Successful percutaneous coronary intervention with extracorporeal membrane oxygenation support after right coronary artery dissection in an eisenmenger syndrome patient
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Seoul Paik Hospital, Inje University College of Medicine, Seoul, Korea
- KMID: 2500951
- DOI: http://doi.org/10.4266/acc.2017.00024
Abstract
- The presentation of coronary artery disease in a patient with Eisenmenger syndrome (ES) is relatively rare. Cardiogenic shock due to coronary artery dissection during percutaneous coronary intervention (PCI) can be more critical in these patients. Here, we report a case of successful PCI under mechanical circulation support in a patient with ES who experienced potentially fatal right coronary artery dissection. This case emphasizes that use of extracorporeal membrane oxygenation (ECMO) can lead to successful management of critical complication during PCI, and that the immediate decision to apply of ECMO is important in ES patients who face impending cardiogenic shock with acute heart failure.
Keyword
Figure
-
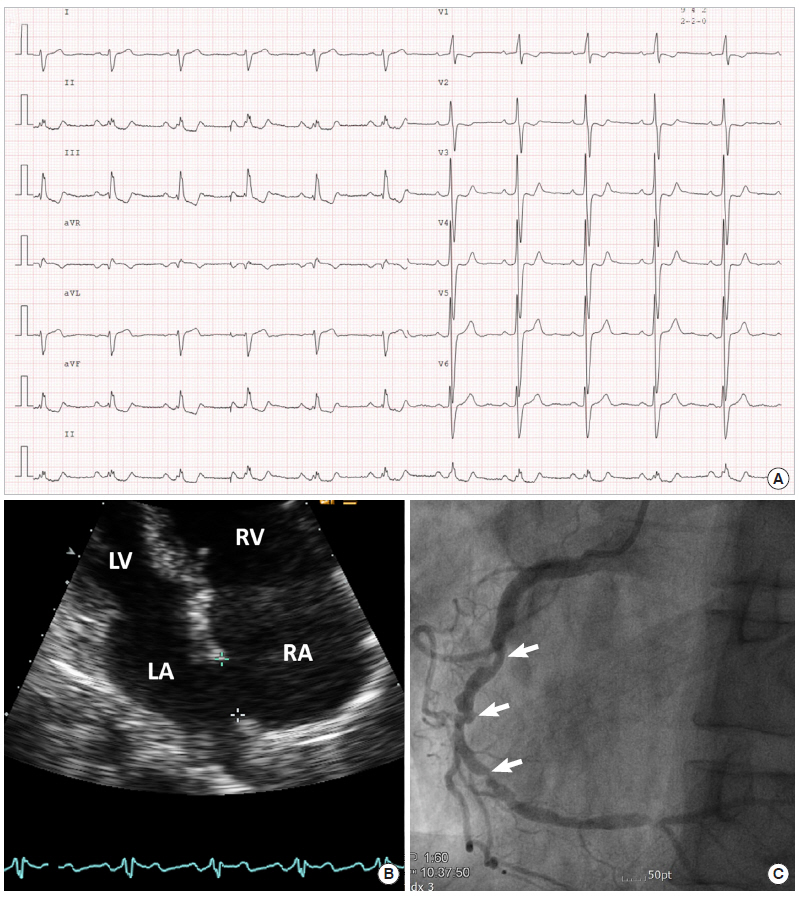
Figure 1. Baseline examination. (A) Electrocardiography showing sinus rhythm and right ventricular hypertrophy. (B) Echocardiography. Apical four chamber view showing right atrial and ventricular dilatation and atrial septal defect. (C) Coronary angiography. Angiographic image showing significant luminal narrowing in the mid to distal right coronary artery. LV: left ventricle; RV: right ventricle; LA: left atrium; RA: right atrium.

Figure 2. Angiography after guiding catheter engagement. (A) The cine showing angiographic haziness at the proximal right coronary artery and contrast stain suggesting dissection at the ostium (arrow). (B) Collapsed and invisible coronary vessel lumen due to dissection.
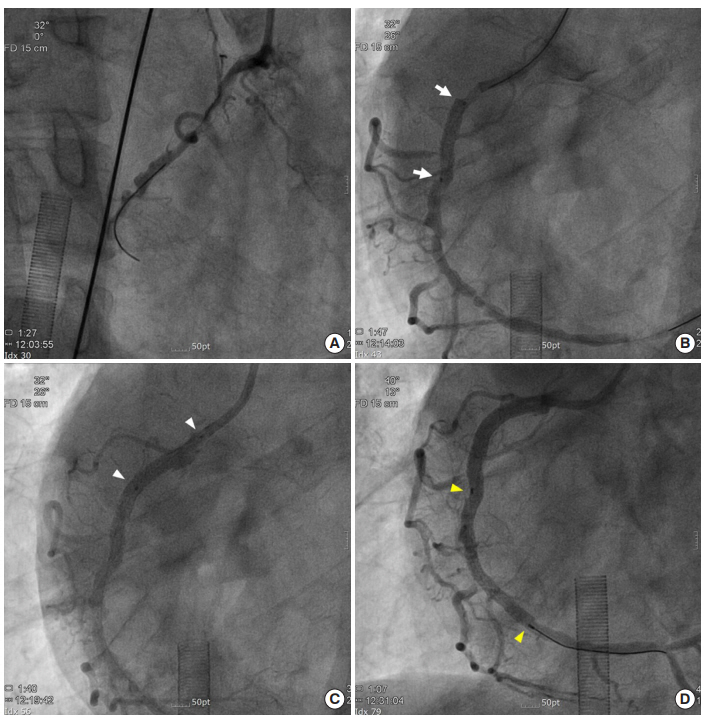
Figure 3. Direct percutaneous coronary intervention under extracorporeal membrane oxygenation support. (A) Successful wiring through the true lumen. (B) Direct stenting at the proximal to mid right coronary artery (RCA) to cover the dissection (white arrows, Onyx 3.5×18 mm). (C) Direct stenting at the RCA ostium (white arrowheads, Onyx 3.5×18 mm). (D) Direct stent deployment at the mid to distal RCA (yellow arrowheads, Onyx 3.0×38 mm).
Reference
-
References
1. Perloff JK. The coronary circulation in cyanotic congenital heart disease. Int J Cardiol. 2004; 97 Suppl 1:79–86.
Article2. Lill MC, Perloff JK, Child JS. Pathogenesis of thrombocytopenia in cyanotic congenital heart disease. Am J Cardiol. 2006; 98:254–8.
Article3. Hjortshøj CM, Kempny A, Jensen AS, Sørensen K, Nagy E, Dellborg M, et al. Past and current cause-specific mortality in Eisenmenger syndrome. Eur Heart J. 2017; 38:2060–7.
Article4. Oechslin E, Kiowski W, Schindler R, Bernheim A, Julius B, Brunner-La Rocca HP. Systemic endothelial dysfunction in adults with cyanotic congenital heart disease. Circulation. 2005; 112:1106–12.
Article5. Platzmann AM, Schmiady M, Rudiger A, Huebler M, Greutmann M, Bettex DA. First description of successful weaning from ECMO in a patient with Eisenmenger syndrome after repair of pulmonary artery dissection. Int J Cardiol. 2015; 187:144–5.
Article6. Belohlavek J, Rohn V, Jansa P, Tosovsky J, Kunstyr J, Semrad M, et al. Veno-arterial ECMO in severe acute right ventricular failure with pulmonary obstructive hemodynamic pattern. J Invasive Cardiol. 2010; 22:365–9.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Preoperative Extracorporeal Membrane Oxygenation for Severe Ischemic Mitral Regurgitation: 2 case reports
- Recent Advances in Percutaneous Coronary Intervention in Coronary Artery Disease
- Spontaneous coronary artery dissection by intravascular ultrasound in a patient with myocardial infarction
- Spontaneous Coronary Artery Dissection in a female patient with fragile X syndrome
- Treatment of Stent Dislodgement Complicated by Coronary Artery Dissection using Parallel Wire Technique and Small Balloon
