Recipient liver splitting to facilitate piggyback hepatectomy in adult living donor liver transplantation
- Affiliations
-
- 1Division of Hepatobiliary Surgery and Liver Transplantation, Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2517296
- DOI: http://doi.org/10.4285/kjt.20.0055
Abstract
- Recipient hepatectomy for an enlarged stony-hard liver is a demanding procedure, thus it is often accompanied by massive blood loss. Recipient liver splitting under prolonged hepatic inflow occlusion would facilitate the piggyback recipient hepatectomy. We herein present a case of recipient liver splitting, which was used for living donor liver transplantation (LDLT). A 48-year-old male patient diagnosed with acute-on-chronic liver failure underwent LDLT. During the recipient operation, the native liver was stony-hard and heavily adherent to the retrohepatic inferior vena cava (IVC). During liver mobilization, diffuse oozing occurred due to disseminated intravascular coagulation. As a change in the concept, we decided to perform in situ liver splitting of the recipient liver to facilitate dissection of the retrohepatic IVC. Under hepatic inflow occlusion, right-left liver splitting was performed along the usual plane of extended left hepatectomy. The procedures time for recipient liver splitting and removal was 60 minutes. A modified right liver graft recovered from his daughter was implanted according to the standard procedures of LDLT. We think that recipient liver splitting is a feasible technical option for coping with difficult recipient hepatectomy, especially in patients with an enlarged stony-hard liver and heavy adhesion around the IVC.
Figure
-

Fig. 1 Preoperative dynamic computed tomography findings. Hepatomegaly is visible (A) with poor development of portal vein collaterals (B).

Fig. 2 Intraoperative photographs. (A, B) Right-left hemiliver splitting along the usual plane of extended left hepatectomy or right hepatectomy was performed under hepatic inflow occlusion. (C) The left liver along with the caudate lobe was removed with temporary closure of the left-middle hepatic vein trunk. (D) The three hepatic vein stumps in the recipient inferior vena cava were widely open, and the left-sided edge was reinforced with an autologous saphenous vein patch.
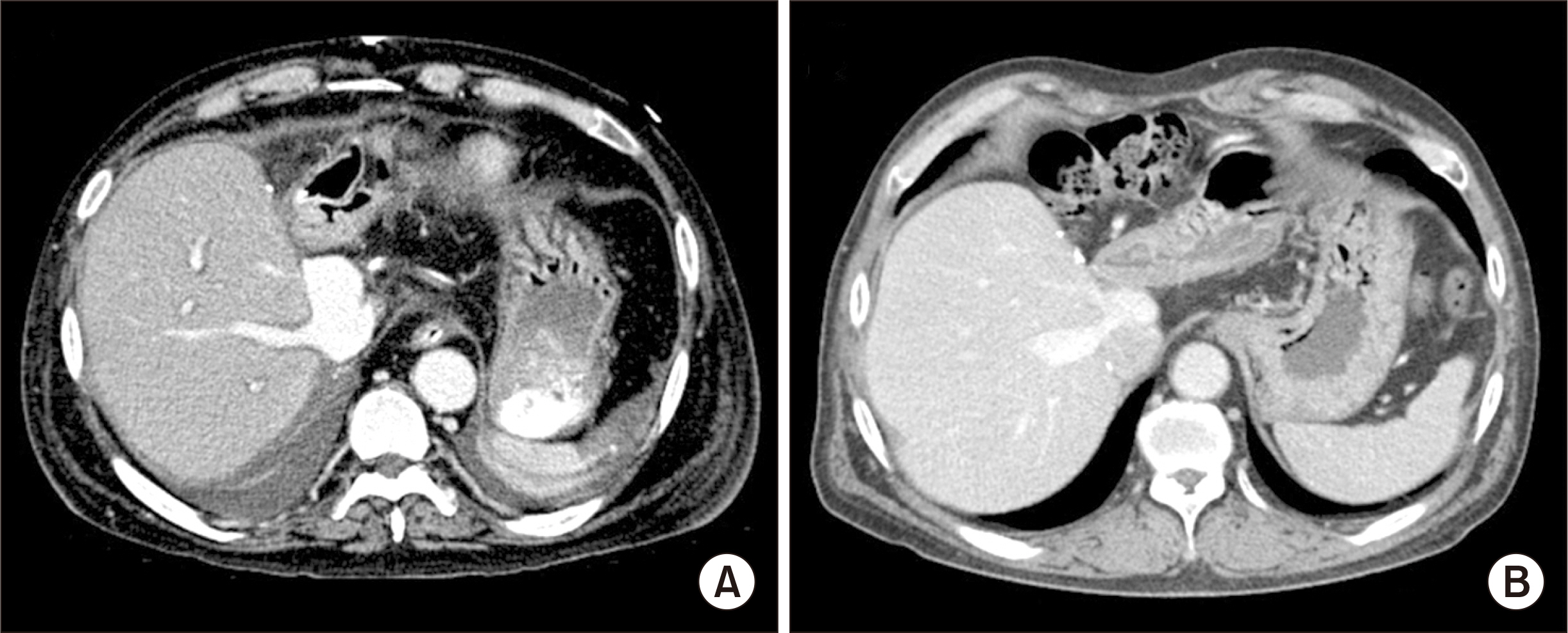
Fig. 3 Posttransplant dynamic computed tomography (CT) findings. (A) CT scan taken 2 weeks after transplantation shows no abnormal findings with bulged portion of the graft hepatic vein reconstruction. (B) CT scan taken 10 years after transplantation also shows no abnormal findings.
Reference
-
1. Hwang S, Moon DB, Lee SG. 2010; Liver transplantation and conventional surgery for advanced hepatocellular carcinoma. Transpl Int. 23:723–7. DOI: 10.1111/j.1432-2277.2010.01103.x. PMID: 20477996.
Article2. Jabir MA, Hamza HM, Fakhry H, Amira G, Hatano E, Uemoto S. 2017; Anterior versus conventional approach for resection of large right lobe hepatocellular carcinoma. J Gastrointest Cancer. 48:25–30. DOI: 10.1007/s12029-016-9865-x. PMID: 27506210.
Article3. Choi JU, Hwang S, Chung IJ, Kang SH, Ahn CS, Moon DB, et al. 2020; Prolonged hepatic inflow occlusion to reduce bleeding during recipient hepatectomy in living donor liver transplantation. Korean J Transplant. 34:55–61.4. Choi JU, Hwang S, Ahn CS, Moon DB, Ha TY, Kim KH, et al. 2019; Prolonged occlusion of the hepatoduodenal ligament to reduce risk of bleeding and tumor spread during recipient hepatectomy for living donor liver transplantation. Ann Hepatobiliary Pancreat Surg. 23:61–4. DOI: 10.14701/ahbps.2019.23.1.61. PMID: 30863809. PMCID: PMC6405371.
Article5. Lee SG, Song GW, Yoon YI. 2019; An exceptional series: 5000 living donor liver transplantations at Asan Medical Center, Seoul, Korea. Transplantation. 103:1739–41. DOI: 10.1097/TP.0000000000002708. PMID: 31461082.
Article6. Hwang S, Lee SG, Lee YJ, Sung KB, Park KM, Kim KH, et al. 2006; Lessons learned from 1,000 living donor liver transplantations in a single center: how to make living donations safe. Liver Transpl. 12:920–7. DOI: 10.1002/lt.20734. PMID: 16721780.
Article7. Pustavoitau A, Lesley M, Ariyo P, Latif A, Villamayor AJ, Frank SM, et al. 2017; Predictive modeling of massive transfusion requirements during liver transplantation and its potential to reduce utilization of blood bank resources. Anesth Analg. 124:1644–52. DOI: 10.1213/ANE.0000000000001994. PMID: 28426586.
Article8. Donohue CI, Mallett SV. 2015; Reducing transfusion requirements in liver transplantation. World J Transplant. 5:165–82. DOI: 10.5500/wjt.v5.i4.165. PMID: 26722645. PMCID: PMC4689928.
Article9. Steib A, Freys G, Lehmann C, Meyer C, Mahoudeau G. 2001; Intraoperative blood losses and transfusion requirements during adult liver transplantation remain difficult to predict. Can J Anaesth. 48:1075–9. DOI: 10.1007/BF03020372. PMID: 11744582.
Article10. Massicotte L, Beaulieu D, Roy JD, Marleau D, Vandenbroucke F, Dagenais M, et al. 2009; MELD score and blood product requirements during liver transplantation: no link. Transplantation. 87:1689–94. DOI: 10.1097/TP.0b013e3181a5e5f1. PMID: 19502961.
Article11. Pinto MA, Chedid MF, Sekine L, Schmidt AP, Capra RP, Prediger C, et al. 2019; Intraoperative cell salvage with autologous transfusion in liver transplantation. World J Gastrointest Surg. 11:11–8. DOI: 10.4240/wjgs.v11.i1.11. PMID: 30705735. PMCID: PMC6354069.
Article12. Park YK, Kim BW, Wang HJ, Xu W. 2012; Usefulness of the Pinch-Burn-Cut (PBC) technique for recipient hepatectomy in liver transplantation. Korean J Hepatobiliary Pancreat Surg. 16:13–6. DOI: 10.14701/kjhbps.2012.16.1.13. PMID: 26388900. PMCID: PMC4575015.
Article13. Lee KW, Joh JW, Kim SJ, Choi SH, Heo JS, Lee HH, et al. 2004; High hilar dissection: new technique to reduce biliary complication in living donor liver transplantation. Liver Transpl. 10:1158–62. DOI: 10.1002/lt.20230. PMID: 15350008.
Article14. Verran DJ, Gurkan A, Chui AK, Dilworth P, Koorey D, McCaughan G, et al. 2000; Pancreatitis in adult orthotopic liver allograft recipients: risk factors and outcome. Liver Transpl. 6:362–6. DOI: 10.1053/lv.2000.5203. PMID: 10827240.
Article15. Smyrniotis VE, Kostopanagiotou GG, Gamaletsos EL, Vassiliou JG, Voros DC, Fotopoulos AC, et al. 2002; Total versus selective hepatic vascular exclusion in major liver resections. Am J Surg. 183:173–8. DOI: 10.1016/S0002-9610(01)00864-9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Minimal-incision donor right hepatectomy for living donor liver transplantation
- Diaphragmatic herniation following donor hepatectomy for living donor liver transplantation: a serious complication not given due recognition
- Split liver transplantation for two adult recipients: A collective review of Korean experience
- Technical refinement of the anterior sectional drainage in right liver transplantation: a single center experience
- Decreasing the operation time of living donor liver transplantation in the era of laparoscopic living donor hepatectomy
