Treatment of Stent Dislodgement Complicated by Coronary Artery Dissection using Parallel Wire Technique and Small Balloon
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Dong-A University, Busan, Korea. thinkmed@dau.ac.kr
- KMID: 2308512
- DOI: http://doi.org/10.7180/kmj.2013.28.1.55
Abstract
- Stent dislodgement is a rare complication of complex percutaneous coronary artery intervention and is often associated with significant morbidity. We report a case of stent dislodgement complicated by coronary artery dissection and acute total occlusion of left circumflex coronary artery. Direct expansion of the dislodged stent was performed using parallel wire technique and small balloon. An overlapping stent was implanted for remained coronary artery dissection. Coronary artery flow was restored and ST segment elevation was normalized after successful intervention.
Keyword
MeSH Terms
Figure
-
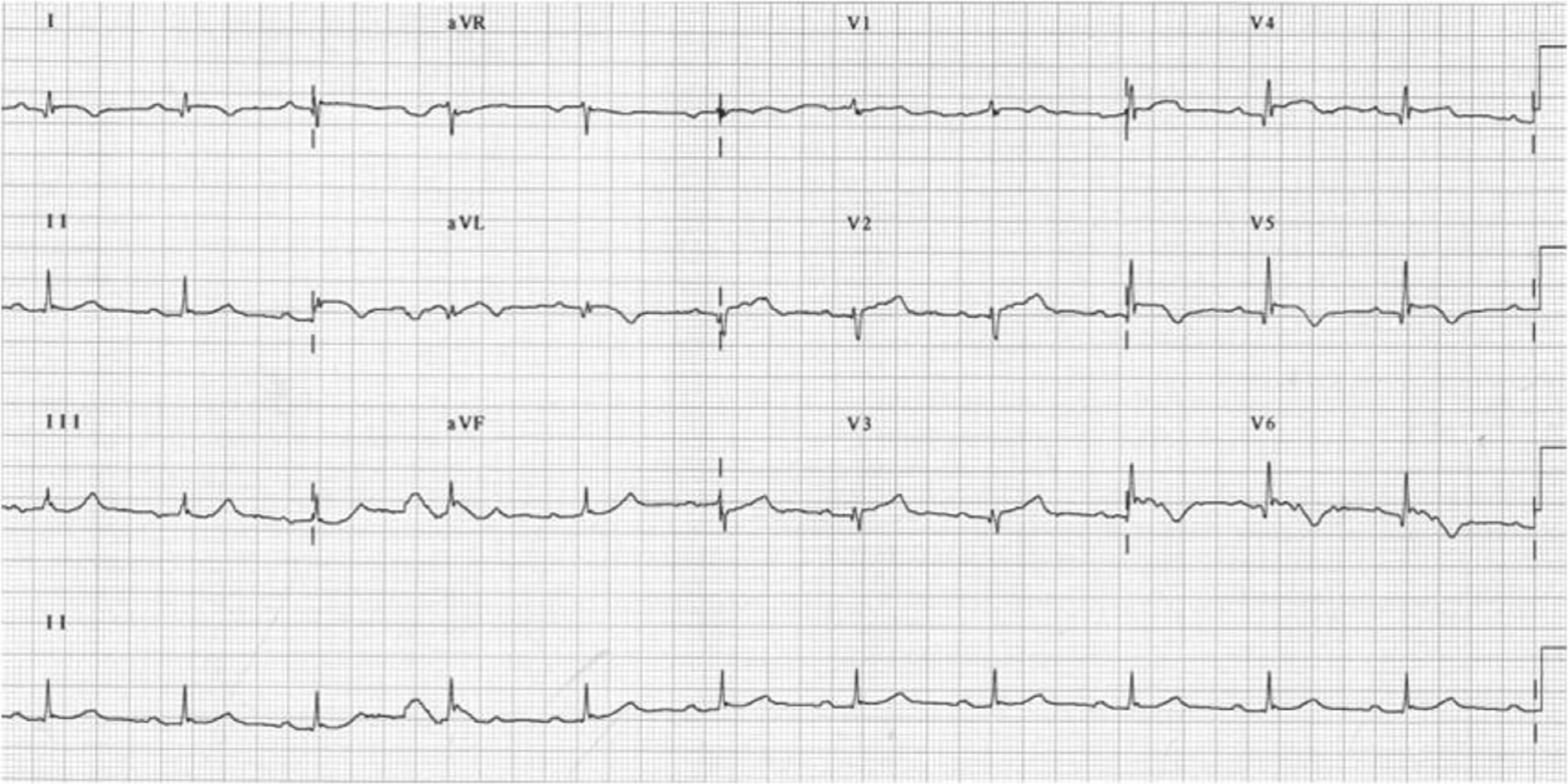
Fig. 1. Electrocardiogram after coronary artery dissection and acute total occlusion of left circumflex coronary artery showed ST segment elevation and T wave inversion in V4-V6, I, and aVL leads.
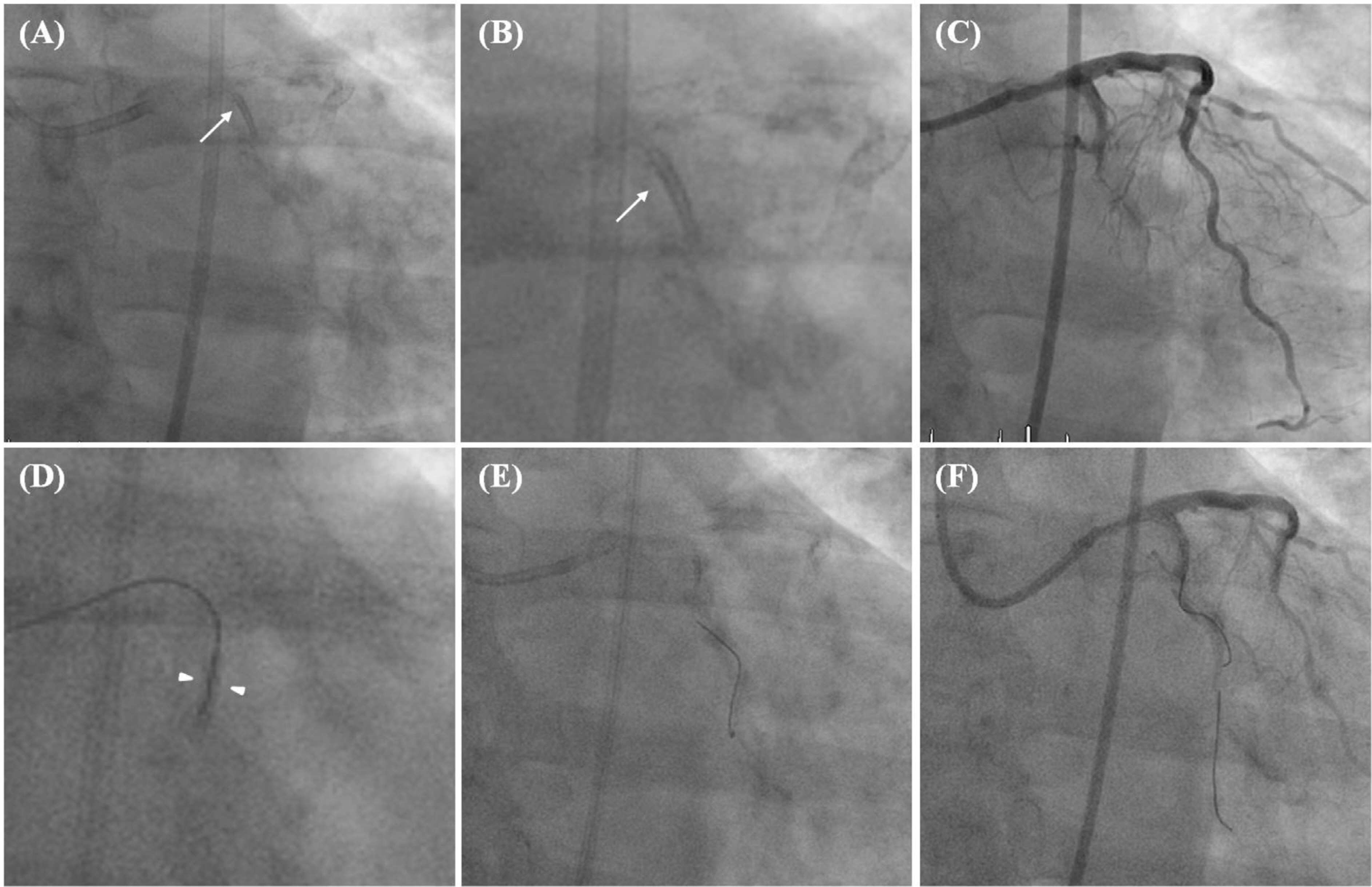
Fig. 2. (A) Dislodged stent (arrow) was remained in proximal LCX. (B) Magnified view of the dislodged stent of 2.75 X 24 mm in size (arrow). (C) Coronary angiography showed coronary artery dissection and total occlusion of proximal LCX. (D) Magnified view of the dislodged stent. A floppy tipped guide wire was inserted to the lumen of dislodged stent (within arrowheads). (E) However, the guide wire entered to the false lumen of distal LCX formed by dissecting intimal flap. (F) Another guide wire was inserted and two guide wires were advanced alternately by parallel wire technique. Finally, a guide wire found the true lumen of distal LCX. LCX: left circumflex coronary artery.
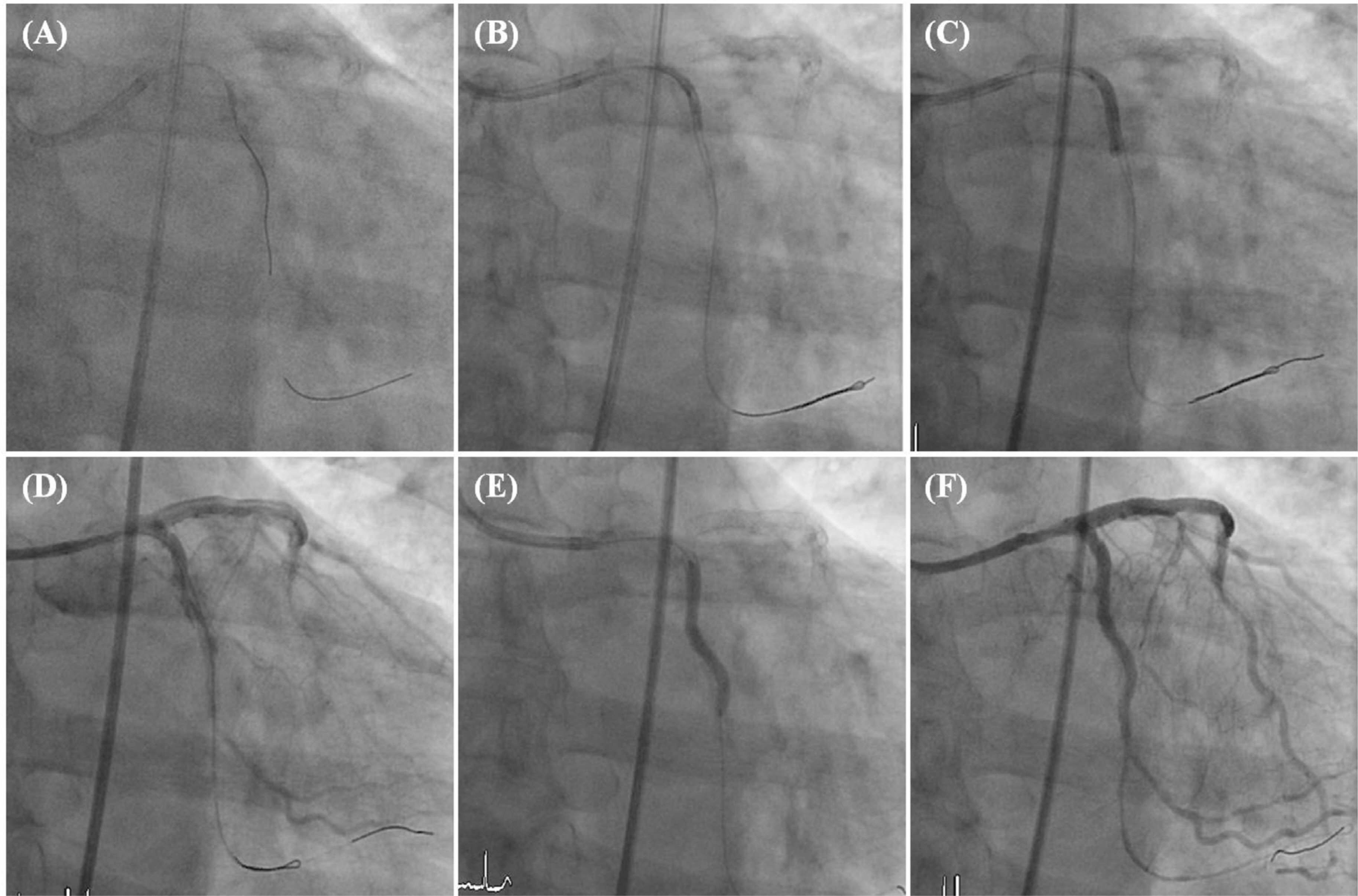
Fig. 3. (A) A guide wire in false lumen was reinserted to the true lumen (B) A small balloon was positioned within the dislodged stent and inflated. (C) Partially expanded dislodged stent was fully expanded by a balloon with larger diameter. (D) Coronary angiography after direct expansion of the dislodged stent showed partial restoration of distal LCX flow. (E) A overlapping stent of 2.5 X 32 mm in size was implanted to cover coronary artery dissection. (F) Distal LCX flow was fully recovered after coronary artery intervention. LCX: left circumflex coronary artery.
Reference
-
1.Bolte J., Neumann U., Pfafferott C., Vogt A., Engel HJ., Mehmel HC, et al. Incidence, management, and outcome of stent loss during intracoronary stenting. Am J Cardiol. 2001. 88:565–7.
Article2.Brilakis ES., Best PJ., Elesber AA., Barsness GW., Lennon RJ., Holmes DR Jr, et al. Incidence, retrieval methods, and outcomes of stent loss during percutaneous coronary intervention: a large single-center experience. Catheter Cardiovasc Interv. 2005. 66:333–40.
Article3.Lohavanichbutr K., Webb JG., Carere RG., Solankhi N., Jarochowski M., D'Yachkova Y, et al. Mechanisms, management, and outcome of failure of delivery of coronary stents. Am J Cardiol. 1999. 83:779–81. A9.
Article4.Eggebrecht H., Haude M., von Birgelen C., Oldenburg O., Baumgart D., Herrmann J, et al. Nonsurgical retrieval of embolized coronary stents. Catheter Cardiovasc Interv. 2000. 51:432–40.
Article5.Shim BJ., Lee JM., Lee SJ., Kim SS., Lee DH., Shin WS, et al. Three cases of non-surgical treatment of stent loss during percutaneous coronary intervention. Korean Circ J. 2010. 40:530–5.
Article6.Lee HY., Kim BH., Yoo WS., Yun SU., Kang MH., Kang TS, et al. Successful removal of a dislodged stent using a gooseneck snare. Korean J Med. 2008. 75:S843–7.7.Hussain F. The parallel wire technique to deal with wire-induced dissection of a complex calcified lesion. J Invasive Cardiol. 2007. 19:E60–2.8.Uyan C., Gündüz H., Arinc H., Akdemir R. Embolised stent into the circumflex coronary artery during percutaneous coronary intervention. Int Heart J. 2006. 47:125–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two dislodged and crushed coronary stents: treatment of two simultaneously dislodged stents using crushing techniques
- Successful coronary stent retrieval from the ascending aorta using a gooseneck snare kit
- Aspiration Thromboembolectomy in the Management of Acute Coronary Occlusion during Pertaneous Transluminal Coronary Angioplasty
- Retrieval of a dislodged and dismounted coronary stent; using a rendezvous and snare technique at the brachial artery level via femoral approach
- Recanalization of an Accidentally Crushed Coronary Stent by Intravascular Ultrasonography Catheter Entrapment
