Living donor liver transplantation with total pancreatectomy and portal vein homograft replacement in a pediatric patient with advanced pancreatoblastoma
- Affiliations
-
- 1Division of Pediatric Surgery, Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 2Division of Hepatobiliary Surgery and Liver Transplantation, Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. shwang@amc.seoul.kr
- 3Department of Pediatrics, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2471194
- DOI: http://doi.org/10.14701/ahbps.2020.24.1.78
Abstract
- Pancreatoblastoma is a malignant exocrine pancreatic tumor that is usually present in childhood. We herein present one case of pediatric living donor liver transplantation (LDLT) combined with spleen-preserving regional total pancreatectomy and portal vein homograft interposition in a 4-year-old boy with advanced pancreatoblastoma invading the portal and superior mesenteric veins. The size of the pancreatoblastoma was gradually reduced along systemic chemotherapy, thus we decided to perform surgery to remove it completely. A cold-stored fresh iliac vein homograft was prepared. Initially, a spleen-preserving distal pancreatectomy was performed. Thereafter, a completion regional total pancreatectomy was performed under superior mesenteric vein-vena cava bypass. A left liver graft from his mother was implanted according to the standardized procedures with portal vein interposition. This patient recovered uneventfully and is currently undergoing scheduled adjuvant chemotherapy. To our knowledge, this is the world-second case of pediatric LDLT for advanced pancreatoblastoma. Availability of fresh vein homografts is helpful to expand the indication of pediatric LDLT.
MeSH Terms
Figure
-
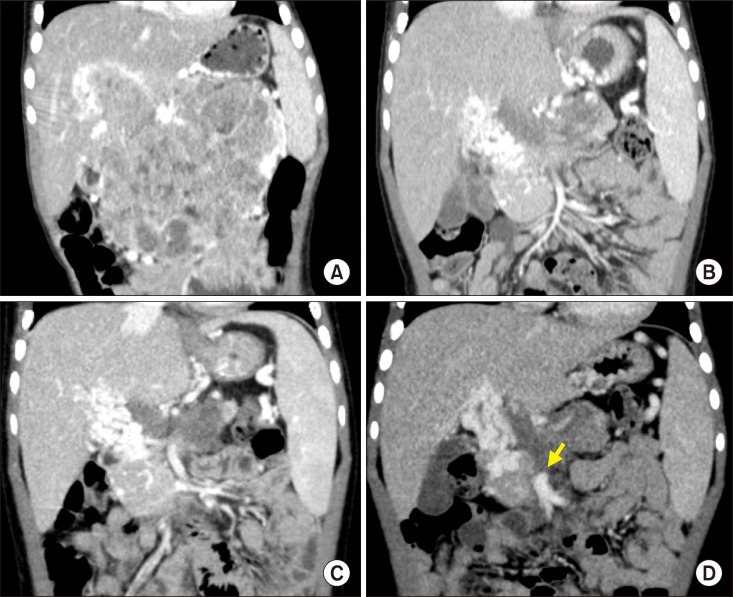
Fig. 1 Pretransplant computed tomography findings. The size of pancreatoblastoma was gradually reduced according to the neoadjuvant chemotherapy, showing serial size changes as follows: at diagnosis (A), five months before transplantation, (B) one month before transplantation, and (C) one week before transplantation (D). An arrow indicates the proximal end of the superior mesenteric vein.
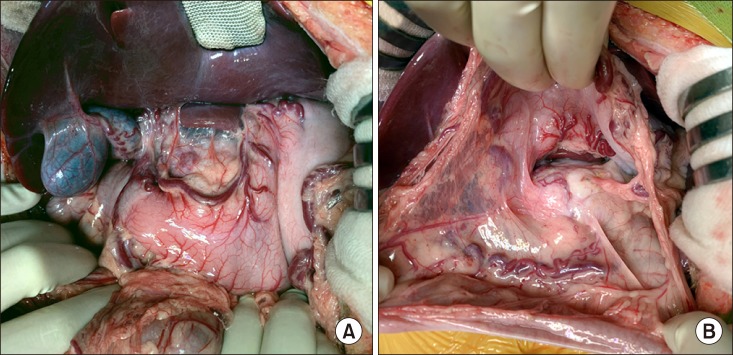
Fig. 2 Intraoperative photographs of the recipient's abdomen. No peritoneal seeding was identified at the mesenteric side (A) and around the pancreas (B).
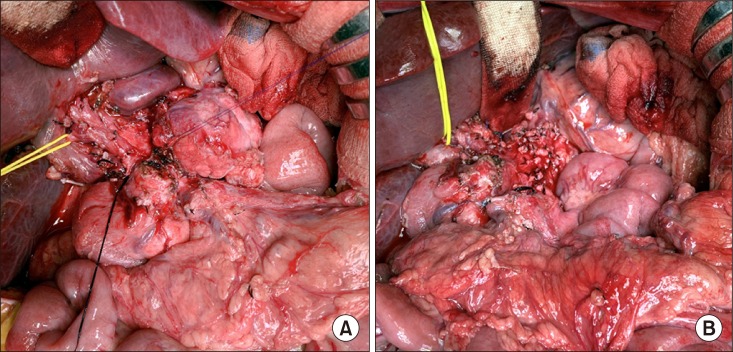
Fig. 3 Intraoperative photographs of spleen-preserving distal pancreatectomy. The pancreas body was transected to facilitate pancreatic resection (A). The celiac axis area was completely dissected (B).
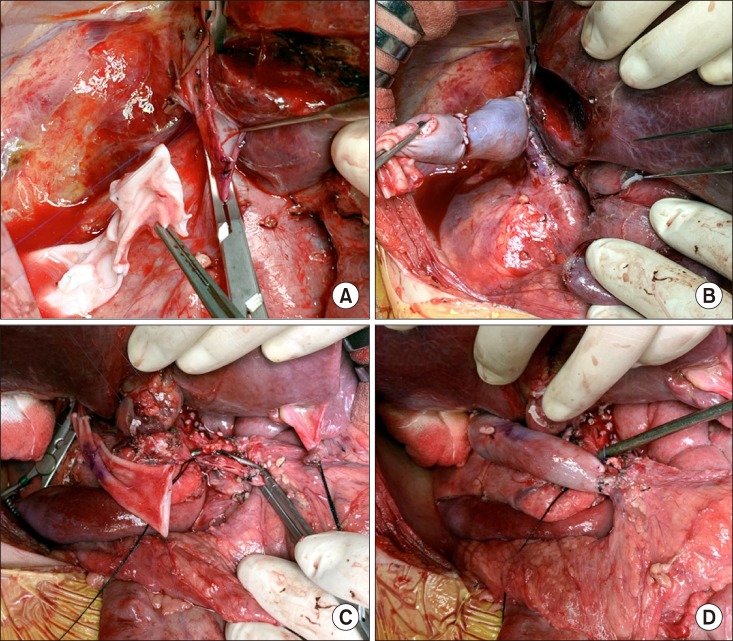
Fig. 4 Intraoperative photographs of the superior mesenteric vein-vena cava bypass using a cold-stored fresh iliac vein homograft. The vein graft is anastomosed to the retrohepatic inferior vena cava (A and B). The vein conduit was anastomosed to the superior mesenteric vein as an end-to-side fashion (C and D).
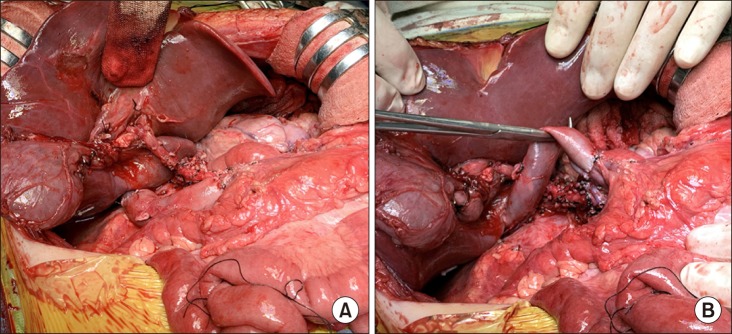
Fig. 5 Intraoperative photographs of spleen-preserving regional total pancreatectomy. The common hepatic artery was preserved with extensive lymph node dissection (A). Superior mesenteric vein-caval bypass was maintained during pancreatectomy (B).
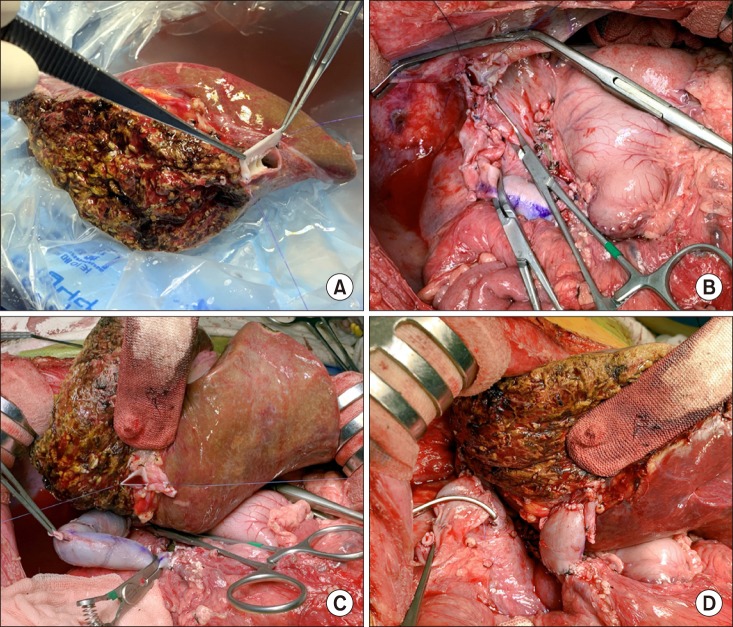
Fig. 6 Intraoperative photographs of the left liver graft implantation. The graft hepatic vein orifices were unified with an iliac vein patch (A). The recipient's native liver was removed with clamping of the superior mesenteric vein-caval bypass (B). The venous bypass was clamped (C). The iliac vein conduit was anastomosed to the graft portal vein (D).
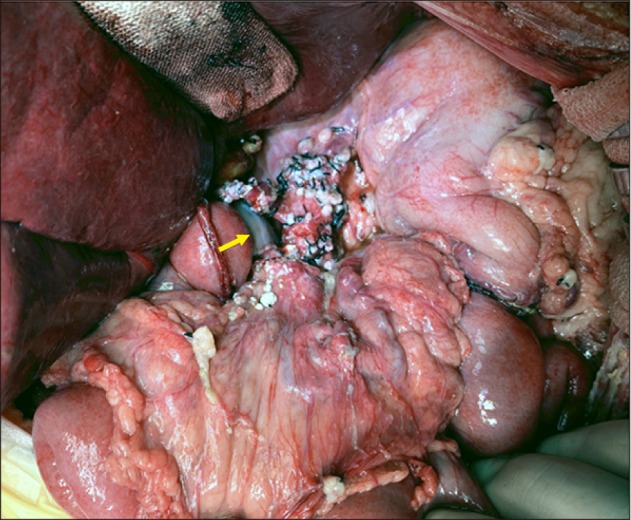
Fig. 7 Intraoperative photographs of the recipient's abdomen after graft implantation. The extent of dissection was visualized. An arrow indicates the interposed iliac vein homograft.
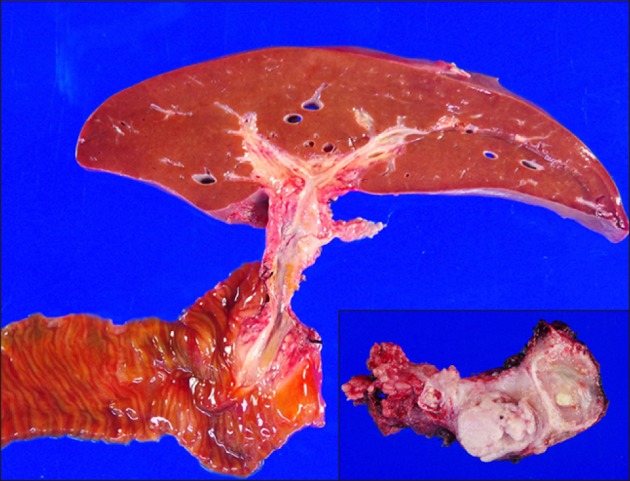
Fig. 8 Gross photographs of the resected specimens including the liver, pancreas and duodenum.
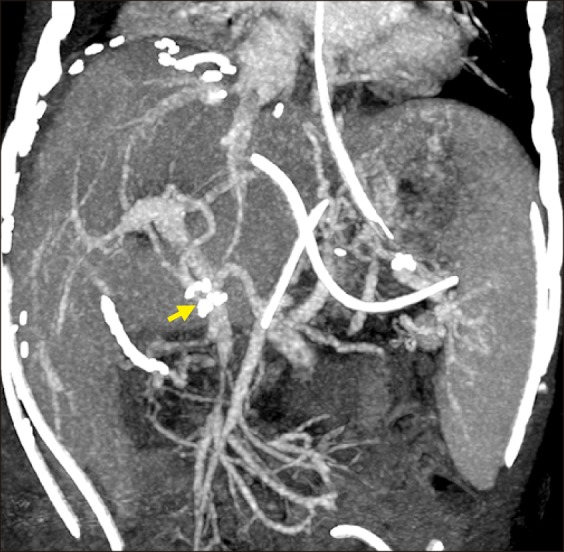
Fig. 9 Posttransplant computed tomography finding showing streamlined reconstruction figures of the graft hepatic and portal veins taken one week after transplantation. An arrow indicates the interposed iliac vein homograft.
Cited by 1 articles
-
Living donor liver retransplantation for primary non-function of liver graft following multivisceral transplantation in a pediatric patient
Shin Hwang, Dae-Yeon Kim, Jung-Man Namgoong, Kyung-Mo Kim, Seak Hee Oh, Ki-Hun Kim, Chul-Soo Ahn, Hyunhee Kwon, Yu Jeong Cho, Yong Jae Kwon
Ann Hepatobiliary Pancreat Surg. 2020;24(2):198-202. doi: 10.14701/ahbps.2020.24.2.198.
Reference
-
1. Dhebri AR, Connor S, Campbell F, Ghaneh P, Sutton R, Neoptolemos JP. Diagnosis, treatment and outcome of pancreatoblastoma. Pancreatology. 2004; 4:441–451. discussion 452–453. PMID: 15256806.
Article2. Défachelles AS, Martin De, Boutard P, Nelken B, Schneider P, Patte C. Pancreatoblastoma in childhood: clinical course and therapeutic management of seven patients. Med Pediatr Oncol. 2001; 37:47–52. PMID: 11466723.
Article3. Glick RD, Pashankar FD, Pappo A, Laquaglia MP. Management of pancreatoblastoma in children and young adults. J Pediatr Hematol Oncol. 2012; 34 Suppl 2:S47–S50. PMID: 22525406.
Article4. Bien E, Godzinski J, Dall'igna P, Defachelles AS, Stachowicz-Stencel T, Orbach D, et al. Pancreatoblastoma: a report from the European cooperative study group for paediatric rare tumours (EXPeRT). Eur J Cancer. 2011; 47:2347–2352. PMID: 21696948.
Article5. Ghaffarian AA, Book L, Meyers RL. Liver transplant for metastatic pancreatoblastoma: 7-year event-free survival after chemotherapy, pancreatectomy, complete hepatectomy, and liver transplant. Pediatr Transplant. 2018; DOI: 10.1111/petr.13098.
Article6. Cho HD, Hwang S, Lee YJ, Park KM, Kim KH, Kim JC, et al. Changes in the types of liver diseases requiring hepatic resection: a single-institution experience of 9016 cases over a 10-year period. Korean J Hepatobiliary Pancreat Surg. 2016; 20:49–52. PMID: 27212990.
Article7. Ibuka S, Uehara S, Ueno T, Oue T, Miyamura T, Hashii Y, et al. Complete resection of pancreatoblastoma with portal vein obstruction after high-dose chemotherapy: a case report. J Pediatr Hematol Oncol. 2017; 39:e275–e278. PMID: 28538503.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Living donor liver transplantation with proximal splenic vein ligation in a pediatric patient with congenital absence of the portal vein
- Portal vein fenestration: a case report of an unusual portal vein developmental anomaly
- Portal vein interposition in living donor liver transplantation for a pediatric hepatoblastoma patient with portal vein tumor thrombosis
- Living-donor liver transplantation with inferior vena cava replacement in an infant recipient with advanced hepatoblastoma
- Tailored standardization of portal vein reconstruction for pediatric liver transplantation at Asan Medical Center
