Living-donor liver transplantation with inferior vena cava replacement in an infant recipient with advanced hepatoblastoma
- Affiliations
-
- 1Division of Pediatric Surgery, Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 2Division of Hepatobiliary Surgery and Liver Transplantation, Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. shwang@amc.seoul.kr
- 3Department of Pediatrics, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2471193
- DOI: http://doi.org/10.14701/ahbps.2020.24.1.72
Abstract
- Replacement of the inferior vena cava (IVC) after concurrent resection of hepatoblastoma-containing liver and retrohepatic IVC is regarded as a feasible option for pediatric living-donor liver transplantation (LDLT). This technique makes the extent of resection of LDLT comparable to that of deceased-donor liver transplantation (DDLT). We present one case of pediatric LDLT with IVC homograft replacement for advanced hepatoblastoma. The patient was a 10-kg 18-month-old girl suffering from large multiple hepatoblastomas, which were partially regressed by neoadjuvant chemotherapy. Because the tumors had invaded the retrohepatic IVC, there was a high risk of residual tumor cells at the IVC if it was preserved. Thus, we decided to replace the IVC during the LDLT operation. After a cold-stored fresh iliac vein homograft was prepared, we performed LDLT using her mother's left lateral section liver graft. A 4-cm-long common iliac vein homograft was attached to the liver graft at the back table. The left lateral-section graft with IVC attachment was implanted using the standard procedures like those of DDLT. We also did portal vein graft interposition. The patient recovered uneventfully and has been undergoing scheduled adjuvant chemotherapy to date. This is our second case of IVC homograft replacement for pediatric LDLT. In pediatric recipients, various vein homografts, such as iliac vein, IVC, and other large veins, can be used depending on the body size of the recipient and availability of vein homografts.
Keyword
MeSH Terms
Figure
-
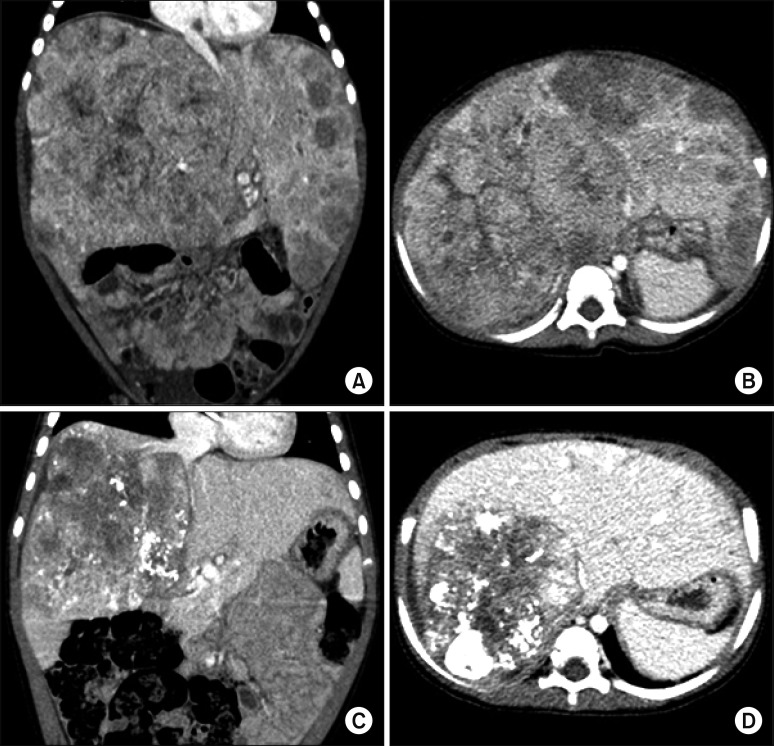
Fig. 1 Pretransplant computed tomography findings. At five months before the liver transplantation operation, huge multiple tumors occupied the whole liver, and the abdomen was distended by the enlarged liver (A and B). At one month before liver transplantation, the tumor size was markedly regressed (C and D), but the retrohepatic inferior vena cava was invaded by the tumors (C).
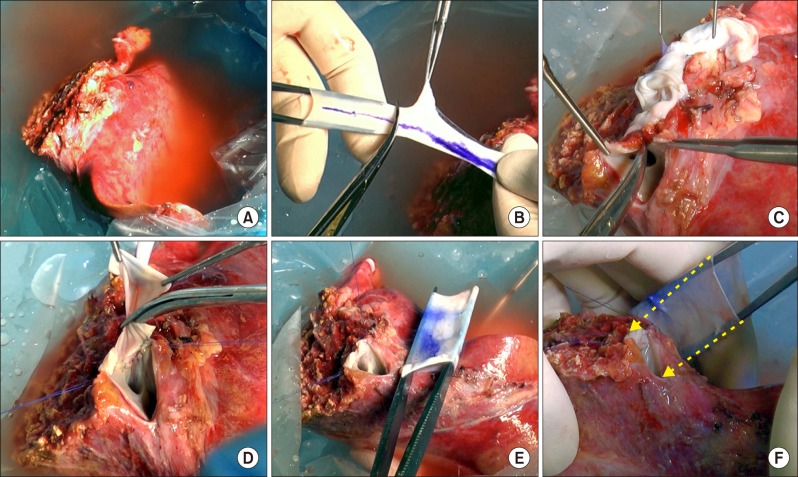
Fig. 2 Intraoperative photographs of the bench work. (A) A left lateral section graft was harvested from her mother. (B) The iliac-vein homograft was divided into two parts as the common iliac vein portion and external iliac-vein portion. (C) The graft hepatic vein orifice was incised for venoplasty. (D) An iliac vein patch was applied to the incised defect. (E) The sizes of the enlarged graft hepatic vein orifice and common iliac vein homograft were matched. (F) The 4-cm-long common iliac vein homograft was attached to replace the retrohepatic inferior vena cava (arrows).
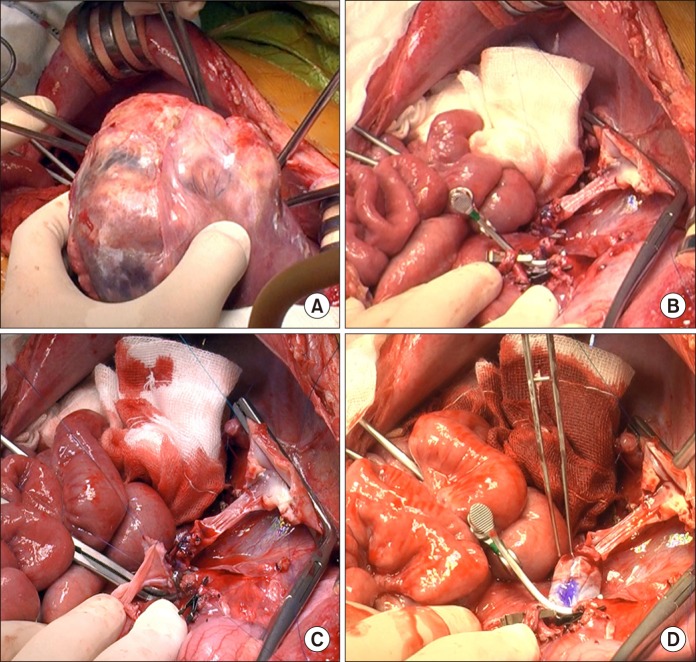
Fig. 3 Intraoperative photographs of the recipient hepatectomy and portal vein interposition venoplasty. (A) The recipient's native liver was removed. (B) Some part of the retrohepatic vein wall remained. (C) Portal vein venoplasty was done with interposition of an external iliac vein homograft. (D) The reconstructed portal vein was temporarily distended to check the security of anastomosis.
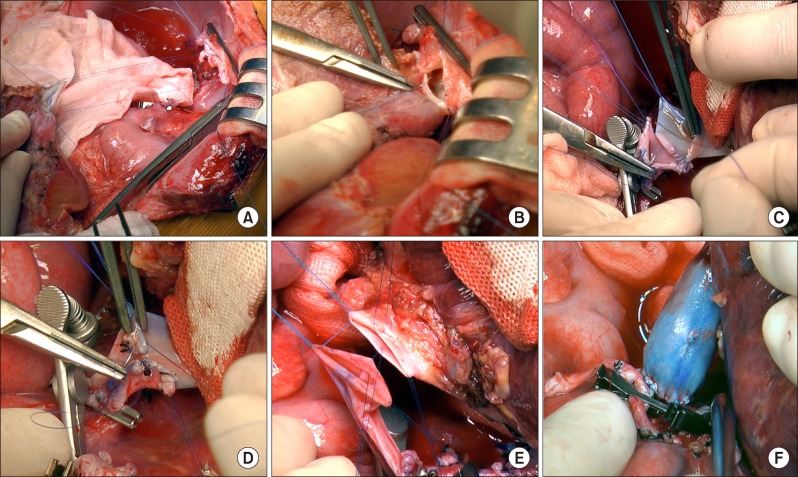
Fig. 4 Intraoperative photographs of the graft implantation. (A and B) The suprahepatic end of the vena cava was anastomosed to the graft hepatic veins. (C and D) The infrahepatic end of the vena cava was anastomosed to the interposed vein homograft after size matching. (E and F) The graft portal vein was anastomosed with the interposed external iliac vein homograft.
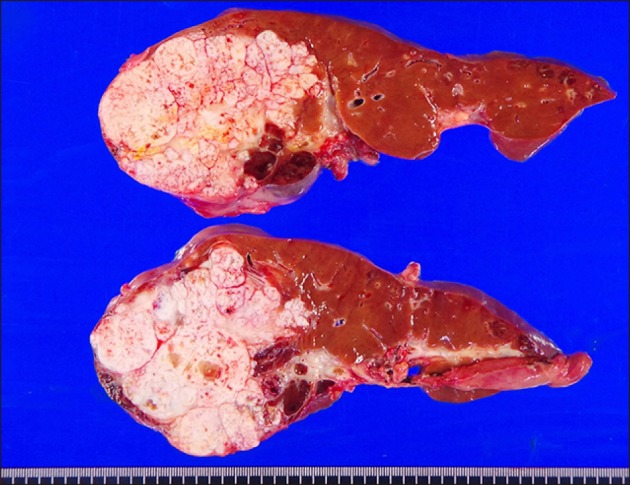
Fig. 5 Gross photographs of the explanted liver. There were multiple viable tumors with extensive necrosis.
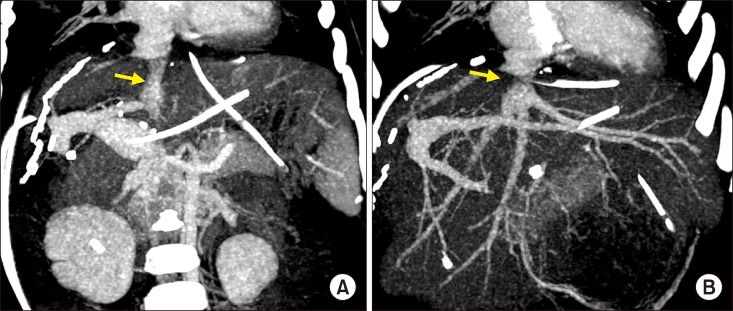
Fig. 6 Post-transplant computed tomography finding taken after five days. (A) The replaced retrohepatic inferior vena cava conduit is visualized (arrow). (B) The anastomosis site at the graft hepatic vein is visualized (arrow).
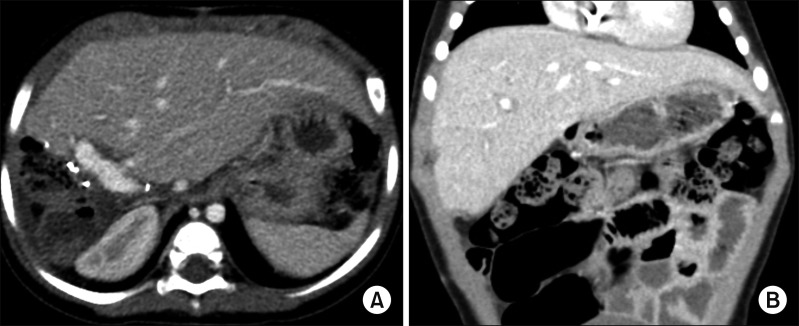
Fig. 7 Post-transplant computed tomography finding taken after 32 days. The normal-looking liver filled the abdomen without any vascular complication (A and B).
Cited by 4 articles
-
Hilar portal vein wedge resection and patch venoplasty in patients undergoing bile duct resection for hepatobiliary malignancy: A report of two cases
Sung-Min Kim, Shin Hwang
Ann Hepatobiliary Pancreat Surg. 2021;25(1):132-138. doi: 10.14701/ahbps.2021.25.1.132.Pediatric split liver transplantation for congenital factor X deficiency: first 10-year follow-up of a case with portal vein stenting
Jung-Man Namgoong, Shin Hwang, Dae-Yeon Kim, Tae-Yong Ha, Gi-Won Song, Dong-Hwan Jung, Kyung Mo Kim, Seak Hee Oh
Korean J Transplant. 2021;35(1):66-70. doi: 10.4285/kjt.20.0039.Portal vein wedge resection and patch venoplasty using autologous and homologous vein grafts during surgery for hepatobiliary malignancies
Byeong-Gon Na, Shin Hwang, Dong-Hwan Jung, Sung-Gyu Lee
Ann Hepatobiliary Pancreat Surg. 2021;25(4):509-516. doi: 10.14701/ahbps.2021.25.4.509.Patch venoplasty for resecting tumor invading the retrohepatic inferior vena cava using total and selective hepatic vascular exclusion
Sung-Min Kim, Shin Hwang, Deok-Bog Moon, Dong-Hwan Jung, Sung-Gyu Lee
Ann Hepatobiliary Pancreat Surg. 2021;25(4):536-543. doi: 10.14701/ahbps.2021.25.4.536.
Reference
-
1. Namgoong JM, Choi JU, Hwang S, Oh SH, Park GC. Pediatric living donor liver transplantation with homograft replacement of retrohepatic inferior vena cava for advanced hepatoblastoma. Ann Hepatobiliary Pancreat Surg. 2019; 23:178–182. PMID: 31225421.
Article2. Sasaki K, Kasahara M, Fukuda A, Shigeta T, Tanaka H, Nakagawa S, et al. Living donor liver transplantation with vena cava reconstruction using a cryopreserved allograft for a pediatric patient with Budd-Chiari syndrome. Transplantation. 2009; 87:304–305. PMID: 19155990.
Article3. Chardot C, Saint Martin C, Gilles A, Brichard B, Janssen M, Sokal E, et al. Living-related liver transplantation and vena cava reconstruction after total hepatectomy including the vena cava for hepatoblastoma. Transplantation. 2002; 73:90–92. PMID: 11792985.4. Hwang S, Kim DY, Ahn CS, Moon DB, Kim KM, Park GC, et al. Computational simulation-based vessel interposition reconstruction technique for portal vein hypoplasia in pediatric liver transplantation. Transplant Proc. 2013; 45:255–258. PMID: 23375311.
Article5. Aavik A, Kibur RT, Lieberg J, Lepner U, Aunapuu M, Arend A. Cold-stored venous allografts in different preserving solutions: a study on changes in vein wall morphology. Scand J Surg. 2019; 108:67–75. PMID: 30319041.
Article6. Aydin C, Ince V, Otan E, Akbulut S, Koc C, Kayaalp C, et al. Storage of allogeneic vascular grafts: experience from a high-volume liver transplant institute. Int Surg. 2013; 98:170–174. PMID: 23701155.
Article7. Kim SH, Hwang S, Ha TY, Song GW, Jung DH, Ahn CS, et al. Usability of cryopreserved aortic allografts for middle hepatic vein reconstruction during living-donor liver transplantation. J Gastrointest Surg. 2016; 20:1049–1055. PMID: 26666546.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Retrohepatic inferior vena cava interposition in living donor liver transplantation for a pediatric patient with advanced hepatoblastoma
- Pediatric living donor liver transplantation with homograft replacement of retrohepatic inferior vena cava for advanced hepatoblastoma
- Technical refinement of inferior vena cava replacement using a synthetic vascular graft in living donor liver transplantation
- Inferior vena cava stenosis-induced sinusoidal obstructive syndrome after living donor liver transplantation
- Tailored techniques of graft outflow vein reconstruction in pediatric liver transplantation at Asan Medical Center
