Prevalence of Low Bone Mineral Density and Associated Risk Factors in Korean Puerperal Women
- Affiliations
-
- 1Department of Obstetrics and Gynecology, The Catholic University of Korea, Seoul, Korea. ooooobbbbb@catholic.ac.kr
- KMID: 2470276
- DOI: http://doi.org/10.3346/jkms.2016.31.11.1790
Abstract
- Although pregnancy is a medical condition that contributes to bone loss, little information is available regarding bone mineral density (BMD) in puerperal women. This cross sectional study aimed to evaluate the prevalence of low BMD in puerperal women and to identify associated risk factors. We surveyed all puerperal women who had BMD measurements taken 4-6 weeks after delivery in a tertiary university hospital, and did not have any bone loss-related comorbidities. Among the 1,561 Korean puerperal women, 566 (36.3%) had low BMD at the lumbar spine, total hip, femoral neck, and/or trochanter. Multivariate analysis revealed that underweight women had a significantly higher risk of low BMD compared with obese women at pre-pregnancy (adjusted odds ratio [aOR], 3.21; 95% confidence interval [CI], 1.83-5.63). Also, women with inadequate gestational weight gain (GWG) were 1.4 times more likely to have low BMD than women with excessive GWG (aOR, 1.42; 95% CI, 1.04-1.94). One-way ANOVA showed that BMDs at the lumbar spine and total hip were significantly different between the 4 BMI groups (both P < 0.001) and also between the 3 GWG groups (both P < 0.001). In conclusion, this study identifies a high prevalence of low BMD in puerperal women and thus suggests the need for further evaluation about the change of BMD in pregnancy and postpartum period.
MeSH Terms
Figure
-
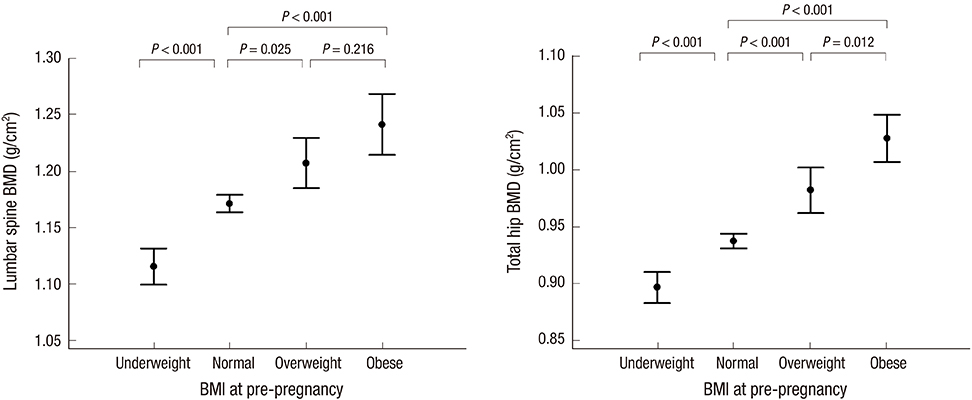
Fig. 1 Mean bone mineral densities (BMDs) at the lumbar spine and total hip in the 4 body mass index (BMI) groups. Data are presented as means; vertical bars show the 95% confidence intervals. At both sites, the BMD tended to increase as the BMI increased (both P < 0.001, ANOVA test). Post hoc analysis revealed significant differences in BMD at the lumbar spine and total hip between the different BMI groups (all P < 0.05), with the exception of BMD at the lumbar spine in the overweight versus obese groups (P = 0.216).
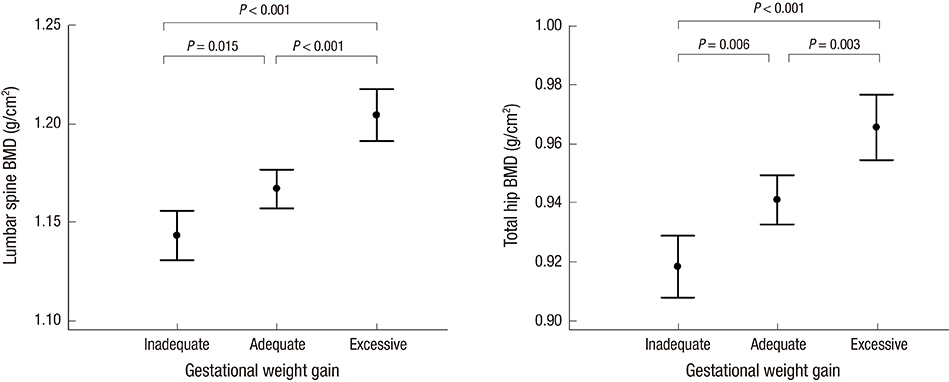
Fig. 2 Mean bone mineral densities (BMDs) at the lumbar spine and hip in the 3 gestational weight gain (GWG) groups. Data are presented as means; vertical bars show the 95% confidence intervals. At both sites, the BMD tended to increase as the GWG increased (both P < 0.001, ANOVA test). Post hoc analysis revealed significant differences in BMD at both sites between the different GWG groups (all P < 0.05).
Reference
-
1. Sambrook P, Cooper C. Osteoporosis. Lancet. 2006; 367:2010–2018.2. Berger C, Goltzman D, Langsetmo L, Joseph L, Jackson S, Kreiger N, Tenenhouse A, Davison KS, Josse RG, Prior JC, et al. Peak bone mass from longitudinal data: implications for the prevalence, pathophysiology, and diagnosis of osteoporosis. J Bone Miner Res. 2010; 25:1948–1957.3. Kovacs CS. Calcium and bone metabolism during pregnancy and lactation. J Mammary Gland Biol Neoplasia. 2005; 10:105–118.4. Ward KA, Adams JE, Mughal MZ. Bone status during adolescence, pregnancy and lactation. Curr Opin Obstet Gynecol. 2005; 17:435–439.5. Hellmeyer L, Ziller V, Anderer G, Ossendorf A, Schmidt S, Hadji P. Biochemical markers of bone turnover during pregnancy: a longitudinal study. Exp Clin Endocrinol Diabetes. 2006; 114:506–510.6. More C, Bettembuk P, Bhattoa HP, Balogh A. The effects of pregnancy and lactation on bone mineral density. Osteoporos Int. 2001; 12:732–737.7. Black AJ, Topping J, Durham B, Farquharson RG, Fraser WD. A detailed assessment of alterations in bone turnover, calcium homeostasis, and bone density in normal pregnancy. J Bone Miner Res. 2000; 15:557–563.8. Kaur M, Pearson D, Godber I, Lawson N, Baker P, Hosking D. Longitudinal changes in bone mineral density during normal pregnancy. Bone. 2003; 32:449–454.9. Yamaga A, Taga M, Minaguchi H, Sato K. Changes in bone mass as determined by ultrasound and biochemical markers of bone turnover during pregnancy and puerperium: a longitudinal study. J Clin Endocrinol Metab. 1996; 81:752–756.10. To WW, Wong MW, Leung TW. Relationship between bone mineral density changes in pregnancy and maternal and pregnancy characteristics: a longitudinal study. Acta Obstet Gynecol Scand. 2003; 82:820–827.11. Hellmeyer L, Hahn B, Fischer C, Hars O, Boekhoff J, Maier J, Hadji P. Quantitative ultrasonometry during pregnancy and lactation: a longitudinal study. Osteoporos Int. 2015; 26:1147–1154.12. World Health Organization Western Pacific Region. International Association for the Study of Obesity. International Obesity Task Force. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment. Sydney: Health Communications Australia Pty Limited;2000.13. Institute of Medicine, National Research Council, Committee to Reexamine IOM Pregnancy Weight Guidelines (US). Weight Gain during Pregnancy: Reexamining the Guidelines. Washington, D.C.: National Academies Press;2009.14. National Osteoporosis Foundation (US). Clinician's Guide to Prevention and Treatment of Osteoporosis. Washington, D.C.: National Osteoporosis Foundation;2008.15. Martínez-Morillo M, Grados D, Holgado S. Premenopausal osteoporosis: how to treat? Reumatol Clin. 2012; 8:93–97.16. Bhalla AK. Management of osteoporosis in a pre-menopausal woman. Best Pract Res Clin Rheumatol. 2010; 24:313–327.17. Coin A, Sergi G, Benincà P, Lupoli L, Cinti G, Ferrara L, Benedetti G, Tomasi G, Pisent C, Enzi G. Bone mineral density and body composition in underweight and normal elderly subjects. Osteoporos Int. 2000; 11:1043–1050.18. Tanaka S, Kuroda T, Saito M, Shiraki M. Overweight/obesity and underweight are both risk factors for osteoporotic fractures at different sites in Japanese postmenopausal women. Osteoporos Int. 2013; 24:69–76.19. Zhao LJ, Jiang H, Papasian CJ, Maulik D, Drees B, Hamilton J, Deng HW. Correlation of obesity and osteoporosis: effect of fat mass on the determination of osteoporosis. J Bone Miner Res. 2008; 23:17–29.20. Cao JJ. Effects of obesity on bone metabolism. J Orthop Surg. 2011; 6:30.21. Zhu K, Hunter M, James A, Lim EM, Cooke BR, Walsh JP. Discordance between fat mass index and body mass index is associated with reduced bone mineral density in women but not in men: the Busselton healthy ageing study. Osteoporos Int. Forthcoming. 2016.22. Ettinger AS, Lamadrid-Figueroa H, Mercado-García A, Kordas K, Wood RJ, Peterson KE, Hu H, Hernández-Avila M, Téllez-Rojo MM. Effect of calcium supplementation on bone resorption in pregnancy and the early postpartum: a randomized controlled trial in Mexican women. Nutr J. 2014; 13:116.23. Janakiraman V, Ettinger A, Mercado-Garcia A, Hu H, Hernandez-Avila M. Calcium supplements and bone resorption in pregnancy: a randomized crossover trial. Am J Prev Med. 2003; 24:260–264.24. Organisation for Economic Co-operation and Development. Obesity and the economics of prevention: fit not fat (key facts ??Korea, update 2012) [Internet]. accessed on 21 February 2012. Availabe at http://www.oecd.org/els/health-systems/49712651.pdf.25. Park SY, Paik HY, Skinner JD, Spindler AA, Park HR. Nutrient intake of Korean-American, Korean, and American adolescents. J Am Diet Assoc. 2004; 104:242–245.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dermographism ( II ) : The Prevalence in Korean Pregnant and Puerperal Women
- A Statistical Analysis of Risk Factors for Osteoporosis in Menopausal Women
- Association of the Metabolic Syndrome and Bone Mineral Density in Postmenopausal Women
- Prevalence of Osteoporosis Based on Bone Density Measurement in Korean Women
- The relationship of maturation value of vaginal epithelium and bone mineral density in postmenopausal women
