Orthodontic upright treatment for mesioangular impacted lower second molar
- Affiliations
-
- 1Gajirunhan S Dental Clinic, Gimpo, Republic of Korea.
- 2Graduate School of Chosun University, Gwangju, Republic of Korea.
- 3Geoje Dental Clinic, Geoje, Republic of Korea.
- 4Department of Orthodontics, School of Dentistry, Chosun University, Gwangju, Republic of Korea. 022bracket@gmail.com
- KMID: 2377056
- DOI: http://doi.org/10.14368/jdras.2017.33.1.25
Abstract
- The lower 2(nd) molar eruption is beginning to mesiolingually, then rotate to distobuccally so it has a tendency to be tilted and impacted mesially. Signs and symptoms of impacted 2(nd) molar are similar to impacted 3(rd) molar's. However, treatment plan for impacted 2nd molar is different from that of impacted 3(rd)'s. The former is the preservation and uprighting of 2(nd) molar so that it could act to recovery of mastication, symmetrical facial growth, maintaining the symmetry of dental arch, stable occlusion, while the latter is the extraction of tooth. If the uprighting treatment is planned, most proper protocol of treatment and the additional treatment opition should be applied with consideration for it's crown exposure, present of 3(rd) molar which interrupt the uprighting process, extrusion of opposite tooth. Although it could not improve the esthetic result, it could prevent many dental problems. Therefore, uprighting for impacted lower 2(nd) molar is meaningful treatment.
Figure
-
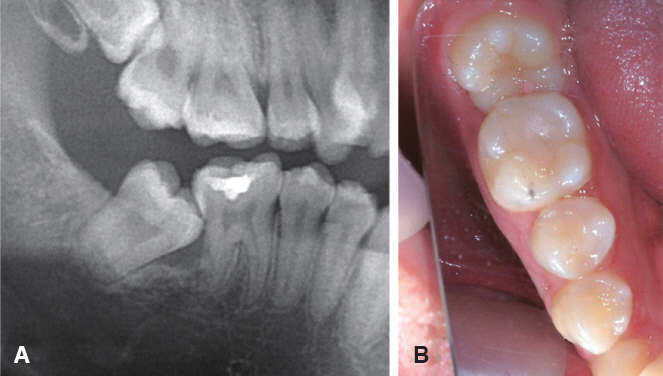
Fig. 1 Pretreatment panoramic radiograph (A), intraoral photograph (B). There were shown mesial angulated impaction of #47. Especially, alveolar bone resorption was shown at #47 mesial side in panoramic view.
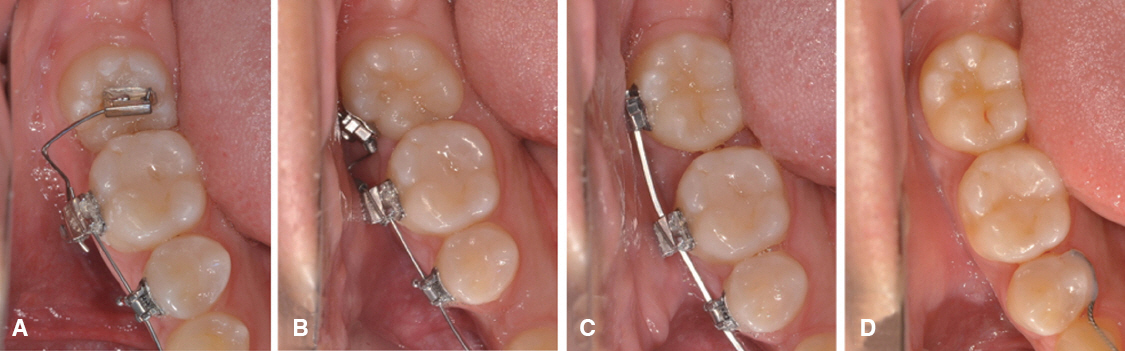
Fig. 2 Intraoral photographs during treat of mesioangulated impaction of #47. Each images was cropped. (A) .018 standard tube was bonded on #47 occlusal surface by rotated 90°then, auxillary wire was engaged. (B) .022 molar tube was bonded on #47 buccal surface at rightly position. A chicane NiTi spring was delivered for continuous uprighting process. (C) After gross uprighting process, continuous main arch wire was engaged. (D) After treatment. The mesioangulated #47 was uprighted to right position.
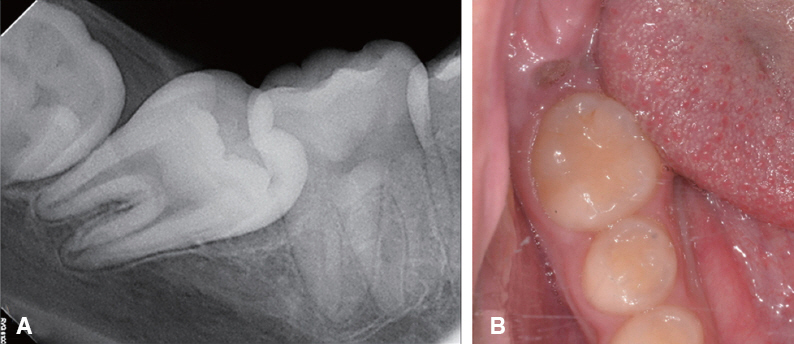
Fig. 3 Pretreatment periapical radiograph (A), intraoral photograph (B). Periapical radiograph was shown mesial angulated impaction of #47, #48 was developed at distal side of #47. Remarkable periodotal or carious lesion were not shown. The ulcerative lesion by erupted #47’s distal cusp was shown at #46 distal side in intraoral photograph.

Fig. 4 Intraoral photographs, periapical radiographs during treat of mesioangulated impaction of #47. Each intraoral photographs were cropped. (A) & (B) After gingivectomy, occlusal surface of #47 was exposed. A lingual button was bonded on most mesial side, Modified Humpery appliance was cemented on #46 and tractional elastic module was engaged. (C) & (D) After gross uprighting process, lingual button, Humpery appliance’s lever arm were removed. .018 standard tube was bonded on right position of #47. Partial .016 × .022 SS wire and open coil was delivered. There were no periodontal problem, root resorption of #47. #48 was developed normally at #47 distal area. (E) After treatment. The mesioangulated #47 was uprighted to right position. Slightly gingival swelling was shown at #47 distal surface.

Fig. 5 Pretreatment panoramic radiograph (A), intraoral photograph (B). Panoramic radiograph was shown mesial angulated impaction of #47, #48 was developing at closed distal side of #47.

Fig. 6 Intraoral photographs, panoramic radiographs during treat of mesioangulated impaction of #47. Each images were cropped. (A) 1 year later after #48 extraction. (B) Mini-implant was inserted at most anterior-inferior border mandibular ramus, then 0.3 mm dead soft SS wire was connected to mini-implant. Elastic chain was engaged between 0.3 mm wire and lingual button that was bonded on #47 occlusal surface. (C) & (D) After gross uprighting process, lingual button, mini-implant were removed, then a .018 standard tube was bonded on right position of #47, continuous arch wire was engaged. (E) MEAW was used at finishing stage. (F) After treatment. The mesioangulated #47 was uprighted to right position.
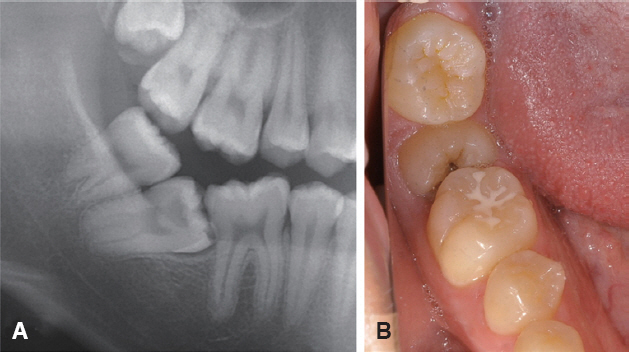
Fig. 7 Pretreatment panoramic radiograph (A), intraoral photograph (B). Panoramic radiograph was shown almost horizontal angulated impaction of #47. Fully developed #48 was erupted at right distal side of #47. It was occluded #17. Deep caries lesion was shown panoramic view, intraoral photograph.
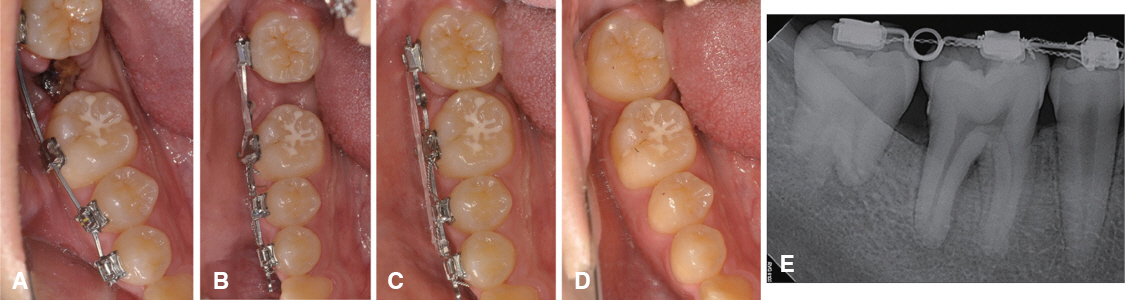
Fig. 8 Intraoral photographs, periapical radiograph during traction of #48. Each intraoral photographs were cropped. (A) After #47 extraction. .022 SWA bracket bonded on #44 - 48, then .016 × .022 Niti was engaged. (B) After initial alignment, .019 × .025 SS with helix loop was engaged for distal tip-back moment during mesial traction procedure by elastic chain. (C) Traction process of #48 was almost finished. (D) After treatment. #48 was tracted to #47’s position. (E) Periapical radiograph after traction of #48. The long axis of #48 was well controlled. However, slightly root resorption was happened.
Reference
-
References
1. Lee HL, Lee KH, La JY, An SY, Kim YH, Lim HS, Lee JW. Eruption guidance of impacted mandibular second molar. J Korean Acad Pediatr Dent. 2012; 39:404–11. DOI: 10.5933/JKAPD.2012.39.4.404.2. Andreasen JO, Peterson J, Laskin DM. Textbook and color atlas of tooth impactions. Copenhagen: Munksgaard;1997. p. 198–216.3. Grover PS, Lorton L. The incidence of unerupted permanent teeth and related clinical cases. Oral Surg Oral Med Oral Pathol. 1985; 59:420–5. DOI: 10.1016/0030-4220(85)90070-2.4. Bondemark L, Tsiopa J. Prevalence of ectopic eruption, impaction, retention and agenesis of the permanent second molar. Angle Orthod. 2007; 77:7738. DOI: 10.2319/072506-306.1. PMID: 17685771.5. Nanci A. Ten Cate’s oral histology: development, structure, and function. 7th ed. St. Louis: Elsevier Health Sciences;2007.6. Fu PS, Wang JC, Wu YM, Huang TK, Chen WC, Tseng YC, Tseng CH, Hung CC. Impacted mandibular second molars. Angle Orthod. 2012; 82:6705. DOI: 10.2319/102111-656.1. DOI: 10.2319/062411-409.1. PMID: 21988519.7. Raghoebar GM, Boering G, Vissink A, Stegenga B. Eruption disturbances of permanent molars: a review. J Oral Pathol Med. 1991; 20:159–66. DOI: 10.1111/j.1600-0714.1991.tb00913.x. PMID: 2061854.8. Sawicka M, Racka-Pilszak B, Rosnowska-Mazurkiewicz A. Uprighting partially impacted permanent second molars. Angle Orthod. 2007; 77:148–54. DOI: 10.2319/010206-461R.1. PMID: 17029525.9. Wellfelt B, Varpio M. Disturbed eruption of the permanent lower second molar: treatment and results. ASDC J Dent Child. 1988; 55:183–9. PMID: 3164337.10. Park HS, Kyung HM, Sung JH. A simple method of molar uprighting with micro-implant anchorage. J Clin Orthod. 2002; 36:592–6. PMID: 12428309.11. Babaji P, Singh V, Chaurasia VR, Jawale MR. Electro surgery in dentistry: report of cases. J Pediatr Dent. 2014; 2:20–4.12. Mavrogiannis M, Ellis J, Seymour RA, Thomason JM. The efficacy of three different surgical techniques in the management of drug induced gingival overgrowth. J Clin Periodontol. 2006; 33:677–82. DOI: 10.1111/j.1600-051X.2006.00968.x.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Orthodontic treatment of molar teeth impacted by local factors
- Orthodontic Traction of the Permanent Molar Using Skeletal Anchorage: A Case Report
- Straight lift technique as an alternative to surgical extraction of an intact, partially impacted mesioangular mandibular third molar
- Orthodontic Traction of the Impacted Mandibular Third Molars to Replace Severely Resorbed Mandibular Second Molars
- Surgical-orthodontic treatment of impacted teeth displaced by unicystic ameloblastoma
