.
Reference
-
1. Dachi SF, Howell FV. 1961; A survey of 3,874 routine full-month radiographs. II. A study of impacted teeth. Oral Surg Oral Med Oral Pathol. 14:1165–9. DOI: 10.1016/0030-4220(61)90204-3.2. Chu FC, Li TK, Lui VK, Newsome PR, Chow RL, Cheung LK. 2003; Prevalence of impacted teeth and associated pathologies--a radiographic study of the Hong Kong Chinese population. Hong Kong Med J. 9:158–63.3. Keris EY, Bozkaya S, Öztürk M, Güngör K. 2016; Prevalence and characteristics of impacted permanent molars in a Turkish subpopulation. J Oral Maxillofac Radiol. 4:45–9. DOI: 10.4103/2321-3841.196345.
Article4. Roberts WW 3rd, Chacker FM, Burstone CJ. 1982; A segmental approach to mandibular molar uprighting. Am J Orthod. 81:177–84. DOI: 10.1016/0002-9416(82)90051-3. PMID: 6960706.5. Kuhlberg AJ. 2001; Cantilever springs: force system and clinicalapplications. Semin Orthod. 7:150–9. DOI: 10.1053/sodo.2001.26689.
Article6. Lee KJ, Park YC, Hwang WS, Seong EH. 2007; Uprighting mandibular second molars with direct miniscrew anchorage. J Clin Orthod. 41:627–35. PMID: 18175884.7. Shapira Y, Borell G, Nahlieli O, Kuftinec MM. 1998; Uprighting mesially impacted mandibular permanent second molars. Angle Orthod. 68:173–8. DOI: 10.1043/0003-3219(1998)068<0173:UMIMPS>2.3.CO;2. PMID: 9564428.8. Majourau A, Norton LA. 1995; Uprighting impacted second molars with segmented springs. Am J Orthod Dentofacial Orthop. 107:235–8. DOI: 10.1016/S0889-5406(95)70137-0. PMID: 7879754.
Article9. Fu PS, Wang JC, Chen CH, Huang TK, Tseng CH, Hung CC. 2012; Management of unilaterally deep impacted first, second, and third mandibular molars. Angle Orthod. 82:565–71. DOI: 10.2319/062411-409.1. PMID: 21988519.
Article10. Resch D. 2003; Clinical management of unilaterally impacted mandibular first and second molars. J Clin Orthod. 37:162–4. quiz 148PMID: 12723332.11. Mehrotra R, Mehrotra A, Mistry J. 2014; Management of unilaterally impacted permanent mandibular first, second and third molars. J Ind Orthod Soc. 48:419–28. DOI: 10.1177/0974909820140611S.
Article12. Lau CK, Whang CZ, Bister D. 2013; Orthodontic uprighting of severely impacted mandibular second molars. Am J Orthod Dentofacial Orthop. 143:116–24. DOI: 10.1016/j.ajodo.2011.09.012. PMID: 23273367.
Article13. Raveli TB, Raveli DB, de Mathias Almeida KC, Pinto ADS. 2017; Molar uprighting: a considerable and safe decision to avoid prosthetic treatment. Open Dent J. 31:466–75. DOI: 10.2174/1874210601711010466. PMID: 29114332. PMCID: PMC5646130.
Article14. Fu PS, Wang JC, Wu YM, Huang TK, Chen WC, Tseng YC, et al. 2012; Impacted mandibular second molars. Angle Orthod. 82:670–5. DOI: 10.2319/102111-656.1. PMID: 22229822.
Article15. Sawicka M, Racka-Pilszak B, Rosnowska-Mazurkiewicz A. 2007; Uprighting partially impacted permanent second molars. Angle Orthod. 77:148–54. DOI: 10.2319/010206-461R.1. PMID: 17029525.
Article16. Magkavali-Trikka P, Emmanouilidis G, Papadopoulos MA. 2018; Mandibular molar uprighting using orthodontic miniscrew implants: a systematic review. Prog Orthod. 19:1. DOI: 10.1186/s40510-017-0200-2. PMID: 29308540. PMCID: PMC5756736.
Article17. Park HS, Kyung HM, Sung JH. 2002; A simple method of molar uprighting with micro-implant anchorage. J Clin Orthod. 36:592–6. PMID: 12428309.18. Giancotti A, Muzzi F, Santini F, Arcuri C. 2003; Miniscrew treatment of ectopic mandibular molars. J Clin Orthod. 37:380–3. PMID: 14515557.19. Giancotti A, Arcuri C, Barlattani A. 2004; Treatment of ectopic mandibular second molar with titanium miniscrews. Am J Orthod Dentofacial Orthop. 126:113–7. DOI: 10.1016/j.ajodo.2003.08.025. PMID: 15224068.
Article20. Barros SE, Janson G, Chiqueto K, Ferreira E, Rösing C. 2018; Expanding torque possibilities: a skeletally anchored torqued cantilever for uprighting "kissing molars". Am J Orthod Dentofacial Orthop. 153:588–98. DOI: 10.1016/j.ajodo.2017.12.006. PMID: 29602351.
Article21. Mah SJ, Won PJ, Nam JH, Kim EC, Kang YG. 2015; Uprighting mesially impacted mandibular molars with 2 miniscrews. Am J Orthod Dentofacial Orthop. 148:849–61. DOI: 10.1016/j.ajodo.2015.07.027. PMID: 26522046.
Article22. Nienkemper M, Ludwig B, Kanavakis G, Pauls A, Wilmes B, Drescher D. 2016; Uprighting mesially impacted lower third molars with skeletal anchorage. J Clin Orthod. 50:420–6. PMID: 27575886.23. Melo AC, Duarte da Silva R, Shimizu RH, Campos D, Andrighetto AR. 2013; Lower molar uprighting with miniscrew anchorage: direct and indirect anchorage. Int J Orthod Milwaukee. 24:9–14. PMID: 24358649.24. Miyawaki S, Koyama I, Inoue M, Mishima K, Sugahara T, Takano-Yamamoto T. 2003; Factors associated with the stability of titanium screws placed in the posterior region for orthodontic anchorage. Am J Orthod Dentofacial Orthop. 124:373–8. DOI: 10.1016/S0889-5406(03)00565-1.
Article25. Cheng SJ, Tseng IY, Lee JJ, Kok SH. 2004; A prospective study of the risk factors associated with failure of mini-implants used for orthodontic anchorage. Int J Oral Maxillofac Implants. 19:100–6.26. Kravitz ND, Kusnoto B. 2007; Risks and complications of orthodontic miniscrews. Am J Orthod Dentofacial Orthop. 131:S43–51. DOI: 10.1016/j.ajodo.2006.04.027. PMID: 17448385.
Article27. Lai TT, Chen MH. 2014; Factors affecting the clinical success of orthodontic anchorage: experience with 266 temporary anchorage devices. J Dent Sci. 9:49–55. DOI: 10.1016/j.jds.2013.02.010.
Article28. Chang CH, Lin JS, Roberts WH. 2018; Ramus screws: the ultimate solution for lower impacted molars. Semin Orthod. 24:135–54. DOI: 10.1053/j.sodo.2018.01.012.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Analysis Of The Relationships Between The Root Curvatures Of The Mandibular Third Molars And Their Locations On The Mandible
- Orthodontic Traction of the Impacted Mandibular Third Molars to Replace Severely Resorbed Mandibular Second Molars
- Evaluation of strategic uprighting of the mandibular molars using an orthodontic miniplate and a nickel-titanium reverse curve arch wire: Preliminary cephalometric study
- Prevalence of missing and impacted third molars in adults aged 25 years and above
- Orthodontic upright treatment for mesioangular impacted lower second molar
