Doppler US and CT Diagnosis of Nutcracker Syndrome
- Affiliations
-
- 1Department of Radiology, Seoul National University Hospital, Seoul, Korea. kimshrad@snu.ac.kr
- 2Kidney Research Institute, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2471675
- DOI: http://doi.org/10.3348/kjr.2019.0084
Abstract
- Nutcracker syndrome (NCS) is a syndrome caused by compression of the left renal vein (LRV), between the abdominal aorta and the superior mesenteric artery, resulting in hypertension of the LRV and hematuria. Doppler ultrasonography (US) has been commonly used for the diagnosis of NCS. However, several technical issues, such as Doppler angle and sample volume, need to be considered to obtain satisfactory results. In addition, morphologic changes of the LRV and a jetting phenomenon across the aortomesenteric portion of the LRV on contrast-enhanced computed tomography (CECT) are diagnostic clues of NCS. With proper Doppler US and CECT, NCS can be diagnosed noninvasively.
Keyword
MeSH Terms
Figure
-
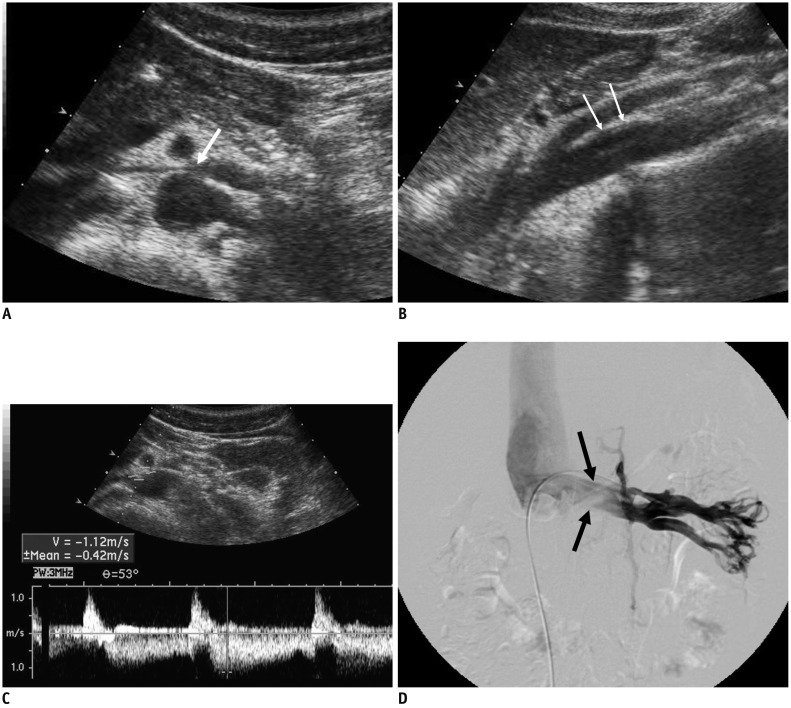
Fig. 1 18-year-old male patient with NCS.A. Transverse US of LRV shows compression of LRV at AM portion (arrow). B. Sagittal US of aorta and SMA shows slit-like LRV (arrows), compressed between two vessels. C. Spectral Doppler US of LRV at AM portion shows clear venous flow spectrum, with PV of 112 cm/s. D. Left renal venogram shows compression of LRV at AM portion (arrows). Pressure gradient measured across AM portion of LRV was 4 mm Hg. AM = aortomesenteric, LRV = left renal vein, NCS = nutcracker syndrome, PV = peak velocity, SMA = superior mesenteric artery, US = ultrasonography
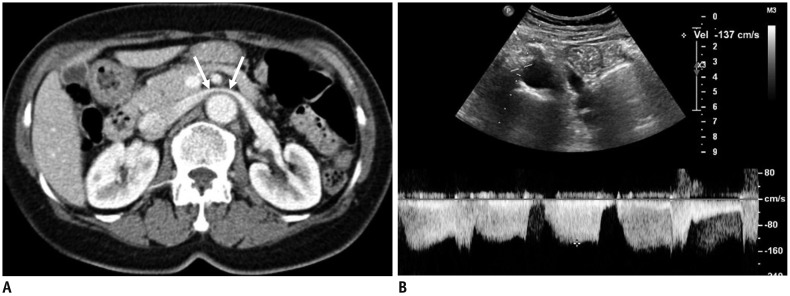
Fig. 2 72-year-old female patient with NCS.A. CECT scan shows LRV (arrows) stretched over aorta, without any compression between aorta and SMA. B. Spectral Doppler US of LRV measured at AM portion shows PV of 137 cm/s. CECT = contrast-enhanced CT

Fig. 3 49-year-old female patient with posterior NCS.CECT images in early cortical phase show retroarotic LRV (arrows) (A) compression between abdominal aorta and vertebra. Jetting phenomenon of contrast-opacified venous flow (arrowheads) (B) into IVC can be seen. C. Spectral Doppler US of retroaortic LRV shows high PV of 94.8 cm/s. IVC = inferior vena cava
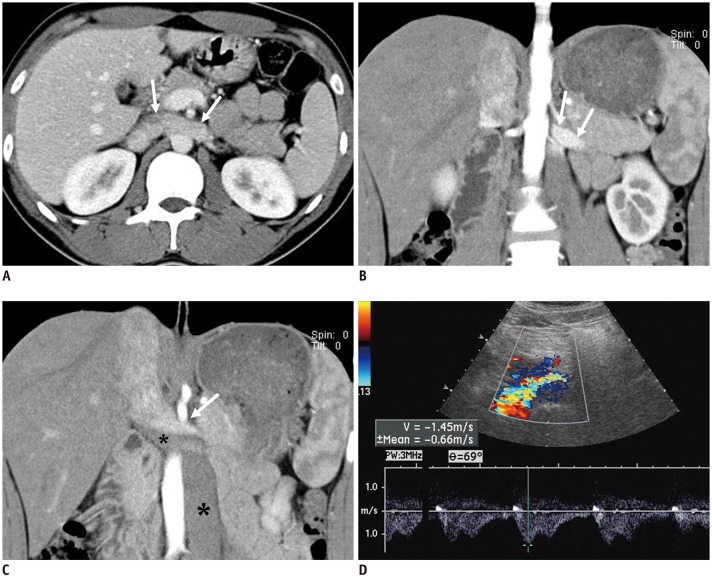
Fig. 4 NCS in 20-year-old male patient with left-sided IVC.A. CECT image shows well-preserved lumen in LRV (arrows), without any compression between aorta and SMA. B, C. Coronal CECT images show left-sided IVC crossing midline and continuous with right-sided suprarenal IVC. Note contrast-opacified venous flow from LRV (arrows), which is compressed by non-opacified venous flow from lower part of body thought left-sided IVC (asterisks). D. Spectral Doppler US performed at midline-crossing of vessel reveals high PV of 145 cm/s. In this patient, LRV is not compressed anatomically, but venous flow from left kidney is hemodynamically impeded by dominant venous flow from lower extremity through left-sided IVC.
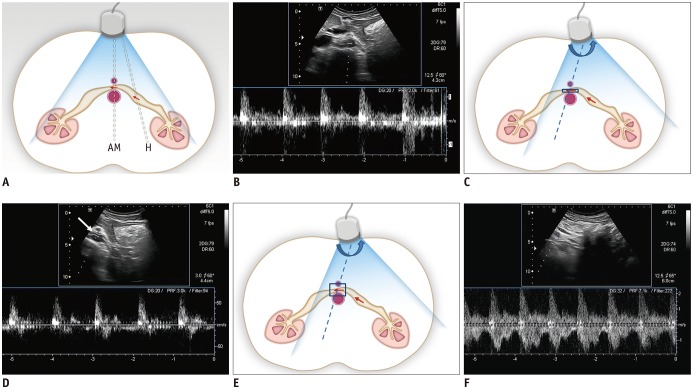
Fig. 5 Schematic drawing of Doppler US of LRV and spectral Doppler US images of LRV.A. With usual position of US transducer in transverse plane, Doppler angle is optimal to obtain clear spectrum for hilar portion of LRV (H), while angle for AM portion of LRV is around 90°. Arrows indicate direction of blood flow and dotted lines indicate direction of ultrasound beam. B. Spectral Doppler US image of LRV obtained at AM portion shows noisy spectrum from aorta. Therefore, it is almost impossible to measure flow velocity in LRV. C. With slight shift of transducer to left and subtle counterclockwise rotation (curved arrow) until AM portion of LRV is located in left corner of US image, Doppler angle for AM portion of LRV can be adjusted. Arrows indicate direction of blood flow and dotted line indicates direction of ultrasound beam. D. Even with adjustment of Doppler angle, Doppler spectrum from LRV is still not clear, because LRV is not properly located due to small sample volume (arrow). E. In addition to adjustment of Doppler angle, increasing sample volume may help LRV be continuously included within sample volume between pulsating aorta and SMA. Arrows indicate direction of blood flow and dotted line indicates direction of ultrasound beam. F. Doppler spectrum from LRV now becomes optimal, with PV of approximately 150 cm/s.
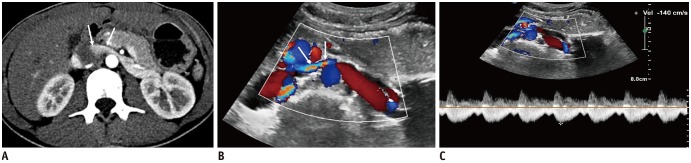
Fig. 6 17-year-old woman with NCS.A. CECT scan shows compression of LRV between aorta and SMA. Note contrast-opacified venous flow along anterior non-dependent portion of IVC (arrows). B. Color Doppler US of LRV shows bright color flow signal (arrows) at AM portion of LRV due to aliasing artifacts caused by high flow velocity. C. Spectral Doppler US at AM portion of LRV shows PV of 140 cm/s.
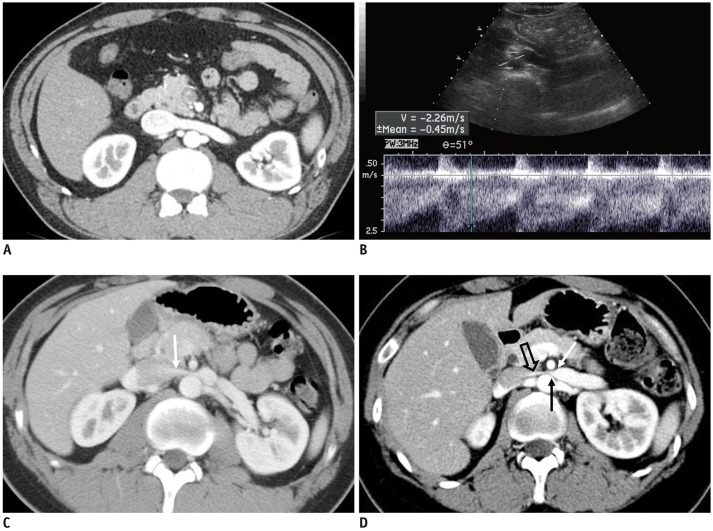
Fig. 7 CECT of kidney in early cortical phase.A. 45-year-old male without hematuria. CECT shows normal LRV without compression at AM portion and homogeneously opacified LRV and IVC. B, C. 17-year-old male with NCS. B. Doppler US of LRV at AM portion shows high PV (226 cm/s) of LRV. C. CECT in early cortical phase shows jetting of contrast-opacified venous flow (arrow) into IVC across AM portion of LRV. D. 28-year-old female with NCS. CECT shows severely compressed LRV at AM portion, with beak sign (arrows). Note jetting (open arrow) of contrast-opacified venous flow into IVC across AM portion of LRV.
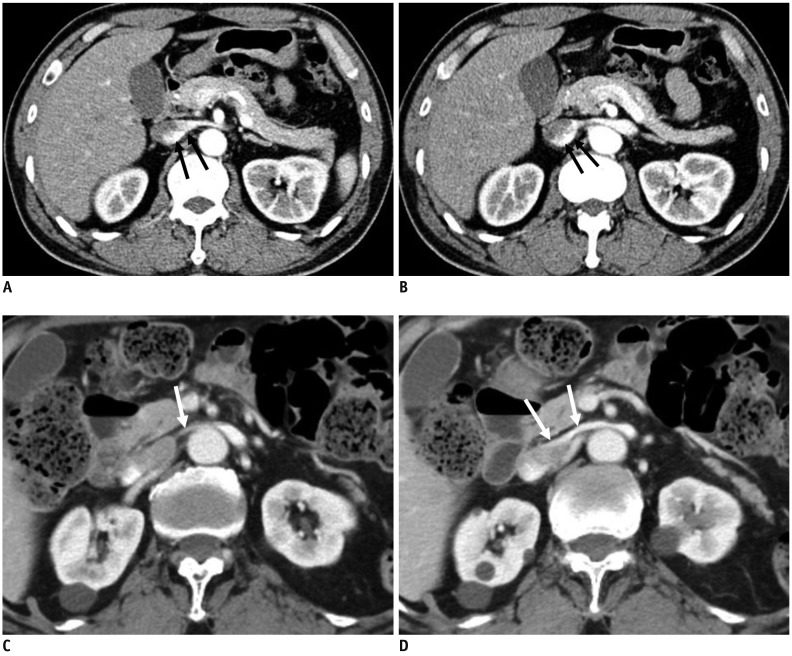
Fig. 8 Preferential flow of contrast-opacified venous flow on CECT.A, B. 48-year-old male without hematuria. CECT images in early cortical phase show contrast-opacified venous flow into IVC along dependent posterior aspect of LRV and IVC (arrows). C, D. 82-year-old male with microscopic hematuria. CECT images in early cortical phase show contrast-opacified venous flow into IVC along non-dependent anterior aspect of LRV and IVC (arrows). PV of LRV at AM portion measured by Doppler US was 133 cm/s (not shown).
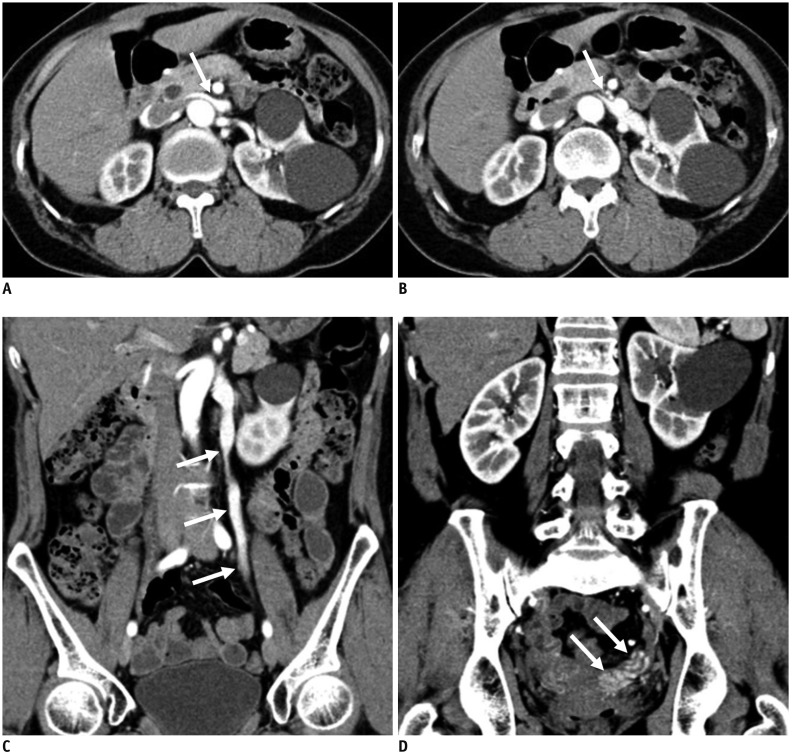
Fig. 9 59-year-old female with concurrent NCS and pelvic congestion syndrome.Patient complained of persistent microscopic hematuria and chronic pelvic pain.A, B. CECT images show compression of LRV at AM portion (arrows). C, D. CECT images in coronal plane show regurgitation of contrast-opacified LRV flow into left gonadal vein and pelvic veins (arrows).
Cited by 2 articles
-
Nutcracker syndrome in children: review of symptom, diagnosis, and treatment
Diana S. Kalantar, Se Jin Park, Jae Il Shin
Child Kidney Dis. 2023;27(2):89-96. doi: 10.3339/ckd.23.018.Effect of renal Doppler ultrasound on the detection of nutcracker syndrome in children presenting orthostatic proteinuria
Eun Jae Hwang, Ji Hong Kim, Mi-Jung Lee, Haesung Yoon, Jae Il Shin, Keum Hwa Lee
Child Kidney Dis. 2024;28(2):74-79. doi: 10.3339/ckd.24.009.
Reference
-
1. El-Sadr AR, Mina E. Anatomical and surgical aspects in the operative management of varicocele. Urol Cutaneous Rev. 1950; 54:257–262. PMID: 15443180.2. Chait A, Matasar KW, Fabian CE, Mellins HZ. Vascular impressions on the ureters. Am J Roentgenol Radium Ther Nucl Med. 1971; 111:729–749.
Article3. de Schepper A. [“Nutcracker” phenomenon of the renal vein and venous pathology of the left kidney]. J Belge Radiol. 1972; 55:507–511. PMID: 4660828.4. Welsch T, Büchler MW, Kienle P. Recalling superior mesenteric artery syndrome. Dig Surg. 2007; 24:149–156. PMID: 17476104.
Article5. Ananthan K, Onida S, Davies AH. Nutcracker syndrome: an update on current diagnostic criteria and management guidelines. Eur J Vasc Endovasc Surg. 2017; 53:886–894. PMID: 28356209.
Article6. Nishimura Y, Fushiki M, Yoshida M, Nakamura K, Imai M, Ono T, et al. Left renal vein hypertension in patients with left renal bleeding of unknown origin. Radiology. 1986; 160:663–667. PMID: 3737903.
Article7. Kim SH, Cho SW, Kim HD, Chung JW, Park JH, Han MC. Nutcracker syndrome: diagnosis with Doppler US. Radiology. 1996; 198:93–97. PMID: 8539413.
Article8. Cheon JE, Kim WS, Kim IO, Kim SH, Yeon KM, Ha IS, et al. Nutcracker syndrome in children with gross haematuria: Doppler sonographic evaluation of the left renal vein. Pediatr Radiol. 2006; 36:682–686. PMID: 16770671.
Article9. Kim KW, Cho JY, Kim SH, Yoon JH, Kim DS, Chung JW, et al. Diagnostic value of computed tomographic findings of nutcracker syndrome: correlation with renal venography and renocaval pressure gradients. Eur J Radiol. 2011; 80:648–654. PMID: 20869828.
Article10. Kurklinsky AK, Rooke TW. Nutcracker phenomenon and nutcracker syndrome. Mayo Clin Proc. 2010; 85:552–559. PMID: 20511485.
Article11. Beinart C, Sniderman KW, Saddekni S, Weiner M, Vaughan ED Jr, Sos TA. Left renal vein hypertension: a cause of occult hematuria. Radiology. 1982; 145:647–650. PMID: 7146391.
Article12. Oteki T, Nagase S, Hirayama A, Sugimoto H, Hirayama K, Hattori K, et al. Nutcracker syndrome associated with severe anemia and mild proteinuria. Clin Nephrol. 2004; 62:62–65. PMID: 15267016.
Article13. Trambert JJ, Rabin AM, Weiss KL, Tein AB. Pericaliceal varices due to the nutcracker phenomenon. AJR Am J Roentgenol. 1990; 154:305–306. PMID: 2105019.
Article14. Cho BS, Choi YM, Kang HH, Park SJ, Lim JW, Yoon TY. Diagnosis of nut-cracker phenomenon using renal Doppler ultrasound in orthostatic proteinuria. Nephrol Dial Transplant. 2001; 16:1620–1625. PMID: 11477164.
Article15. Park SJ, Lim JW, Cho BS, Yoon TY, Oh JH. Nutcracker syndrome in children with orthostatic proteinuria: diagnosis on the basis of Doppler sonography. J Ultrasound Med. 2002; 21:39–45. PMID: 11794401.16. Pournasiri Z. The nutcracker syndrome as a rare cause of chronic abdominal pain: a case report. J Compr Ped. 2016; 7:e39741.
Article17. Taktak A, Hakan Demirkan T, Acar B, Gu R G, Köksoy A, Uncu N, et al. Clinico-radiological correlation of nutcracker syndrome: a single centre experience. Arch Argent Pediatr. 2017; 115:165–168. PMID: 28318183.
Article18. Liebl R. Nutcracker phenomenon or nutcracker syndrome? Nephrol Dial Transplant. 2005; 20:2009. author reply 2009. PMID: 15985517.
Article19. Buschi AJ, Harrison RB, Norman A, Brenbridge AG, Williamson BR, Gentry RR, et al. Distended left renal vein: CT/sonographic normal variant. AJR Am J Roentgenol. 1980; 135:339–342. PMID: 6773339.
Article20. Zerin JM, Hernandez RJ, Sedman AB, Kelsch RC. “Dilatation” of the left renal vein on computed tomography in children: a normal variant. Pediatr Radiol. 1991; 21:267–269. PMID: 1870922.
Article21. Sebro K, Goetz L, Persaud S. Nutcracker syndrome: a rare and potentially under diagnosed cause of haematuria. Case Rep Surg Invasive Proced. 2017; 1:4–6.22. He Y, Wu Z, Chen S, Tian L, Li D, Li M, et al. Nutcracker syndrome—How well do we know it? Urology. 2014; 83:12–17. PMID: 24139744.
Article23. Wendel RG, Crawford ED, Hehman KN. The “nutcracker” phenomenon: an unusual cause for renal varicosities with hematuria. J Urol. 1980; 123:761–763. PMID: 7420571.
Article24. Hayashi M, Kume T, Nihira H. Abnormalities of renal venous system and unexplained renal hematuria. J Urol. 1980; 124:12–16. PMID: 7411696.
Article25. Lau JLT, Lo R, Chan FL, Wong KK. The posterior “nutcracker”: hematuria secondary to retroaortic left renal vein. Urology. 1986; 28:437–439. PMID: 3787913.
Article26. Ali-El-Dein B, Osman Y, Shehab El-Din AB, El-Diasty T, Mansour O, Ghoneim MA. Anterior and posterior nutcracker syndrome: a report on 11 cases. Transplant Proc. 2003; 35:851–853. PMID: 12644163.
Article27. Skeik N, Gloviczki P, Macedo TA. Posterior nutcracker syndrome. Vasc Endovascular Surg. 2011; 45:749–755. PMID: 21890560.
Article28. Özkan MB, Ceyhan Bilgici M, Hayalioglu E. Anterior and posterior nutcracker syndrome accompanying left circumaortic renal vein in an adolescent: case report. Arch Argent Pediatr. 2016; 114:e114–e116. PMID: 27079405.29. Naito M, Terayama H, Nakamura Y, Hayashi S, Miyaki T, Itoh M. Left testicular artery arching over the ipsilateral renal vein. Asian J Androl. 2006; 8:107–110. PMID: 16372128.
Article30. Radisic MV, Feldman D, Diaz C, Froment RO. Unexplained hematuria during pregnancy: right-sided nutcracker phenomenon. Int Urol Nephrol. 2007; 39:709–711. PMID: 17031506.
Article31. Beinart C, Sniderman KW, Tamura S, Vaughan ED Jr, Sos TA. Left renal vein to inferior vena cava pressure relationship in humans. J Urol. 1982; 127:1070–1071. PMID: 7087011.
Article32. Hangge PT, Gupta N, Khurana A, Quencer KB, Albadawi H, Alzubaidi SJ, et al. Degree of left renal vein compression predicts nutcracker syndrome. J Clin Med. 2018; 7:E107. PMID: 29738433.
Article33. Fong JKK, Poh ACC, Tan AGS, Taneja R. Imaging findings and clinical features of abdominal vascular compression syndromes. AJR Am J Roentgenol. 2014; 203:29–36. PMID: 24951193.
Article34. Orczyk K, Wysiadecki G, Majos A, Stefańczyk L, Topol M, Polguj M. What each clinical anatomist has to know about left renal vein entrapment syndrome (nutcracker syndrome): a review of the most important findings. Biomed Res Int. 2017; DOI: 10.1155/2017/1746570. [Epub].
Article35. Ahmed K, Sampath R, Khan MS. Current trends in the diagnosis and management of renal nutcracker syndrome: a review. Eur J Vasc Endovasc Surg. 2006; 31:410–416. PMID: 16431142.
Article36. Hohenfellner M, Steinbach F, Schultz-Lampel D, Schantzen W, Walter K, Cramer BM, et al. The nutcracker syndrome: new aspects of pathophysiology, diagnosis and treatment. J Urol. 1991; 146:685–688. PMID: 1875472.
Article37. Fitoz S, Ekim M, Ozcakar ZB, Elhan AH, Yalcinkaya F. Nutcracker syndrome in children: the role of upright position examination and superior mesenteric artery angle measurement in the diagnosis. J Ultrasound Med. 2007; 26:573–580. PMID: 17459998.38. Stewart BH, Reiman G. Left renal venous hypertension “nutcracker” syndrome: managed by direct renocaval reimplantation. Urology. 1982; 20:365–369. PMID: 7147503.39. Kim SH, Park JH, Han MC, Paick JS. Embolization of the internal spermatic vein in varicocele: significance of venous pressure. Cardiovasc Intervent Radiol. 1992; 15:102–106. PMID: 1571922.
Article40. Zerhouni EA, Siegelman SS, Walsh PC, White RI. Elevated pressure in the left renal vein in patients with varicocele: preliminary observations. J Urol. 1980; 123:512–513. PMID: 7365887.
Article41. Pallwein L, Pinggera G, Schuster AH, Klauser A, Weirich HG, Recheis W, et al. The influence of left renal vein entrapment on outcome after surgical varicocele repair: a color Doppler sonographic demonstration. J Ultrasound Med. 2004; 23:595–601. PMID: 15154525.42. Scultetus AH, Villavicencio JL, Gillespie DL. The nutcracker syndrome: its role in the pelvic venous disorders. J Vasc Surg. 2001; 34:812–819. PMID: 11700480.
Article43. Kim WS, Cheon JE, Kim IO, Kim SH, Yeon KM, Kim KM, et al. Hemodynamic investigation of the left renal vein in pediatric varicocele: Doppler US, venography, and pressure measurements. Radiology. 2006; 241:228–234. PMID: 16908673.
Article44. Barsoum MK, Shepherd RFJ, Welch TJ. Patient with both Wilkie syndrome and nutcracker syndrome. Vasc Med. 2008; 13:247–250. PMID: 18687762.
Article45. Inal M, Unal Daphan B, Karadeniz Bilgili MY. Superior mesenteric artery syndrome accompanying with nutcracker syndrome: a case report. Iran Red Crescent Med J. 2014; 16:e14755. PMID: 25763192.
Article46. Javaid MM, Ong CC, Subramanian S. Blood in urine: a hard nut to crack. Am J Med. 2017; 130:e89–e91. PMID: 27816446.
Article47. Sugimoto I, Ohta T, Ishibashi H, Takeuchi N, Nagata Y, Honda Y. Left renal vein entrapment syndrome (nutcracker syndrome) treated with left renal vein transposition. Jpn J Vasc Surg. 2001; 10:503–507.48. Barnes RW, Fleisher HL 3rd, Redman JF, Smith JW, Harshfield DL, Ferris EJ. Mesoaortic compression of the left renal vein (the so-called nutcracker syndrome): repair by a new stenting procedure. J Vasc Surg. 1988; 8:415–421. PMID: 3172376.
Article49. Shokeir AA, El-Diasty TA, Ghoneim MA. The nutcracker syndrome: new methods of diagnosis and treatment. Br J Urol. 1994; 74:139–143. PMID: 7921927.
Article50. Reed NR, Kalra M, Bower TC, Vrtiska TJ, Ricotta JJ 2nd, Gloviczki P. Left renal vein transposition for nutcracker syndrome. J Vasc Surg. 2009; 49:386–393. PMID: 19216958.
Article51. Xu D, Liu Y, Gao Y, Zhang L, Wang J, Che J, et al. Management of renal nutcracker syndrome by retroperitoneal laparoscopic nephrectomy with ex vivo autograft repair and autotransplantation: a case report and review of the literature. J Med Case Rep. 2009; 3:82. PMID: 19946558.
Article52. Hartung O. Nutcracker syndrome. Phlebolymphology. 2009; 16:246–252.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The role of Doppler ultrasonography in the detection and management of nutcracker syndrome
- Nutcracker Syndrome: Diagnostic Usefulness of Doppler US
- Spontaneous Resolution of Childhood Nutcracker Syndrome
- Superior Mesenteric Artery Syndrome Combined with Renal Nutcracker Syndrome in a Young Male: A Case Report
- A Case of the Nutcracker Syndrome
