Prolonged hepatic inflow occlusion to reduce bleeding during recipient hepatectomy in living donor liver transplantation
- Choi JU
 1
1 - Hwang S1
- Chung IJ1
- Kang SH1
- Ahn CS1
- Moon DB1
- Ha TY1
- Kim KH1
- Song GW1
- Jung DH1
- Park GC1
- Yoon YI1
- Cho HD1
- Lee SG1
- Affiliations
-
- 1Division of Hepatobiliary Surgery and Liver Transplantation, Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2503783
- DOI: http://doi.org/10.4285/kjt.2020.34.1.55
Abstract
- Background
Living donor liver transplantation (LDLT) causes bleeding in recipients during the careful preservation of most perihilar structures during this surgery. This case-control study aimed to analyze the effect of prolonged hepatic inflow occlusion (PHIO) when applied during recipient hepatectomy in LDLT.
Methods
The study group comprised patients who underwent PHIO with Model for End-Stage Liver Disease (MELD) scores ranging from 26 to 35 (n=20). The following two control groups were selected according to their MELD scores: the low-MELD score group (MELD scores of 15–20, n=40) and the high-MELD score group (MELD scores of 26–35, n=40). Total dissection time for hepatic mobilization and dissection and blood loss during these procedures were compared between the two groups.
Results
In the PHIO study group, mean total dissection time and mean PHIO duration were 226.3±59.4 and 68.2±19.1 minutes, respectively. Twelve patients underwent PHIO twice, and the other eight patients underwent PHIO once. The low-MELD score control group and the PHIO study group showed similar dissection duration (216.0±43.9 vs. 226.3±59.4 minutes, P=0.82) and similar blood loss volume during dissection (2,112.5±1,614.9 vs. 2,350.0±951.9 mL, P=0.17). The high-MELD score control group and the PHIO study group showed similar dissection duration (241.0±41.9 vs. 226.3±59.4 minutes, P=0.71), but the PHIO group showed a significantly lower blood loss during dissection than the high-MELD score group (2,350.0±951.9 vs. 2,815.0±1,813.9 mL, P=0.002). During and after PHIO, no adverse complication was observed, except for transient splanchnic congestion.
Conclusions
Our findings suggest that PHIO is a simple effective method to reduce intraoperative bleeding during hepatic mobilization and dissection during LDLT operation requiring difficult dissection.
Figure
-
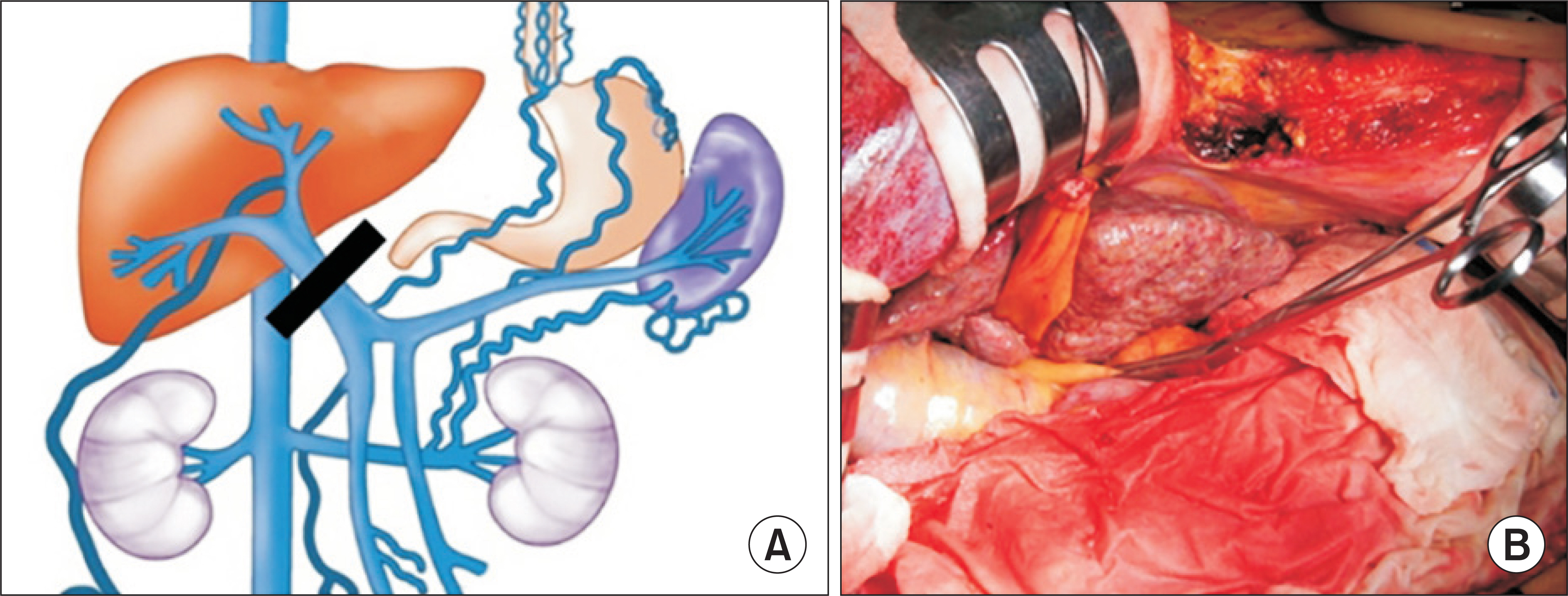
Fig. 1 Concept of prolonged hepatic inflow occlusion. (A) Interruption of the main portal flow and hepatic arterial flow in a patient with liver cirrhosis, and portal hypertension does not induce significant splanchnic congestion because of portal bypass through venous collaterals. Adapted from Choi et al. Ann Hepatobiliary Pancreat Surg 2019;23:61-4 [3]. (B) A curved intestinal clamp is attached to the hepatoduodenal ligament for right liver mobilization.
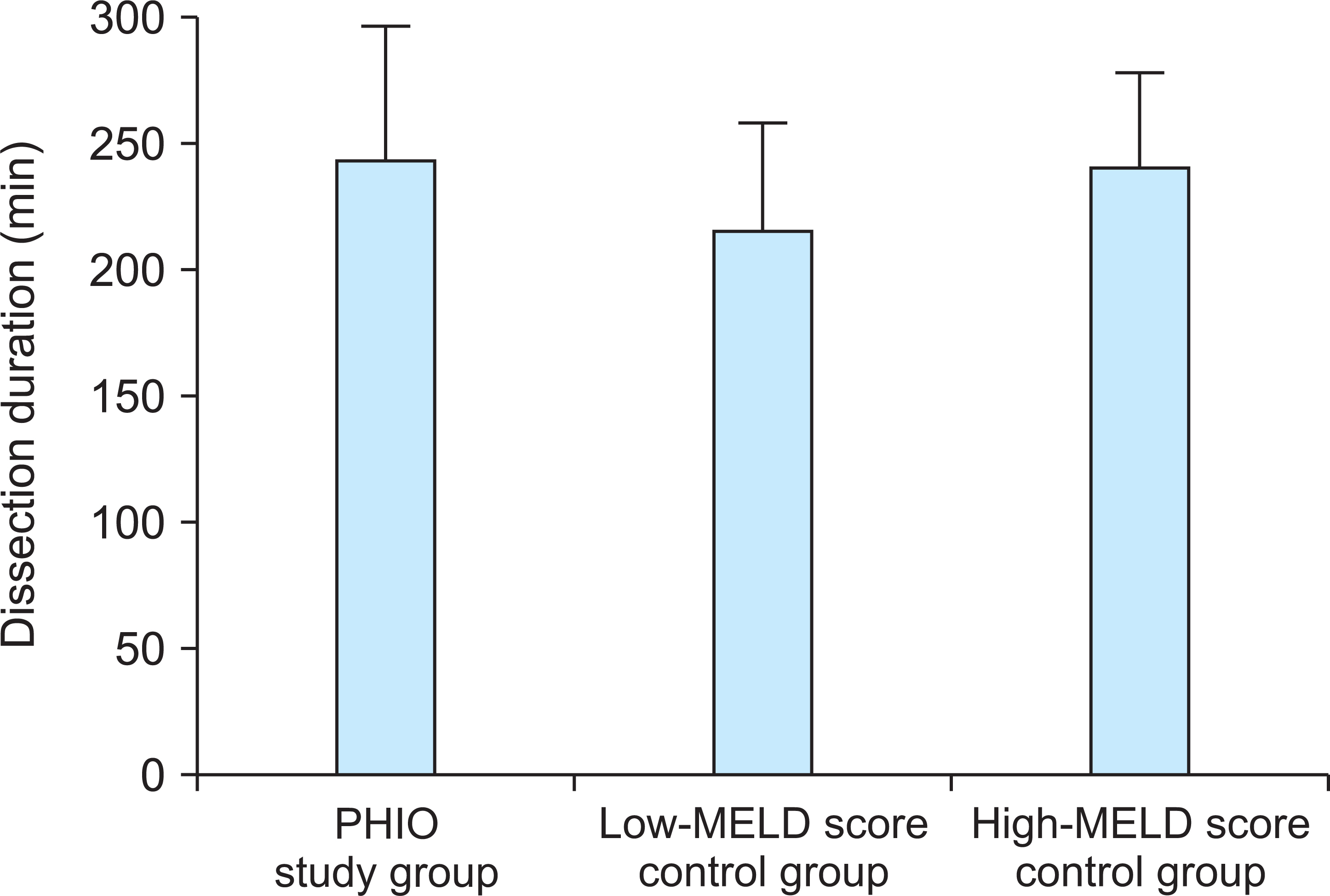
Fig. 2 Comparison of the total liver dissection duration in the prolonged hepatic inflow occlusion (PHIO) study group and two Model for End-Stage Liver Disease (MELD) score control groups.

Fig. 3 Comparison of amount of blood loss during liver dissection in the prolonged hepatic inflow occlusion (PHIO) study group and two Model for End-Stage Liver Disease (MELD) score control groups.
Reference
-
Hwang S., Lee SG., Lee YJ., Sung KB., Park KM., Kim KH, et al. 2006. Lessons learned from 1,000 living donor liver transplantations in a single center: how to make living donations safe. Liver Transpl. 12:920–7. DOI: 10.1002/lt.20734. PMID: 16721780.
ArticleHwang S., Lee SG., Moon DB., Ahn CS., Kim KH., Lee YJ, et al. 2007. Salvage living donor liver transplantation after prior liver resection for hepatocellular carcinoma. Liver Transpl. 13:741–6. DOI: 10.1002/lt.21157. PMID: 17457860.
ArticleChoi JU., Hwang S., Ahn CS., Moon DB., Ha TY., Kim KH, et al. 2019. Prolonged occlusion of the hepatoduodenal ligament to reduce risk of bleeding and tumor spread during recipient hepatectomy for living donor liver transplantation. Ann Hepatobiliary Pancreat Surg. 23:61–4. DOI: 10.14701/ahbps.2019.23.1.61. PMID: 30863809. PMCID: PMC6405371.
ArticleLee KF., Wong J., Cheung SY., Chong CC., Hui JW., Leung VY, et al. 2018. Does intermittent pringle maneuver increase postoperative complications after hepatectomy for hepatocellular carcinoma? A randomized controlled trial. World J Surg. 42:3302–11. DOI: 10.1007/s00268-018-4637-3. PMID: 29696328.
ArticleYoon JU., Byeon GJ., Park JY., Yoon SH., Ryu JH., Ri HS. 2018. Bloodless living donor liver transplantation: risk factors, outcomes, and diagnostic predictors. Medicine (Baltimore). 97:e13581. DOI: 10.1097/MD.0000000000013581. PMID: 30558025. PMCID: PMC6320073.Huang CJ., Cheng KW., Chen CL., Wu SC., Shih TH., Yang SC, et al. 2013. Predictive factors for pediatric patients requiring massive blood transfusion during living donor liver transplantation. Ann Transplant. 18:443–7. DOI: 10.12659/AOT.889293. PMID: 23999839.
ArticlePustavoitau A., Lesley M., Ariyo P., Latif A., Villamayor AJ., Frank SM, et al. 2017. Predictive modeling of massive transfusion requirements during liver transplantation and its potential to reduce utilization of blood bank resources. Anesth Analg. 124:1644–52. DOI: 10.1213/ANE.0000000000001994. PMID: 28426586.
ArticleDonohue CI., Mallett SV. 2015. Reducing transfusion requirements in liver transplantation. World J Transplant. 5:165–82. DOI: 10.5500/wjt.v5.i4.165. PMID: 26722645. PMCID: PMC4689928.
ArticleSteib A., Freys G., Lehmann C., Meyer C., Mahoudeau G. 2001. Intraoperative blood losses and transfusion requirements during adult liver transplantation remain difficult to predict. Can J Anaesth. 48:1075–9. DOI: 10.1007/BF03020372. PMID: 11744582.
ArticleCacciarelli TV., Keeffe EB., Moore DH., Burns W., Chuljian P., Busque S, et al. 1996. Primary liver transplantation without transfusion of red blood cells. Surgery. 120:698–704. DOI: 10.1016/S0039-6060(96)80019-5. PMID: 8862380.
ArticleMassicotte L., Beaulieu D., Roy JD., Marleau D., Vandenbroucke F., Dagenais M, et al. 2009. MELD score and blood product requirements during liver transplantation: no link. Transplantation. 87:1689–94. DOI: 10.1097/TP.0b013e3181a5e5f1. PMID: 19502961.
ArticlePinto MA., Chedid MF., Sekine L., Schmidt AP., Capra RP., Prediger C, et al. 2019. Intraoperative cell salvage with autologous transfusion in liver transplantation. World J Gastrointest Surg. 11:11–8. DOI: 10.4240/wjgs.v11.i1.11. PMID: 30705735. PMCID: PMC6354069.
ArticlePark YK., Kim BW., Wang HJ., Xu W. 2012. Usefulness of the Pinch-Burn-Cut (PBC) technique for recipient hepatectomy in liver transplantation. Korean J Hepatobiliary Pancreat Surg. 16:13–6. DOI: 10.14701/kjhbps.2012.16.1.13. PMID: 26388900. PMCID: PMC4575015.
ArticleLee KW., Joh JW., Kim SJ., Choi SH., Heo JS., Lee HH, et al. 2004. High hilar dissection: new technique to reduce biliary complication in living donor liver transplantation. Liver Transpl. 10:1158–62. DOI: 10.1002/lt.20230. PMID: 15350008.
ArticleScatton O., Brustia R., Belli G., Pekolj J., Wakabayashi G., Gayet B. 2015. What kind of energy devices should be used for laparoscopic liver resection? Recommendations from a systematic review. J Hepatobiliary Pancreat Sci. 22:327–34. DOI: 10.1002/jhbp.213. PMID: 25624116.
ArticlePringle JH. 1908. V. Notes on the arrest of hepatic hemorrhage due to trauma. Ann Surg. 48:541–9. DOI: 10.1097/00000658-190810000-00005. PMID: 17862242. PMCID: PMC1406963.Verran DJ., Gurkan A., Chui AK., Dilworth P., Koorey D., McCaughan G, et al. 2000. Pancreatitis in adult orthotopic liver allograft recipients: risk factors and outcome. Liver Transpl. 6:362–6. DOI: 10.1053/lv.2000.5203. PMID: 10827240.
ArticleCamargo CA Jr Jr., Greig PD., Levy GA., Clavien PA. 1995. Acute pancreatitis following liver transplantation. J Am Coll Surg. 181:249–56. DOI: 10.1097/00007890-198909000-00037. PMID: 7545514.Krokos NV., Karavias D., Tzakis A., Tepetes K., Ramos E., Todo S, et al. 1995. Acute pancreatitis after liver transplantation: incidence and contributing factors. Transpl Int. 8:1–7. DOI: 10.1111/j.1432-2277.1995.tb01698.x. PMID: 7534081. PMCID: PMC2950630.
ArticleLi H., Yang Z., Tian F. 2019. Clinical characteristics and risk factors for sinistral portal hypertension associated with moderate and severe acute pancreatitis: a seven-year single-center retrospective study. Med Sci Monit. 25:5969–76. DOI: 10.12659/MSM.916192. PMID: 31400275. PMCID: PMC6699198.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recipient liver splitting to facilitate piggyback hepatectomy in adult living donor liver transplantation
- Prolonged occlusion of the hepatoduodenal ligament to reduce risk of bleeding and tumor spread during recipient hepatectomy for living donor liver transplantation
- Hepatic Artery Reconstruction Using the Right Gastroepiploic Artery for Hepatic Artery Inflow in a Living Donor Liver Transplantation
- Minimal-incision donor right hepatectomy for living donor liver transplantation
- Anatomical limits in living donor liver transplantation
