J Korean Foot Ankle Soc.
2020 Mar;24(1):31-36. 10.14193/jkfas.2020.24.1.31.
Effect of Leg Elevation Height on Reduced Swelling of Patients of Postoperative Acute Ankle Fractures
- Affiliations
-
- 1Departments of Orthopedic Surgery, Gangneung Asan Hospital, Korea
- 2Departments of Nursing, Gangneung Asan Hospital, Korea
- 3Department of Preventive Medicine & Public Health, Catholic Kwandong University College of Medicine, Gangneung, Korea
- KMID: 2502906
- DOI: http://doi.org/10.14193/jkfas.2020.24.1.31
Abstract
- Purpose
Leg elevation is known as an effective method for reducing leg swelling, and it has been routinely used in medical practice. However, the effect of swelling reduction in relation to the degree of elevation height is not known. This study evaluated the swelling of the leg after acute ankle fracture operations at two different elevation heights and the elevated leg heights were compared.
Materials and Methods
A total of 66 patients with postoperative acute ankle fractures were classified into two groups depending on the presence of different leg elevation heights: high-elevated (HE, case) and low-elevated groups (LE, control). We checked leg swelling, pain, subjective satisfaction for the elevation device, and the American Orthopedic Foot and Ankle Society (AOFAS) score, and we retrospectively compared them between both the groups.
Results
Leg swelling and pain were reduced in both groups. However, they did not show any significant differences between both the groups (p>0.05). Nineteen patients in the HE group replied with uncomfortable, while no patients in LE group did so. The AOFAS score at 1 year postoperatively did not show any significant differences between both the groups (p=0.46).
Conclusion
High elevation of the leg after ankle fractures did not show a significant difference from low elevation in regard to leg swelling, pain, and function. Furthermore, high leg elevation resulted in discomfort during the postoperative period. Thus, low elevation with a pillow is enough for acute ankle fracture patients with little discomfort and satisfactory swelling reduction.
Keyword
Figure
-
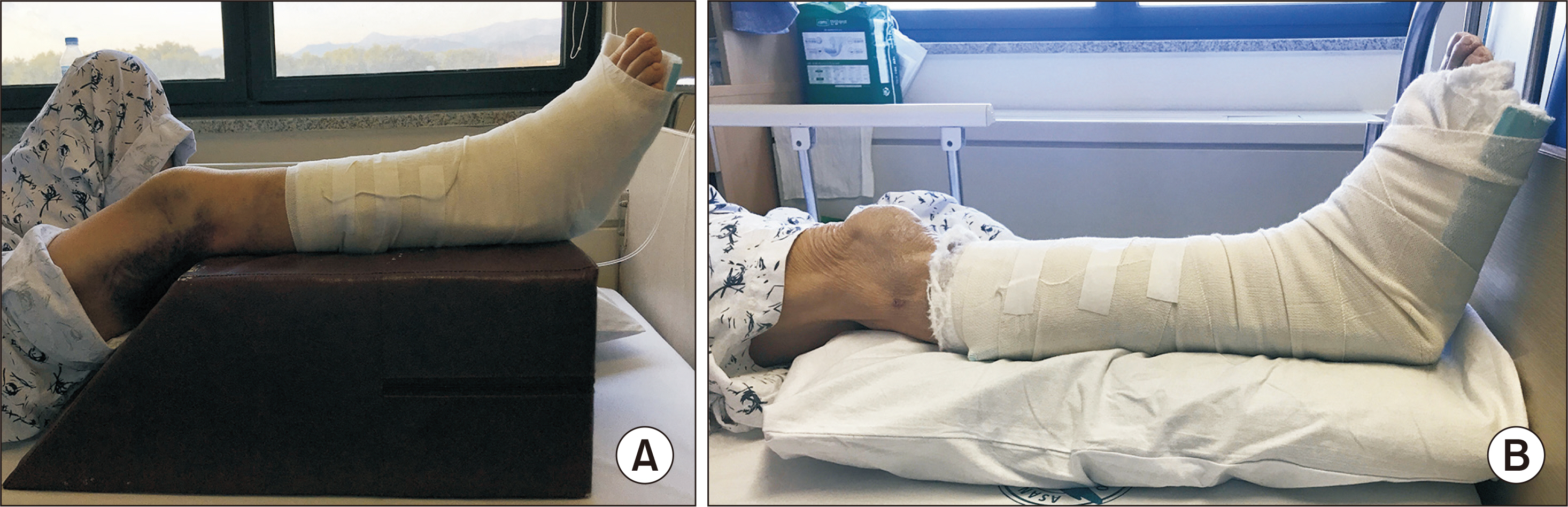
Figure 1. (A) Elevated leg with cushion elevator (30 cm-height) and (B) pillow elevator (10 cm-height) on the bed.
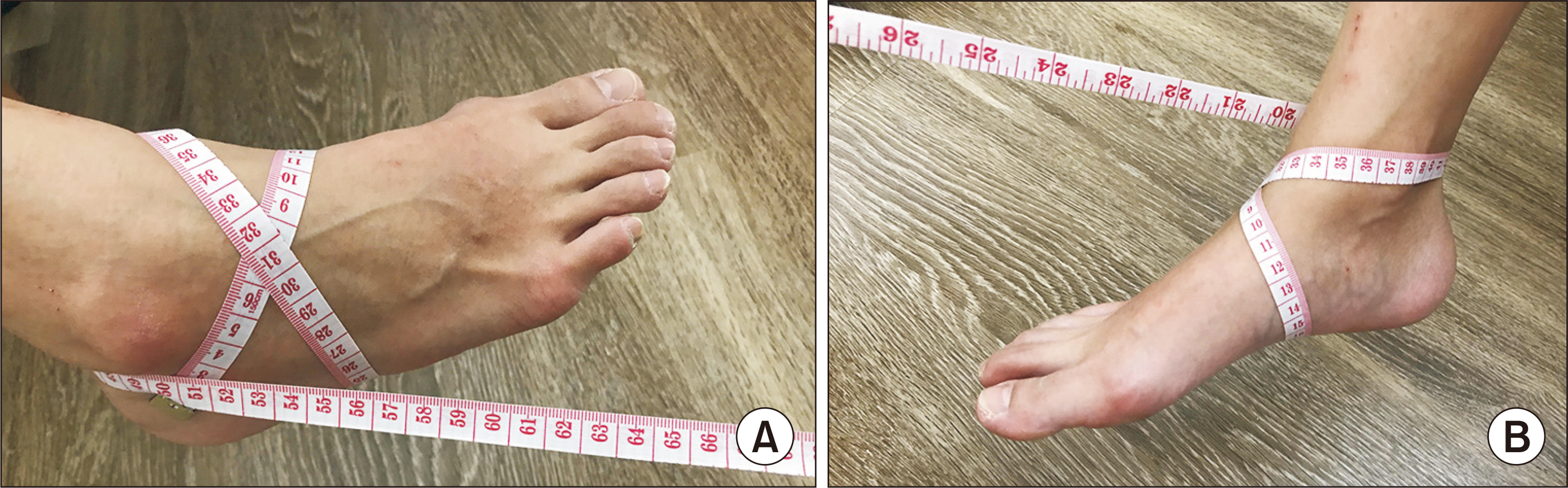
Figure 2. Figure-of-eight method. Flexible tape runs through from the tip of lateral malleolus, tuberosity of navicular, base of fifth metatarsal bone, tip of medial malleolus, and then returns to tip of lateral malleolus. (A) Medial side; (B) lateral side.
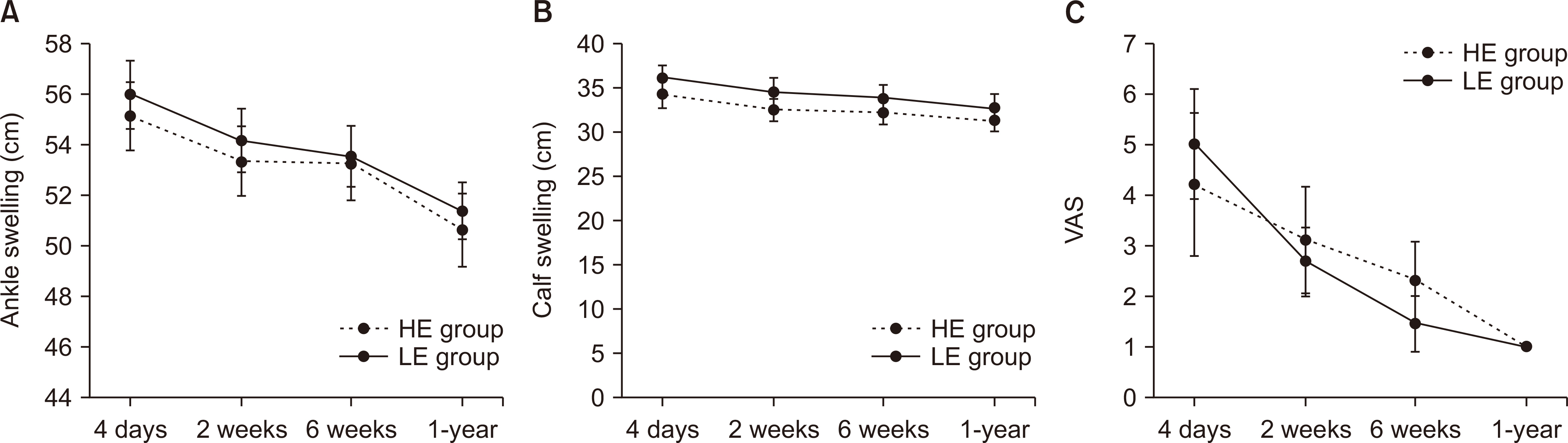
Figure 3. Change of swelling in the ankle (A), calf (B), and visual analogue scale (VAS) (C) in both groups. All parameters were checked four times at 4-day, 2-week, 6-week, and one-year postoperatively. HE: high-elevated, LE: low-elevated.
Reference
-
References
1. Elsoe R, Ostgaard SE, Larsen P. Population-based epidemiology of 9767 ankle fractures. Foot Ankle Surg. 2018; 24:34–9. doi:. DOI: 10.1016/j.fas.2016.11.002.
Article2. Tsang KK, Hertel J, Denegar CR. Volume decreases after elevation and intermittent compression of postacute ankle sprains are negated by gravity-dependent positioning. J Athl Train. 2003; 38:320–4.3. Rucinkski TJ, Hooker DN, Prentice WE, Shields EW, Cote-Murray DJ. The effects of intermittent compression on edema in postacute ankle sprains. J Orthop Sports Phys Ther. 1991; 14:65–9. doi:. DOI: 10.2519/jospt.1991.14.2.65.4. Dehghan N, McKee MD, Jenkinson RJ, Schemitsch EH, Stas V, Nauth A, et al. Early weightbearing and range of motion versus non-weightbearing and immobilization after open reduction and internal fixation of unstable ankle fractures: a randomized controlled trial. J Orthop Trauma. 2016; 30:345–52.
Article5. Jansen H, Jordan M, Frey S, Hölscher-Doht S, Meffert R, Heintel T. Active controlled motion in early rehabilitation improves outcome after ankle fractures: a randomized controlled trial. Clin Rehabil. 2018; 32:312–8. doi:. DOI: 10.1177/0269215517724192.
Article6. Esterson PS. Measurement of ankle joint swelling using a figure of 8∗. J Orthop Sports Phys Ther. 1979; 1:51–2. doi:. DOI: 10.2519/jospt.1979.1.1.51.
Article7. Donner A, Donald A. Analysis of data arising from a stratified design with the cluster as unit of randomization. Stat Med. 1987; 6:43–52. doi:. DOI: 10.1002/sim.4780060106.
Article8. Petersen EJ, Irish SM, Lyons CL, Miklaski SF, Bryan JM, Henderson NE, et al. Reliability of water volumetry and the figure of eight method on subjects with ankle joint swelling. J Orthop Sports Phys Ther. 1999; 29:609–15. doi:. DOI: 10.2519/jospt.1999.29.10.609.
Article9. Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979; 86:420–8. doi:. DOI: 10.1037//0033-2909.86.2.420.
Article10. Sims D. Effects of positioning on ankle edema. J Orthop Sports Phys Ther. 1986; 8:30–3. doi:. DOI: 10.2519/jospt.1986.8.1.30.
Article11. Cloughley WB, Mawdsley RH. Effect of running on volume of the foot and ankle. J Orthop Sports Phys Ther. 1995; 22:151–4. doi:. DOI: 10.2519/jospt.1995.22.4.151.
Article12. McCulloch J, Boyd VB. The effects of whirlpool and the dependent position on lower extremity volume. J Orthop Sports Phys Ther. 1992; 16:169–73. doi:. DOI: 10.2519/jospt.1992.16.4.169.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- May-Thurner Syndrome Appearing as Recurrent Swelling and Cellulitis in the Left Leg and Foot
- A Clinical Observation on 30 Cases of Ankle Fractures
- Role of Arthroscopy in Ankle Fracture Surgeries
- Conservative Management of Ankle Sprains
- Meshed Stab Incision for Severe Swelling after Foot and Ankle Injury: A Technical Report
