Ultrasonography of Pediatric Superficial Soft Tissue Tumors and Tumor-Like Lesions
- Affiliations
-
- 1Department of Radiology, Sungkyunkwan University School of Medicine, Samsung Medical Center, Seoul, Korea. sy1131.yoo@samsung.com
- 2Department of Radiology, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 3Department of Radiology, Korea University Medical Center, Seoul, Korea.
- KMID: 2470758
- DOI: http://doi.org/10.3348/kjr.2019.0343
Abstract
- Ultrasonography (US) is usually the first imaging examination performed to evaluate palpable or visible superficial soft tissue lesions that are common in children. Although clinical assessments, such as age at presentation, clinical course, and overlying skin discoloration, are important for the differentiation of pediatric soft tissue lesions, US allows a specific diagnosis of some typical benign lesions and helps in guiding further investigation since it provides detailed information about the lesion location, characterization including solid versus cystic, vascularity, and compressibility. Therefore, sufficient knowledge of the normal anatomy, proper ultrasonographic techniques, and the imaging findings of common and uncommon soft tissue lesions in children are crucial for accurate assessment and management of patients. In this article, we review the techniques and imaging findings focusing on the ultrasonographic features of a variety of superficial soft tissue lesions detected in children.
Keyword
Figure
-
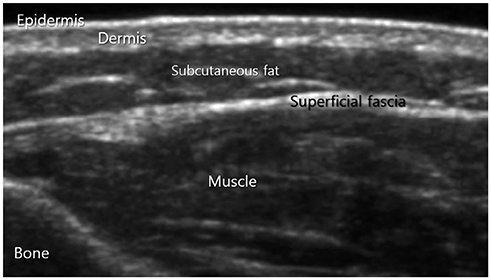
Fig. 1 Visualization of normal soft tissue structure at dorsal aspect of forearm by US. US = ultrasonograpy
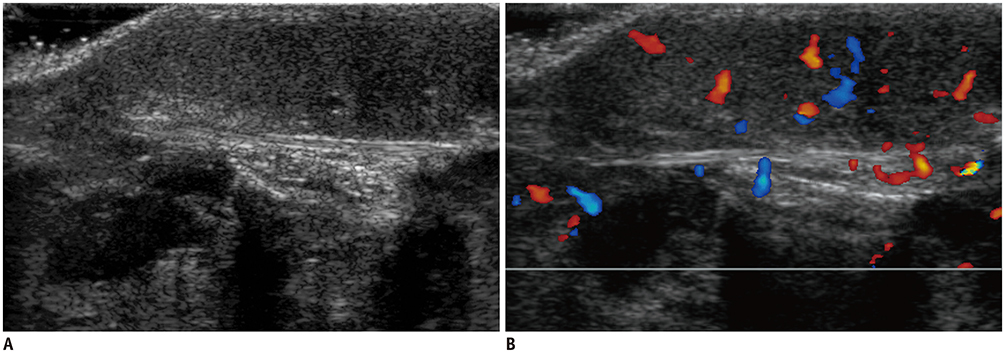
Fig. 2 Infantile hemangioma in 8-month-old girl with enlarging foot mass. US (A) shows well-defined ovoid hypoechoic mass confined to subcutaneous fat. Color Doppler scan (B) shows increased vascular flow.
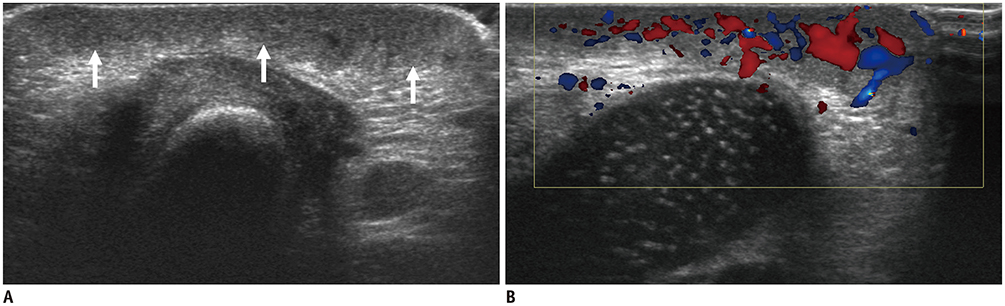
Fig. 3 Congenital hemangioma in 2-day-old boy at knee present at birth. US (A) shows homogeneous hypoechoic lesion in subcutaneous fat layer (arrows). Color Doppler scan (B) shows markedly increased vascular flow.
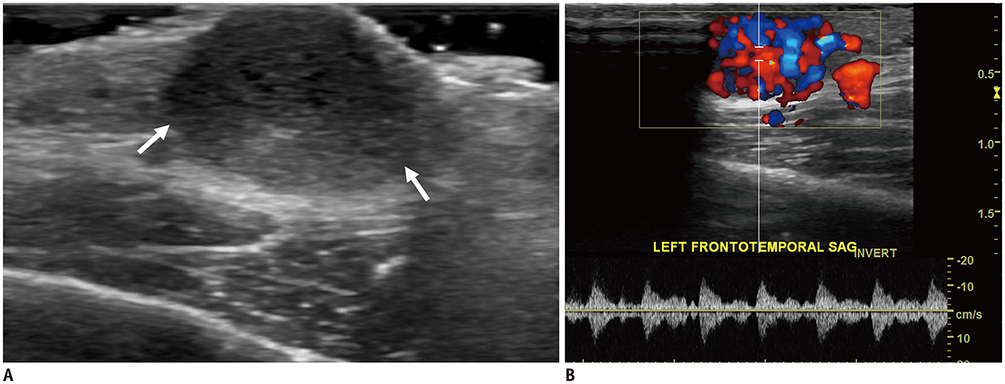
Fig. 4 Lobular capillary hemangioma in 13-year-old girl with enlarging soft tissue mass at scalp. US (A) shows well-defined slightly heterogeneous hypoechoic nodule on skin and subcutaneous fat layer (arrows). Color Doppler scan (B) shows increased vascular flow within nodule.
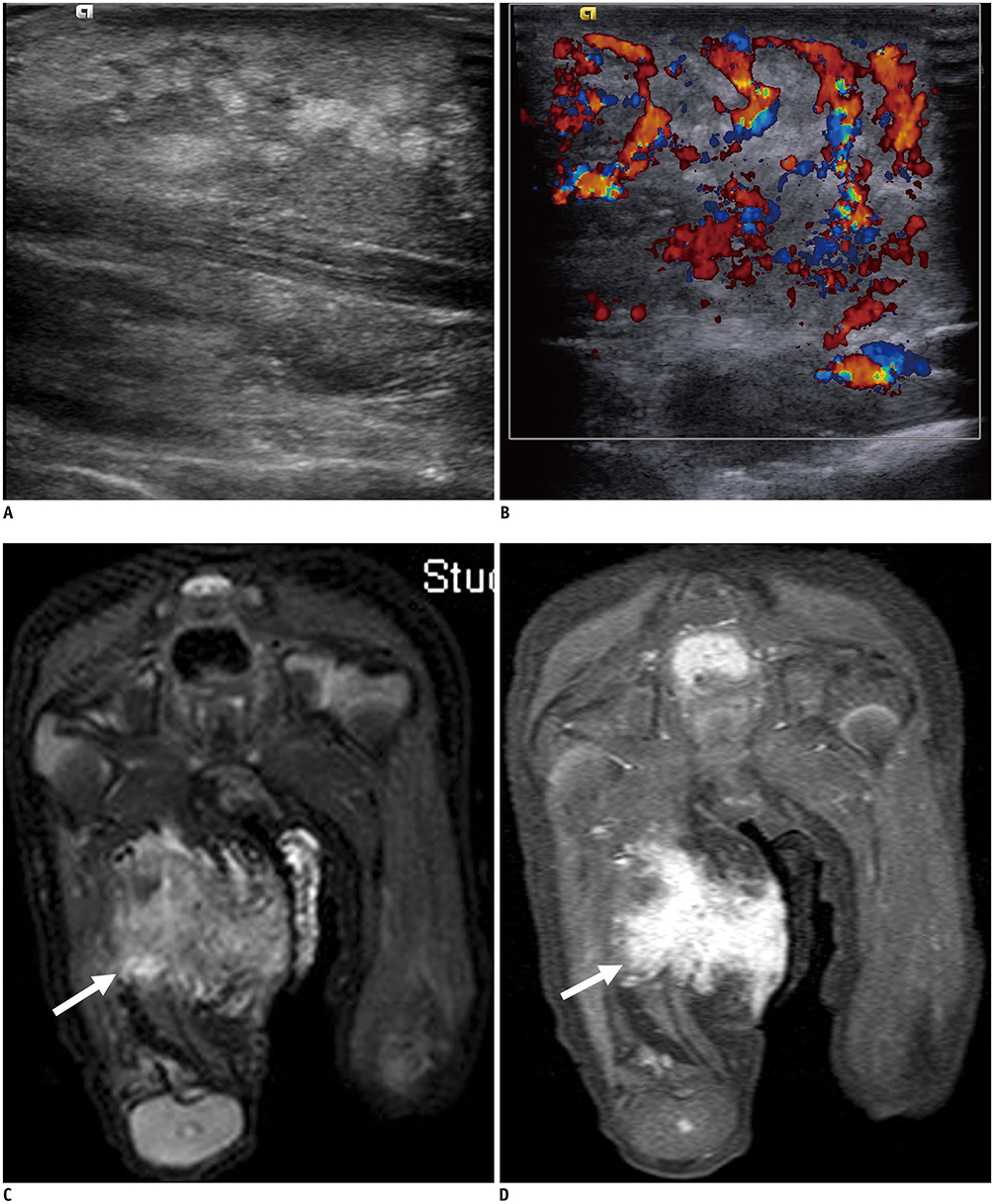
Fig. 5 Kaposiform hemangioendothelioma at right thigh in 2-day-old girl with Kasabach-Merritt phenomenon. US (A) shows large ill-defined heterogeneous mass, which infiltrates subcutaneous tissue and underlying musculature with marked skin thickening. Color Doppler scan (B) shows increased vascular flow with high velocity of lesion. Coronal fat-suppressed T2-weighted MRI (C) shows heterogeneous high signal intensity mass (arrow). Contrast-enhanced coronal fat-suppressed T1-weighted MRI (D) shows prominent enhancement of mass (arrow).
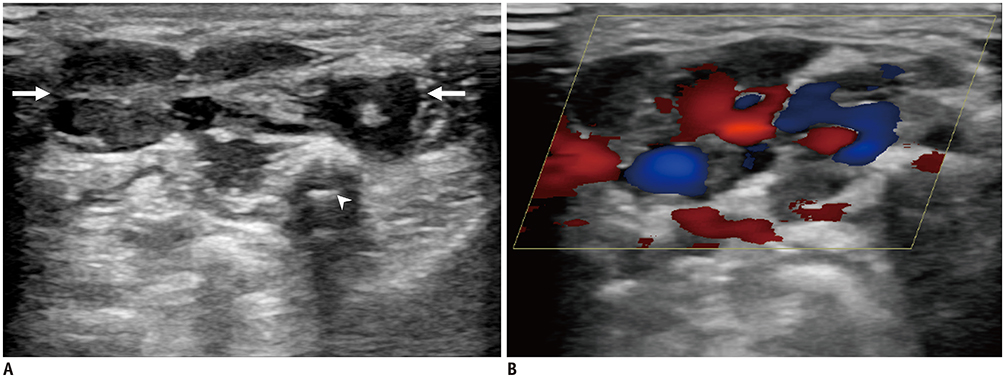
Fig. 6 Venous malformation in 9-year old boy presented with mass in hand. US (A) shows inter-/intra-muscular lesion containing anechoic serpentine structure (arrows) with increased internal echogenicity due to slow blood flow. There is focal hyperechoic lesion with posterior acoustic shadowing, suggesting phlebolith (arrowhead). Color Doppler scan (B) shows venous flow.
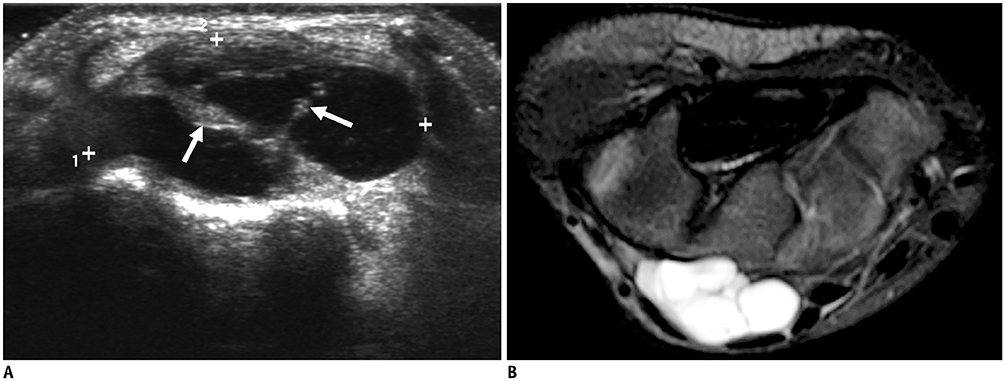
Fig. 7 Lymphatic malformation in 9-year-old girl with palpable mass at wrist dorsum. US (A) shows multiloculated cyst (between cursors) in subcutaneous fat layer with internal septa (arrows) and some echogenic debris. Axial fat-suppressed T2-weighted image (B) shows multiloculated cyst with internal septa.
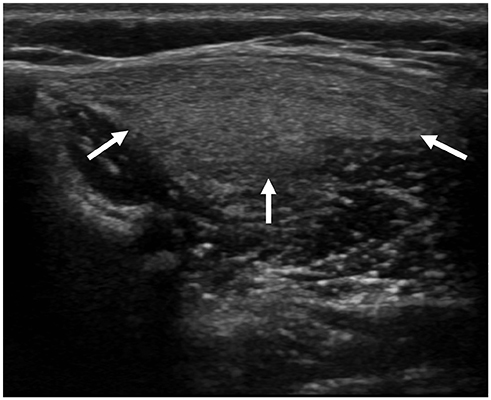
Fig. 8 Lipoma in 9-month-old girl with lump on back. US shows ill-defined ovoid hyperechoic mass (arrows) confined within right paravertebral muscle.

Fig. 9 Lipoblastoma in 5-month-old girl with gradually enlarging buttock mass from birth. US (A) shows heterogeneous, mainly hyperechoic mass (arrows), with intervening hypoechoic areas. Axial T1-weighted MRI (B) shows well-demarcated high signal intensity mass (arrows) involving gluteus muscle and subcutaneous fat. There are some intervening hyperintense strands (arrowheads). Axial fat-suppressed T2-weighted MRI (C) shows mainly high signal intensity mass (arrows) with intervening linear hypointense strands suggesting fat component (arrowheads).
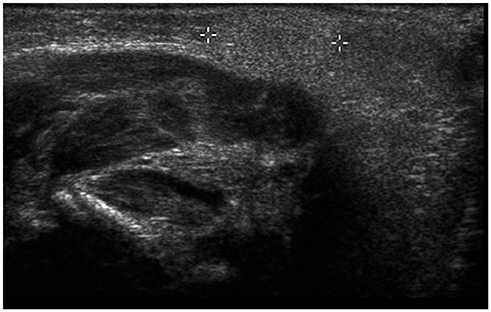
Fig. 10 Subcutaneous fat necrosis of newborn in 1-month-old boy with small palpable mass at posterior neck. US shows homogeneous echogenic nodule (between cursors) at subcutaneous fat layer without cystic changes or calcification.
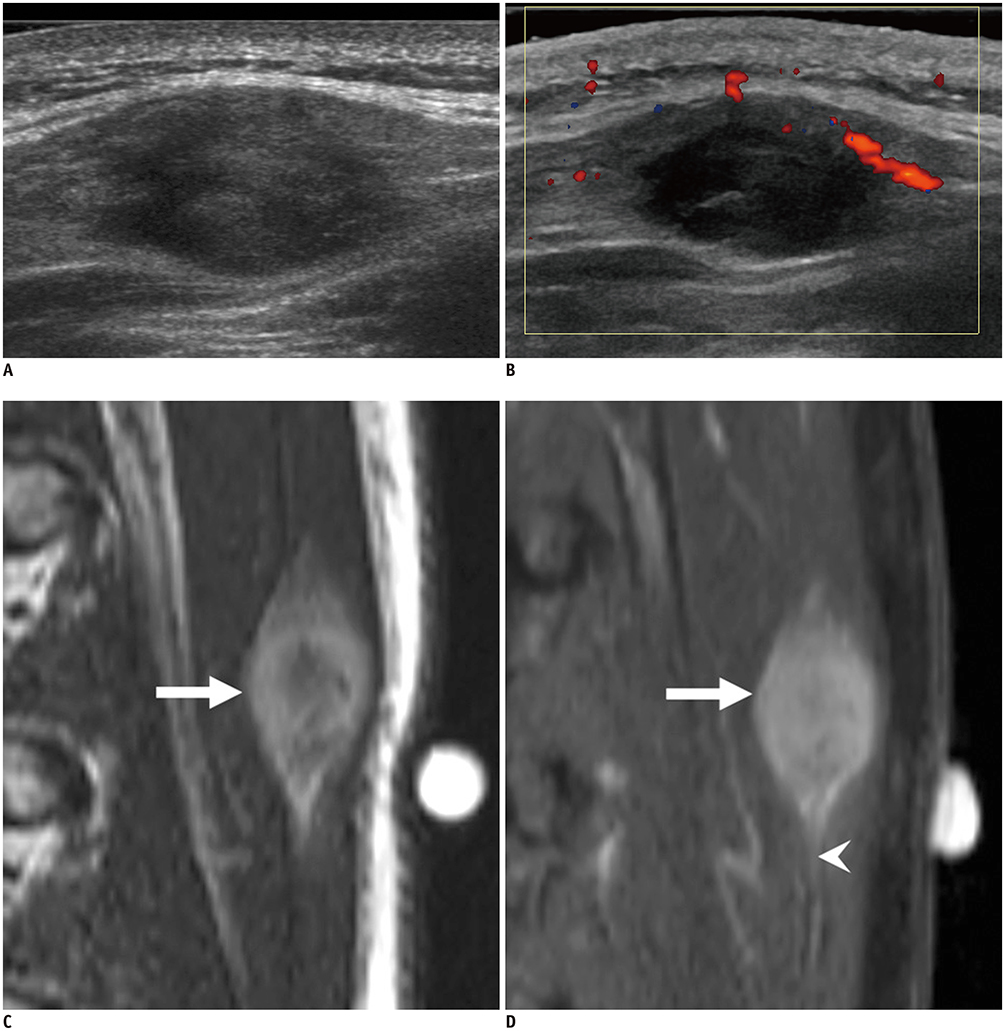
Fig. 11 Nodular fasciitis in 14-year-old boy on back. US (A) shows well-defined ovoid hypoechoic lesion confined within muscle abutting fascia. Color Doppler scan (B) shows mild peripheral vascularity. Sagittal T2-weighted MRI (C) shows well-demarcated ovoid high signal intensity mass (arrow) within back muscle. Contrast-enhanced sagittal T1-weighted MRI (D) shows diffuse enhancement of mass (arrow) with fascial tail sign (arrowhead).

Fig. 12 Fibrous hamartoma of infancy in 8-month-old boy with slowly growing palpable lump at upper arm. US shows well-defined heterogeneous lesion (arrows) with alternating hyperechoic and hypoechoic areas.
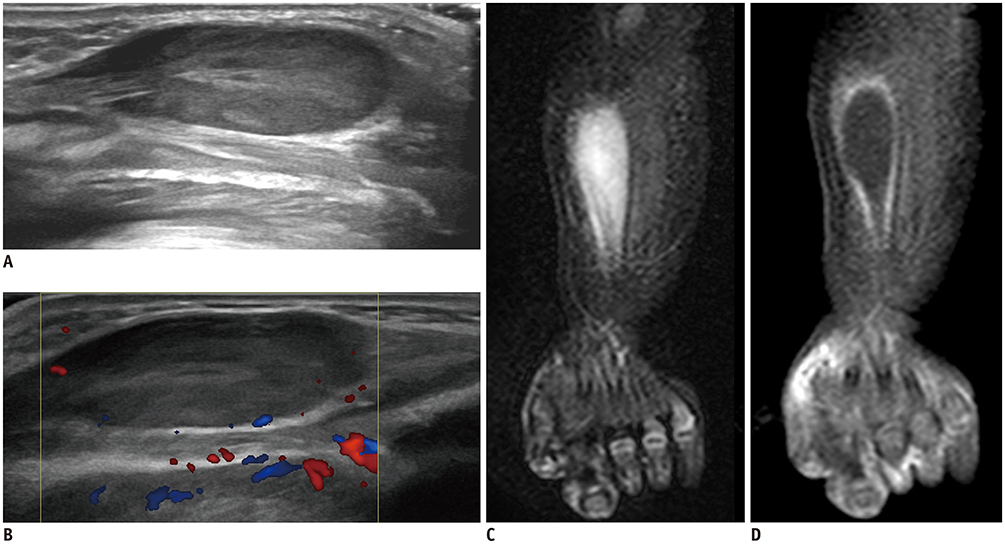
Fig. 13 Infantile myofibromatosis in neonate presented with multiple palpable lesions. US (A, B) shows well-defined intramuscular hypoechoic mass with minimal peripheral vascularity at forearm. Additional lesions with similar characteristic were also founded at chest wall and buttock on US (not shown). Coronal fat-suppressed T2-weighted MRI (C) shows heterogeneous hyperintense mass with central fluid signal suggesting central necrosis. Contrast-enhanced coronal T1-weighted MRI (D) shows peripheral rim enhancement of lesion.
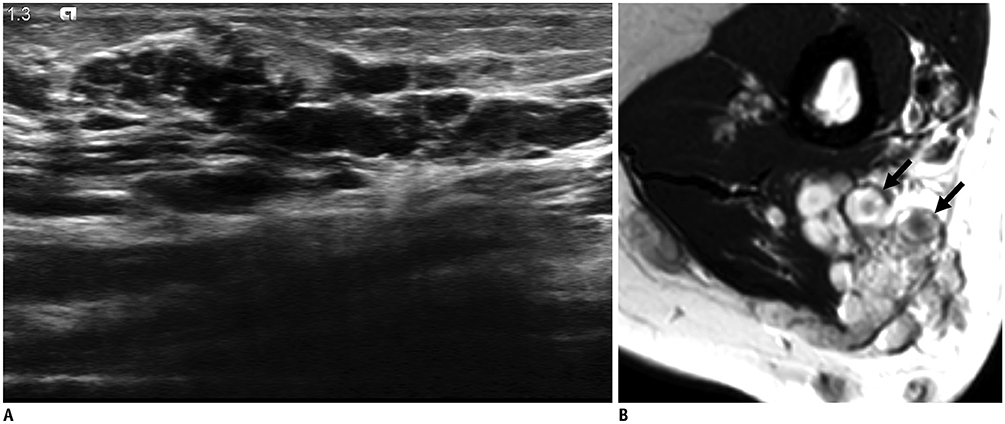
Fig. 14 Plexiform neurofibroma in 14-year-old girl with known neurofibromatosis type 1 and palpable masses on upper arm. US (A) shows conglomerated numerous serpiginous hypoechoic lesions at subcutaneous fat layer and muscle. Coronal T2-weighted MRI (B) shows conglomerated rounded hyperintense lesions with hypointense central foci known as “target sign” (arrows).
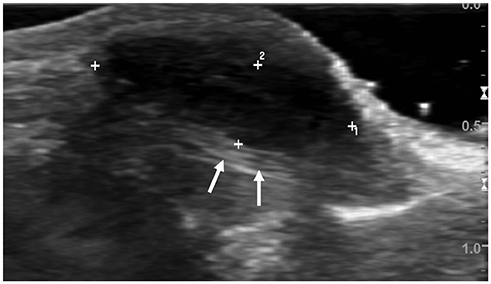
Fig. 15 Giant cell tumor of tendon sheath in 9-year-old girl with palpable mass at finger. US shows well-defined hypoechoic ovoid mass with lobulated contour at volar aspect of metacarpophalangeal joint, in close contact with but being separate from flexor tendon (arrows).

Fig. 16 Epidermal inclusion cyst in 4-year-old boy with palpable mass at chest wall. US shows well-demarcated, ovoid, hypoechoic lesion with posterior acoustic enhancement (arrow).
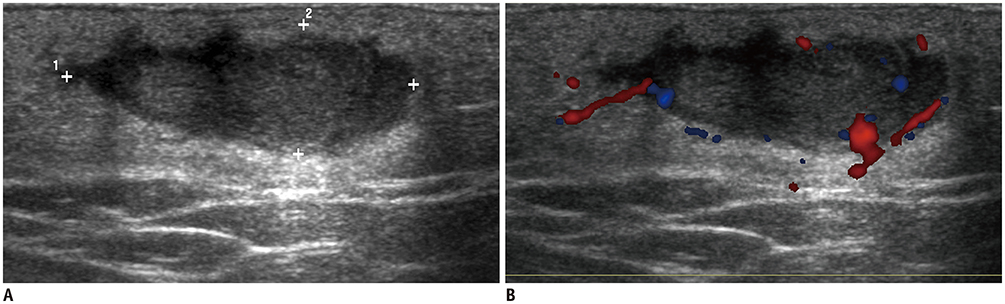
Fig. 17 Ruptured epidermal inclusion cyst in 13-year-old girl at buttock. US (A) shows irregular low echoic nodular lesion with adjacent fat inflammation. Color Doppler scan (B) shows peripheral vascularity

Fig. 18 Pilomatricoma in 6-year-old girl with small palpable nodule at pre-auricular area. US (A) shows well-defined ovoid solid lesion (arrows) at subcutaneous fat layer abutting dermis. Lesion shows heterogeneous echogenicity with echogenic calcified foci and increased perilesional fat echogenicity. Color Doppler scan (B) shows peripheral and central vascularity.
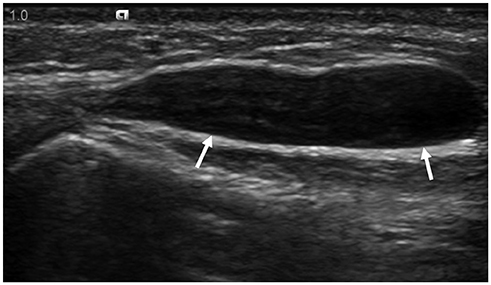
Fig. 19 Ganglion in 8-year-old girl at hand dorsum. US shows well-defined ovoid hypoechoic mass (arrows).
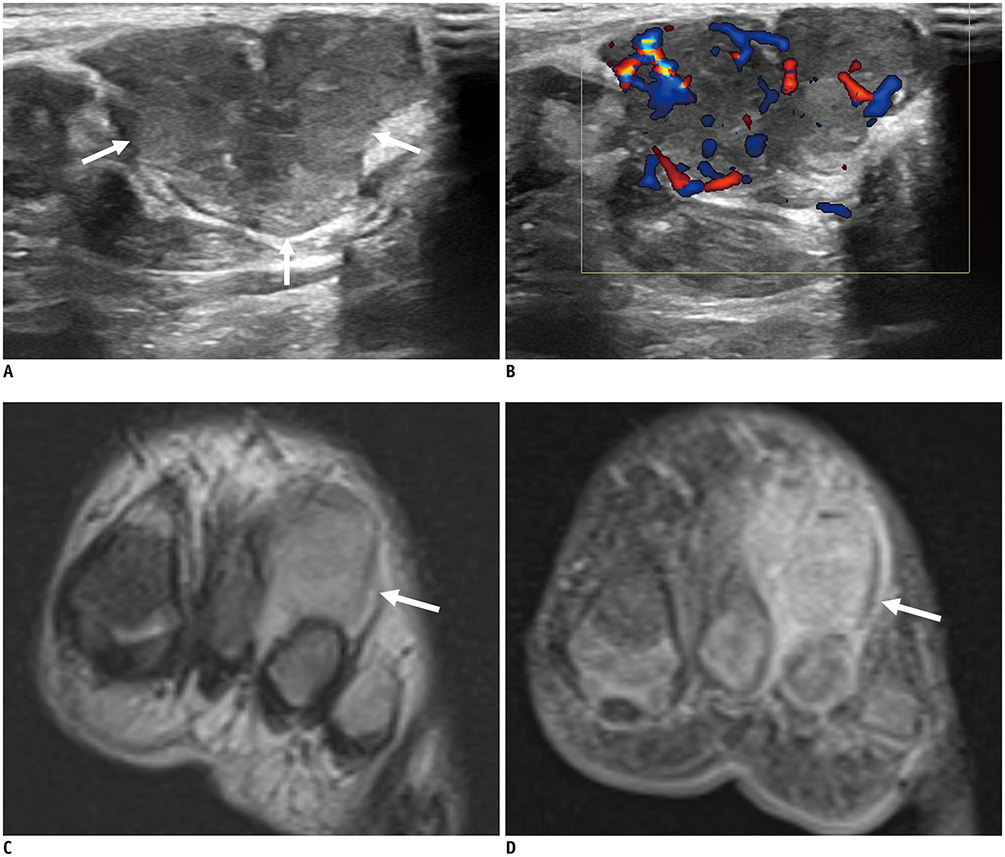
Fig. 20 Rhabdomyosarcoma in 11-month-old girl at foot dorsum. US (A) demonstrates well-circumscribed, lobulating contoured, heterogeneous mass (arrows) at foot dorsum. Color Doppler scan (B) shows increased intralesional vascularity. Metastatic lymphadenopathy has found on US of left inguinal region (not shown). Coronal T2-weighted MRI (C) shows lobulated hyperintense mass (arrow). Contrast-enhanced coronal T1-weighted MRI (D) shows diffuse enhancement of lesion (arrow). Findings are not specific and histopathological findings were needed for final diagnosis.
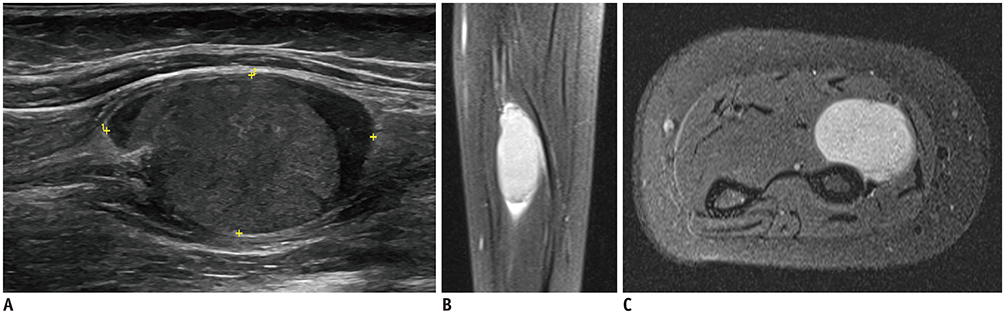
Fig. 21 Synovial sarcoma in 9-year-old girl at forearm. US (A) shows elliptical heterogeneous hypoechoic mass within muscle. Sagittal fat-suppressed T2-weighted MRI (B) shows well-demarcated ovoid hyperintense mass. Contrast-enhanced axial T1-weighted MRI (C) shows prominent enhancement of mass.
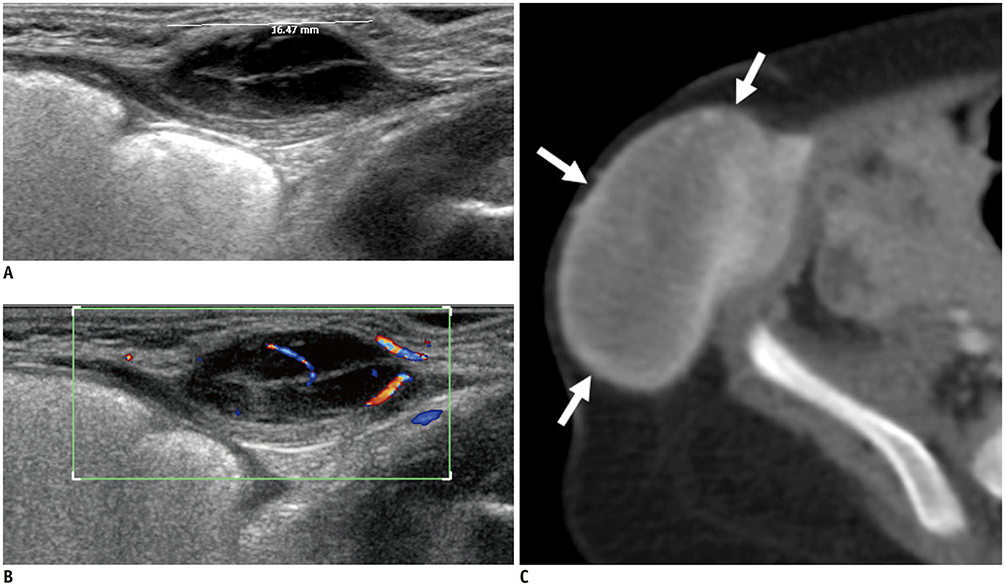
Fig. 22 Infantile fibrosarcoma in 1-month-old boy at abdominal wall. US (A) shows well-demarcated ovoid hypoechoic mass at subcutaneous fat layer. Color Doppler scan (B) shows slightly increased vascularity of mass. Contrast-enhanced CT scan which was taken 5 months later (C) shows markedly increased size of mass with heterogeneous enhancement (arrows).
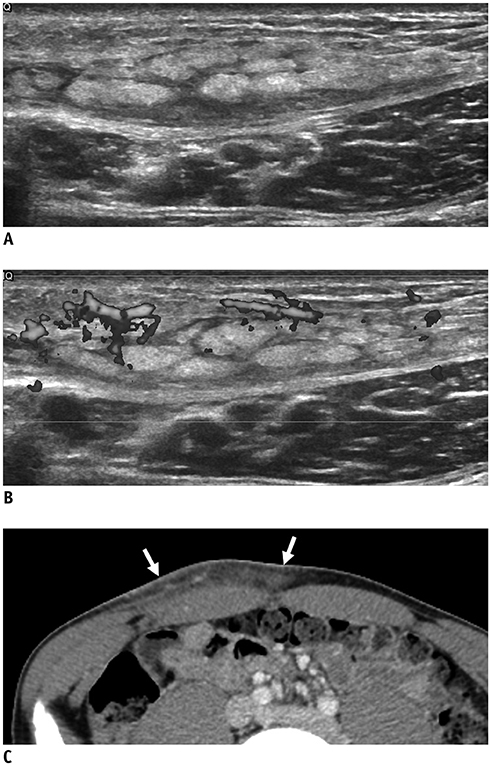
Fig. 23 Subcutaneous panniculitis-like T-cell lymphoma in 13-year-old boy with enlarging periumbilical mass. US (A) shows diffuse ill-defined hyperechoic lesion at subcutaneous fat layer with multiple linear hypoechoic mass. Color Doppler scan (B) shows increased vascularity within area. Subsequent contrast-enhanced CT (C) shows multiple enhancing nodular infiltrations at subcutaneous layer (arrows).

Fig. 24 Metastatic lesions in 3-year-old boy with adrenal neuroblastoma. US (A) shows lobulated hypoechoic solid masses at chest wall with minimal vascularity (arrows). Abdominal US (B) shows primary tumor in left adrenal gland, neuroblastoma (arrows).
Reference
-
1. Beaman FD, Kransdorf MJ, Andrews TR, Murphey MD, Arcara LK, Keeling JH. Superficial soft-tissue masses: analysis, diagnosis, and differential considerations. Radiographics. 2007; 27:509–523.
Article2. Wu JS, Hochman MG. Soft-tissue tumors and tumorlike lesions: a systematic imaging approach. Radiology. 2009; 253:297–316.
Article3. Navarro OM. Soft tissue masses in children. Radiol Clin North Am. 2011; 49:1235–1259. vi–vii.
Article4. Shah SH, Callahan MJ. Ultrasound evaluation of superficial lumps and bumps of the extremities in children: a 5-year retrospective review. Pediatr Radiol. 2013; 43 Suppl 1:S23–S40.
Article5. DiDomenico P, Middleton W. Sonographic evaluation of palpable superficial masses. Radiol Clin North Am. 2014; 52:1295–1305.
Article6. Carra BJ, Bui-Mansfield LT, O'Brien SD, Chen DC. Sonography of musculoskeletal soft-tissue masses: techniques, pearls, and pitfalls. AJR Am J Roentgenol. 2014; 202:1281–1290.
Article7. Campbell R. Ultrasound of soft tissue masses. In : Allan PL, Baxter GM, Weston MJ, editors. Clinical ultrasound. 2:3rd ed. London: Churchill Livingstone: Elsevier;2011. p. 1109–1125.8. Siegel MJ. Pediatric sonography. 5th ed. Philadelphia, PA: Wolters Kluwer;2019.9. ISSVA classification for vascular anomalies. ISSVA;2014. updated May 2018. Accessed September 22, 2019. Available at: http://www.issva.org/UserFiles/file/ISSVA-Classification-2018.pdf.10. Esposito F, Ferrara D, Di Serafino M, Diplomatico M, Vezzali N, Giugliano AM, et al. Classification and ultrasound findings of vascular anomalies in pediatric age: the essential. J Ultrasound. 2019; 22:13–25.
Article11. Enjolras O, Wassef M, Chapot R. Color atlas of vascular tumors and vascular malformations. 1st ed. Cambridge: Cambridge University Press;2007.12. Johnson CM, Navarro OM. Clinical and sonographic features of pediatric soft-tissue vascular anomalies part 1: classification, sonographic approach and vascular tumors. Pediatr Radiol. 2017; 47:1184–1195.
Article13. Olivieri B, White CL, Restrepo R, McKeon B, Karakas SP, Lee EY. Low-flow vascular malformation pitfalls: from clinical examination to practical imaging evaluation—Part 2, venous malformation mimickers. AJR Am J Roentgenol. 2016; 206:952–962.
Article14. Ryu YJ, Choi YH, Cheon JE, Kim WS, Kim IO, Park JE, et al. Imaging findings of kaposiform hemangioendothelioma in children. Eur J Radiol. 2017; 86:198–205.
Article15. White CL, Olivieri B, Restrepo R, McKeon B, Karakas SP, Lee EY. Low-flow vascular malformation pitfalls: from clinical examination to practical imaging evaluation—Part 1, lymphatic malformation mimickers. AJR Am J Roentgenol. 2016; 206:940–951.
Article16. Fishman SJ, Mulliken JB. Hemangiomas and vascular malformations of infancy and childhood. Pediatr Clin North Am. 1993; 40:1177–1200.
Article17. Johnson CM, Navarro OM. Clinical and sonographic features of pediatric soft-tissue vascular anomalies part 2: vascular malformations. Pediatr Radiol. 2017; 47:1196–1208.
Article18. Legiehn GM, Heran MK. Venous malformations: classification, development, diagnosis, and interventional radiologic management. Radiol Clin North Am. 2008; 46:545–597. vi
Article19. Flors L, Leiva-Salinas C, Maged IM, Norton PT, Matsumoto AH, Angle JF, et al. MR imaging of soft-tissue vascular malformations: diagnosis, classification, and therapy follow-up. Radiographics. 2011; 31:1321–1340. discussion 1340-1341.
Article20. Wassef M, Blei F, Adams D, Alomari A, Baselga E, Berenstein A, et al. ISSVA Board and Scientific Committee. Vascular anomalies classification: recommendations from the International Society for the Study of Vascular Anomalies. Pediatrics. 2015; 136:e203–e214.
Article21. Sheybani EF, Eutsler EP, Navarro OM. Fat-containing soft-tissue masses in children. Pediatr Radiol. 2016; 46:1760–1773.
Article22. Navarro OM, Laffan EE, Ngan BY. Pediatric soft-tissue tumors and pseudo-tumors: MR imaging features with pathologic correlation: part 1. Imaging approach, pseudotumors, vascular lesions, and adipocytic tumors. Radiographics. 2009; 29:887–906.23. Susam-Sen H, Yalcin B, Kutluk T, Cahit Tanyel F, Haliloglu M, Orhan D, et al. Lipoblastoma in children: review of 12 cases. Pediatr Int. 2017; 59:545–550.24. Han JW, Kim H, Youn JK, Oh C, Jung SE, Park KW, et al. Analysis of clinical features of lipoblastoma in children. Pediatr Hematol Oncol. 2017; 34:212–220.
Article25. Gupta P, Potti TA, Wuertzer SD, Lenchik L, Pacholke DA. Spectrum of fat-containing soft-tissue masses at MR imaging: the common, the uncommon, the characteristic, and the sometimes confusing. Radiographics. 2016; 36:753–766.
Article26. Szpecht D, Bagnosz-Magnuszewska A, Szymankiewicz M, Gadzinowski J. Subcutaneous fat necrosis in neonates after therapeutic hypothermia - report of two cases. Postepy Dermatol Alergol. 2016; 33:152–154.
Article27. Vasireddy S, Long SD, Sacheti B, Mayforth RD. MRI and US findings of subcutaneous fat necrosis of the newborn. Pediatr Radiol. 2009; 39:73–76.
Article28. Lee KJ, Jin W, Kim GY, Rhee SJ, Park SY, Park JS, et al. Sonographic features of superficial-type nodular fasciitis in the musculoskeletal system. J Ultrasound Med. 2015; 34:1465–1471.
Article29. Khuu A, Yablon CM, Jacobson JA, Inyang A, Lucas DR, Biermann JS. Nodular fasciitis: characteristic imaging features on sonography and magnetic resonance imaging. J Ultrasound Med. 2014; 33:565–573.30. Naidu A, Lerman MA. Clinical pathologic conference case 3: nodular fasciitis. Head Neck Pathol. 2011; 5:276–280.
Article31. Lee S, Choi YH, Cheon JE, Kim MJ, Lee MJ, Koh MJ. Ultrasonographic features of fibrous hamartoma of infancy. Skeletal Radiol. 2014; 43:649–653.
Article32. Chung EB, Enzinger FM. Infantile myofibromatosis. Cancer. 1981; 48:1807–1818.
Article33. Sargar KM, Sheybani EF, Shenoy A, Aranake-Chrisinger J, Khanna G. Pediatric fibroblastic and myofibroblastic tumors: a pictorial review. Radiographics. 2016; 36:1195–1214.
Article34. Gruber H, Glodny B, Bendix N, Tzankov A, Peer S. High-resolution ultrasound of peripheral neurogenic tumors. Eur Radiol. 2007; 17:2880–2888.
Article35. Reynolds DL Jr, Jacobson JA, Inampudi P, Jamadar DA, Ebrahim FS, Hayes CW. Sonographic characteristics of peripheral nerve sheath tumors. AJR Am J Roentgenol. 2004; 182:741–744.
Article36. Gosein M, Ameeral A, Banfield R, Mosodeen M. Plexiform neurofibroma of the wrist: imaging features and when to suspect malignancy. Case Rep Radiol. 2013; 2013:493752.
Article37. Quinn TJ, Jacobson JA, Craig JG, van Holsbeeck MT. Sonography of Morton's neuromas. AJR Am J Roentgenol. 2000; 174:1723–1728.
Article38. Wasa J, Nishida Y, Tsukushi S, Shido Y, Sugiura H, Nakashima H, et al. MRI features in the differentiation of malignant peripheral nerve sheath tumors and neurofibromas. AJR Am J Roentgenol. 2010; 194:1568–1574.
Article39. Bhargava R, Parham DM, Lasater OE, Chari RS, Chen G, Fletcher BD. MR imaging differentiation of benign and malignant peripheral nerve sheath tumors: use of the target sign. Pediatr Radiol. 1997; 27:124–129.
Article40. Bensaid B, Giammarile F, Mognetti T, Galoisy-Guibal L, Pinson S, Drouet A, et al. [Utility of 18 FDG positon emission tomography in detection of sarcomatous transformation in neurofibromatosis type 1]. Ann Dermatol Venereol. 2007; 134(10 Pt 1):735–741.41. Wagner JM, Rebik K, Spicer PJ. Ultrasound of soft tissue masses and fluid collections. Radiol Clin North Am. 2019; 57:657–669.
Article42. Kim HK, Kim SM, Lee SH, Racadio JM, Shin MJ. Subcutaneous epidermal inclusion cysts: ultrasound (US) and MR imaging findings. Skeletal Radiol. 2011; 40:1415–1419.
Article43. Yuan WH, Hsu HC, Lai YC, Chou YH, Li AF. Differences in sonographic features of ruptured and unruptured epidermal cysts. J Ultrasound Med. 2012; 31:265–272.
Article44. Hwang JY, Lee SW, Lee SM. The common ultrasonographic features of pilomatricoma. J Ultrasound Med. 2005; 24:1397–1402.
Article45. Eutsler EP, Siegel MJ. Musculoskeletal system and vascular imaging. In : Siegel MJ, editor. Pediatric sonography. 5th ed. Philadelphia, PA: Wolters Kluwer;2018. p. 627.46. Teefey SA, Dahiya N, Middleton WD, Gelberman RH, Boyer MI. Ganglia of the hand and wrist: a sonographic analysis. AJR Am J Roentgenol. 2008; 191:716–720.
Article47. Wang G, Jacobson JA, Feng FY, Girish G, Caoili EM, Brandon C. Sonography of wrist ganglion cysts: variable and noncystic appearances. J Ultrasound Med. 2007; 26:1323–1328. quiz 1330–1331.48. Van Rijn RR, Wilde JC, Bras J, Oldenburger F, McHugh KM, Merks JH. Imaging findings in noncraniofacial childhood rhabdomyosarcoma. Pediatr Radiol. 2008; 38:617–634.
Article49. Miller RW, Young JL Jr, Novakovic B. Childhood cancer. Cancer. 1995; 75:1 Suppl. 395–405.
Article50. Bakri A, Shinagare AB, Krajewski KM, Howard SA, Jagannathan JP, Hornick JL, et al. Synovial sarcoma: imaging features of common and uncommon primary sites, metastatic patterns, and treatment response. AJR Am J Roentgenol. 2012; 199:W208–W215.
Article51. Murphey MD, Gibson MS, Jennings BT, Crespo-Rodríguez AM, Fanburg-Smith J, Gajewski DA. From the archives of the AFIP: imaging of synovial sarcoma with radiologic-pathologic correlation. Radiographics. 2006; 26:1543–1565.52. Kang BS, Choi SH, Cha HJ, Jung YK, Lee JH, Jeong AK, et al. Subcutaneous panniculitis-like T-cell lymphoma: US and CT findings in three patients. Skeletal Radiol. 2007; 36 Suppl 1:S67–S71.
Article53. Bakst RL, Tallman MS, Douer D, Yahalom J. How I treat extramedullary acute myeloid leukemia. Blood. 2011; 118:3785–3793.
Article54. Isaacs H Jr. Cutaneous metastases in neonates: a review. Pediatr Dermatol. 2011; 28:85–93.
Article55. Hanna SL, Kaste S, Jenkins JJ, Hewan-Lowe K, Spence JV, Gupta M, et al. Epithelioid sarcoma: clinical, MR imaging and pathologic findings. Skeletal Radiol. 2002; 31:400–412.56. Giovagnorio F, Valentini C, Paonessa A. High-resolution and color doppler sonography in the evaluation of skin metastases. J Ultrasound Med. 2003; 22:1017–1022. quiz 1023–1025.
Article57. Sood S, Baheti AD, Shinagare AB, Jagannathan JP, Hornick JL, Ramaiya NH, et al. Imaging features of primary and metastatic alveolar soft part sarcoma: single institute experience in 25 patients. Br J Radiol. 2014; 87:20130719.
Article58. Chung HW, Cho KH. Ultrasonography of soft tissue “oops lesions”. Ultrasonography. 2015; 34:217–225.
Article59. Calleja M, Dimigen M, Saifuddin A. MRI of superficial soft tissue masses: analysis of features useful in distinguishing between benign and malignant lesions. Skeletal Radiol. 2012; 41:1517–1524.
Article
