Diagnostic Accuracy of a Novel On-site Virtual Fractional Flow Reserve Parallel Computing System
- Affiliations
-
- 1Connect-AI Research Center, Yonsei University College of Medicine, Seoul, Korea.
- 2Department of Cardiology, International St. Mary's Hospital, Catholic Kwandong University College of Medicine, Incheon, Korea.
- 3Mayo Clinic, Division of Cardiology, Department of Internal Medicine, Scottsdale, AZ, USA.
- 4School of Mechanical Engineering, University of Ulsan, Ulsan, Korea. leesw@ulsan.ac.kr
- 5Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University Health System, Seoul, Korea.
- KMID: 2468488
- DOI: http://doi.org/10.3349/ymj.2020.61.2.137
Abstract
- PURPOSE
To evaluate the diagnostic accuracy of a novel on-site virtual fractional flow reserve (vFFR) derived from coronary computed tomography angiography (CTA).
MATERIALS AND METHODS
We analyzed 100 vessels from 57 patients who had undergone CTA followed by invasive FFR during coronary angiography. Coronary lumen segmentation and three-dimensional reconstruction were conducted using a completely automated algorithm, and parallel computing based vFFR prediction was performed. Lesion-specific ischemia based on FFR was defined as significant at ≤0.8, as well as ≤0.75, and obstructive CTA stenosis was defined that ≥50%. The diagnostic performance of vFFR was compared to invasive FFR at both ≤0.8 and ≤0.75.
RESULTS
The average computation time was 12 minutes per patient. The correlation coefficient (r) between vFFR and invasive FFR was 0.75 [95% confidence interval (CI) 0.65 to 0.83], and Bland-Altman analysis showed a mean bias of 0.005 (95% CI −0.011 to 0.021) with 95% limits of agreement of −0.16 to 0.17 between vFFR and FFR. The accuracy, sensitivity, specificity, positive predictive value, and negative predictive value were 78.0%, 87.1%, 72.5%, 58.7%, and 92.6%, respectively, using the FFR cutoff of 0.80. They were 87.0%, 95.0%, 80.0%, 54.3%, and 98.5%, respectively, with the FFR cutoff of 0.75. The area under the receiver-operating characteristics curve of vFFR versus obstructive CTA stenosis was 0.88 versus 0.61 for the FFR cutoff of 0.80, respectively; it was 0.94 versus 0.62 for the FFR cutoff of 0.75.
CONCLUSION
Our novel, fully automated, on-site vFFR technology showed excellent diagnostic performance for the detection of lesion-specific ischemia.
Keyword
MeSH Terms
Figure
-

Fig. 1 Workflow of the automated segmentation algorithm and the novel parallel computing method. (A) A fully automated lumen segmentation algorithm was applied to reconstruct patient-specific coronary geometry. (B) A novel parallel computing procedure based on a cluster with 40 cores decomposing the domain into 40 sub-domains and assigning a sub-domain to each computing core was applied.
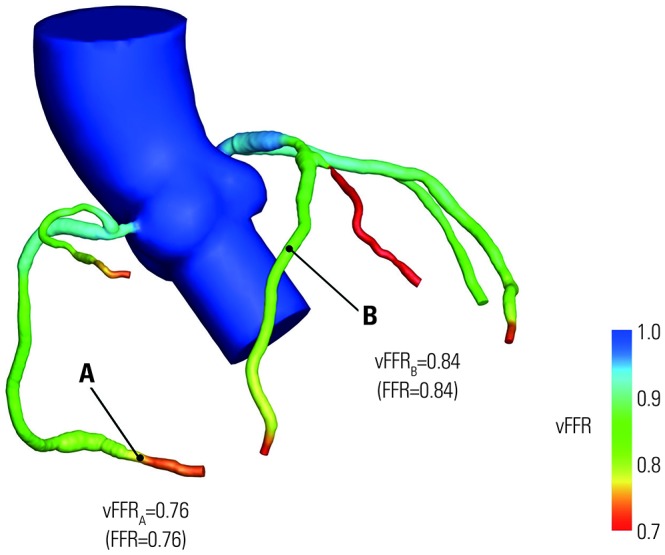
Fig. 2 Example simulation case of on-site virtual fractional flow reserve (vFFR). A noninvasive on-site vFFR simulation defined the distal portion of the right coronary artery (A) as an ischemic lesion (0.76) and the middle portion of the left anterior descending artery (B) as a non-ischemic lesion (0.84). These simulation derived values matched perfectly with the invasively measured FFR values.

Fig. 3 Linear regression (A) and Bland-Altman analysis (B) between vFFR and FFR. Correlation coefficient (r) between vFFR and FFR was 0.75 (95% CI 0.65 to 0.83), and Bland-Altman analysis showed a mean bias of 0.005 (95% CI −0.011 to 0.021), with 95% limits of agreement of −0.16 to 0.17. vFFR, virtual fractional flow reserve; CI, confidence interval.
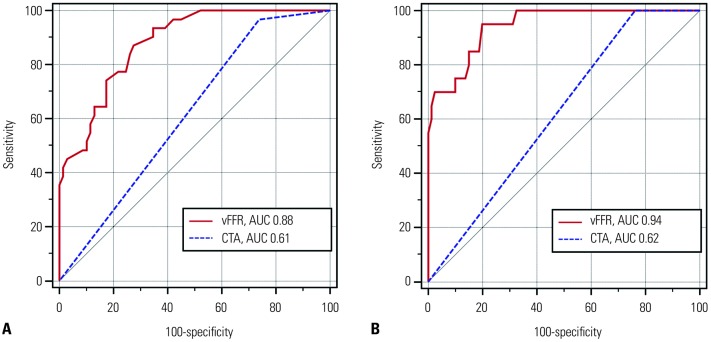
Fig. 4 ROC demonstrating AUCs for vFFR and obstructive (≥50%) CTA stenosis for the discrimination of lesion-specific ischemia using FFR cutoff values of 0.8 and 0.75. (A) The AUC for vFFR was significantly higher (0.88, 95% CI 0.80–0.94) than CTA ≥50% stenosis (0.61, 95% CI 0.51–0.71) when an FFR cutoff of 0.8 was used. (B) The AUC value for vFFR was excellent (0.94, 95% CI 0.88–0.98), compared to the CTA ≥50% stenosis (0.62, 95% CI 0.52–0.71), when an FFR cutoff of 0.75 was used. ROC, receiver operating characteristic curve; AUC, areas under receiver operating characteristic curve; vFFR, virtual fractional flow reserve; CTA, com-puted tomography angiography; CI, confidence interval.
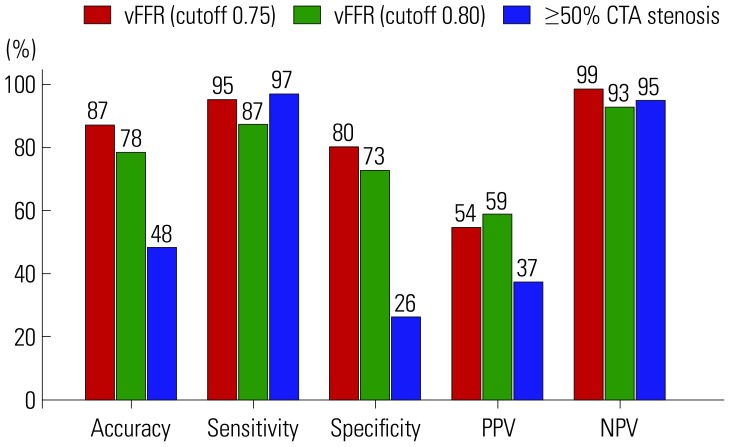
Fig. 5 Diagnostic performance of vFFR using a cutoff of 0.75 (red), vFFR using a cutoff of 0.8 (green), and obstructive (≥50%) CTA stenosis (blue) for lesion-specific ischemia detection. vFFR, virtual fractional flow reserve; CTA, computed tomography angiography.
Reference
-
1. Tonino PA, De Bruyne B, Pijls NH, Siebert U, Ikeno F, van' t Veer M, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009; 360:213–224. PMID: 19144937.
Article2. Pijls NH, Fearon WF, Tonino PA, Siebert U, Ikeno F, Bornschein B, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention in patients with multivessel coronary artery disease: 2-year follow-up of the FAME (Fractional Flow Reserve Versus Angiography for Multivessel Evaluation) study. J Am Coll Cardiol. 2010; 56:177–184. PMID: 20537493.3. De Bruyne B, Pijls NH, Kalesan B, Barbato E, Tonino PA, Piroth Z, et al. Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease. N Engl J Med. 2012; 367:991–1001. PMID: 22924638.
Article4. Budoff MJ, Dowe D, Jollis JG, Gitter M, Sutherland J, Halamert E, et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol. 2008; 52:1724–1732. PMID: 19007693.5. Miller JM, Rochitte CE, Dewey M, Arbab-Zadeh A, Niinuma H, Gottlieb I, et al. Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med. 2008; 359:2324–2336. PMID: 19038879.
Article6. Meijboom WB, Meijs MF, Schuijf JD, Cramer MJ, Mollet NR, van Mieghem CA, et al. Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol. 2008; 52:2135–2144. PMID: 19095130.7. Dewey M, Rief M, Martus P, Kendziora B, Feger S, Dreger H, et al. Evaluation of computed tomography in patients with atypical angina or chest pain clinically referred for invasive coronary angiography: randomised controlled trial. BMJ. 2016; 355:i5441. PMID: 27777234.
Article8. Raff GL, Gallagher MJ, O'Neill WW, Goldstein JA. Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol. 2005; 46:552–557. PMID: 16053973.
Article9. Leber AW, Knez A, von Ziegler F, Becker A, Nikolaou K, Paul S, et al. Quantification of obstructive and nonobstructive coronary lesions by 64-slice computed tomography: a comparative study with quantitative coronary angiography and intravascular ultrasound. J Am Coll Cardiol. 2005; 46:147–154. PMID: 15992649.10. Koo BK, Erglis A, Doh JH, Daniels DV, Jegere S, Kim HS, et al. Diagnosis of ischemia-causing coronary stenoses by noninvasive fractional flow reserve computed from coronary computed tomographic angiograms. Results from the prospective multicenter DISCOVER-FLOW (Diagnosis of Ischemia-Causing Stenoses Obtained Via Noninvasive Fractional Flow Reserve) study. J Am Coll Cardiol. 2011; 58:1989–1997. PMID: 22032711.11. Min JK, Leipsic J, Pencina MJ, Berman DS, Koo BK, van Mieghem C, et al. Diagnostic accuracy of fractional flow reserve from anatomic CT angiography. JAMA. 2012; 308:1237–1245. PMID: 22922562.
Article12. Nørgaard BL, Leipsic J, Gaur S, Seneviratne S, Ko BS, Ito H, et al. Diagnostic performance of noninvasive fractional flow reserve derived from coronary computed tomography angiography in suspected coronary artery disease: the NXT trial (analysis of coronary blood flow using CT angiography: next steps). J Am Coll Cardiol. 2014; 63:1145–1155. PMID: 24486266.13. Ding A, Qiu G, Lin W, Hu L, Lu G, Long X, et al. Diagnostic performance of noninvasive fractional flow reserve derived from coronary computed tomography angiography in ischemia-causing coronary stenosis: a meta-analysis. Jpn J Radiol. 2016; 34:795–808. PMID: 27796727.
Article14. Min JK, Taylor CA, Achenbach S, Koo BK, Leipsic J, Nørgaard BL, et al. Noninvasive fractional flow reserve derived from coronary CT angiography: clinical data and scientific principles. JACC Cardiovasc Imaging. 2015; 8:1209–1222. PMID: 26481846.15. Kimura T, Shiomi H, Kuribayashi S, Isshiki T, Kanazawa S, Ito H, et al. Cost analysis of non-invasive fractional flow reserve derived from coronary computed tomographic angiography in Japan. Cardiovasc Interv Ther. 2015; 30:38–44. PMID: 25030180.
Article16. Douglas PS, De Bruyne B, Pontone G, Patel MR, Norgaard BL, Byrne RA, et al. 1-year outcomes of FFRCT-guided care in patients with suspected coronary disease: the PLATFORM study. J Am Coll Cardiol. 2016; 68:435–445. PMID: 27470449.17. Rajani R, Modi B, Ntalas I, Curzen N. Non-invasive fractional flow reserve using computed tomographic angiography: where are we now and where are we going? Heart. 2017; 103:1216–1222. PMID: 28559426.
Article18. Otake H, Taylor CA, Matsuo H, Tanaka N, Akasaka T. Noninvasive fractional flow reserve derived from coronary computed tomography angiography-is this just another new diagnostic test or the long-awaited game changer? Circ J. 2017; 81:1085–1093. PMID: 28413187.19. Jeon B, Hong Y, Han D, Jang Y, Jung S, Hong Y, et al. Maximum a posteriori estimation method for aorta localization and coronary seed identification. Pattern Recognition. 2017; 68:222–232.
Article20. Han D, Shim H, Jeon B, Jang Y, Hong Y, Jung S, et al. Automatic coronary artery segmentation using active search for branches and seemingly disconnected vessel segments from coronary CT angiography. PLoS One. 2016; 11:e0156837. PMID: 27536939.
Article21. Jang Y, Kim DH, Jeon B, Han D, Shim H, Chang HJ. Generation of triangular mesh of coronary artery using mesh merging. Journal of KIISE. 2016; 43:419–429.
Article22. Sankaran S, Esmaily Moghadam M, Kahn AM, Tseng EE, Guccione JM, Marsden AL. Patient-specific multiscale modeling of blood flow for coronary artery bypass graft surgery. Ann Biomed Eng. 2012; 40:2228–2242. PMID: 22539149.
Article23. Sharma P, Itu L, Zheng X, Kamen A, Bernhardt D, Suciu C, et al. A framework for personalization of coronary flow computations during rest and hyperemia. Conf Proc IEEE Eng Med Biol Soc. 2012; 2012:6665–6668. PMID: 23367458.
Article24. Murray CD. The physiological principle of minimum work: I. The vascular system and the cost of blood volume. Proc Natl Acad Sci U S A. 1926; 12:207–214. PMID: 16576980.
Article25. Nguyen MT, Jeon BJ, Chang HJ, Lee SW. Domain decomposition based parallel computing for multi-scale coronary blood flow simulations. Computers & Fluids. 2019; 191:104254.
Article26. Karypis G, Kumar V. A fast and high quality multilevel scheme for partitioning irregular graphs. SIAM J Sci Comput. 1998; 20:359–392.
Article27. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988; 44:837–845. PMID: 3203132.
Article28. Nørgaard BL, Jensen JM, Leipsic J. Fractional flow reserve derived from coronary CT angiography in stable coronary disease: a new standard in non-invasive testing? Eur Radiol. 2015; 25:2282–2290. PMID: 25680721.
Article29. Renker M, Schoepf UJ, Wang R, Meinel FG, Rier JD, Bayer RR 2nd, et al. Comparison of diagnostic value of a novel noninvasive coronary computed tomography angiography method versus standard coronary angiography for assessing fractional flow reserve. Am J Cardiol. 2014; 114:1303–1308. PMID: 25205628.
Article30. Yang DH, Kim YH, Roh JH, Kang JW, Ahn JM, Kweon J, et al. Diagnostic performance of on-site CT-derived fractional flow reserve versus CT perfusion. Eur Heart J Cardiovasc Imaging. 2017; 18:432–440. PMID: 27354345.
Article31. Motoyama S, Kondo T, Sarai M, Sugiura A, Harigaya H, Sato T, et al. Multislice computed tomographic characteristics of coronary lesions in acute coronary syndromes. J Am Coll Cardiol. 2007; 50:319–326. PMID: 17659199.
Article32. Motoyama S, Sarai M, Harigaya H, Anno H, Inoue K, Hara T, et al. Computed tomographic angiography characteristics of atherosclerotic plaques subsequently resulting in acute coronary syndrome. J Am Coll Cardiol. 2009; 54:49–57. PMID: 19555840.
Article33. Motoyama S, Ito H, Sarai M, Kondo T, Kawai H, Nagahara Y, et al. Plaque characterization by coronary computed tomography angiography and the likelihood of acute coronary events in mid-term follow-up. J Am Coll Cardiol. 2015; 66:337–346. PMID: 26205589.34. Park HB, Heo R, Ó Hartaigh B, Cho I, Gransar H, Nakazato R, et al. Atherosclerotic plaque characteristics by CT angiography identify coronary lesions that cause ischemia: a direct comparison to fractional flow reserve. JACC Cardiovasc Imaging. 2015; 8:1–10. PMID: 25592691.35. Nakazato R, Park HB, Gransar H, Leipsic JA, Budoff MJ, Mancini GB, et al. Additive diagnostic value of atherosclerotic plaque characteristics to non-invasive FFR for identification of lesions causing ischaemia: results from a prospective international multicentre trial. EuroIntervention. 2016; 12:473–481. PMID: 26348673.
Article36. Gaur S, Øvrehus KA, Dey D, Leipsic J, Bøtker HE, Jensen JM, et al. Coronary plaque quantification and fractional flow reserve by coronary computed tomography angiography identify ischaemia-causing lesions. Eur Heart J. 2016; 37:1220–1227. PMID: 26763790.
Article37. Leipsic J, Yang TH, Thompson A, Koo BK, Mancini GB, Taylor C, et al. CT angiography (CTA) and diagnostic performance of noninvasive fractional flow reserve: results from the Determination of Fractional Flow Reserve by Anatomic CTA (DeFACTO) study. AJR Am J Roentgenol. 2014; 202:989–994. PMID: 24758651.
Article38. Nørgaard BL, Gaur S, Leipsic J, Ito H, Miyoshi T, Park SJ, et al. Influence of coronary calcification on the diagnostic performance of CT angiography derived FFR in coronary artery disease: a substudy of the NXT trial. JACC Cardiovasc Imaging. 2015; 8:1045–1055. PMID: 26298072.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Myocardial fractional flow reserve in acute myocardial infarction
- Funtional significance of the intermediate lesion in a single coronary artery assessed by fractional flow reserve
- Physiologic Assessment of Coronary Artery Disease: Focus on Fractional Flow Reserve
- Diagnostic Performance of On-Site Automatic Coronary Computed Tomography Angiography-Derived Fractional Flow Reserve
- Fractional Flow Reserve: The Past, Present and Future
