Successful treatment of early acute antibody-mediated rejection in an human leukocyte antigen-incompatible and ABO-incompatible living-donor kidney transplant patient
- Affiliations
-
- 1Department of Surgery, Seoul National University Hospital, Seoul, Korea. jcyjs@snu.ac.kr
- 2Transplantation Center, Seoul National University Hospital, Seoul, Korea.
- 3Transplantation Research Institute, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2468166
- DOI: http://doi.org/10.4285/jkstn.2019.33.4.153
Abstract
- For successful human leukocyte antigen-incompatible (HLAi) or ABO-incompatible (ABOi) living-donor kidney transplantations (LDKTs), pretransplant desensitization is essential; however, early antibody-mediated rejection (ABMR) remains the most important complication after HLAi or ABOi transplantation. Here, we report a case of early acute ABMR in simultaneous HLAi and ABOi LDKT with preformed donor-specific antibody (DSA), despite desensitization. Dialysis-dependent, severe ABMR occurred with a rebound of pre-existing DSA and appearance of de novo DSA after initial normalization of renal function, 8 days postoperatively. However, a low anti-ABO antibody titer (1:8) was maintained after transplantation. Combination therapy of plasmapheresis, high-dose intravenous immunoglobulin, and bortezomib improved both ABMR and renal functions. Thus, an appropriate preventive and therapeutic management for early ABMR is important among high-risk LDKT patients. Furthermore, early AMBR can occur despite pretransplant desensitization as seen in this case, and close monitoring of the patient and prompt management are considered vital for better therapeutic outcomes.
MeSH Terms
Figure
-
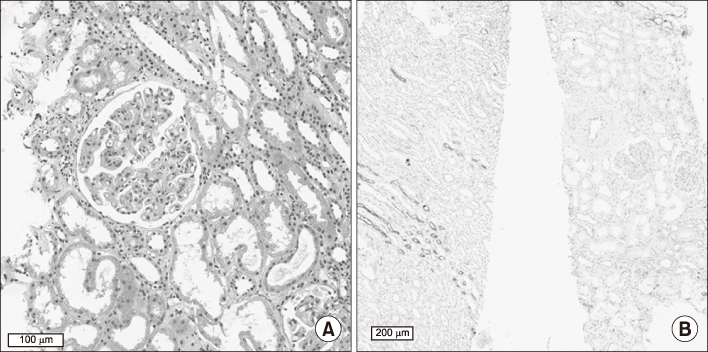
Fig. 1 Pathology of kidney biopsy on postoperative day 28 (POD28). Kidney biopsy on POD28 showed antibody-mediated rejection (ABMR) grade-II as per Banff classification 2017 (t0, i0, iIFTA0, g1, ptc1, v1, ci0, ct0, cg3, mm1, cv1, ah0, aah0, c4d2). According to Banff 2013 classification of acute ABMR in renal allografts, three criteria have to be met for diagnosing ABMR. For tissue injury compatible with ABMR, conditions include microvascular injury, intimal or transmural arteritis, acute thrombotic microangiopathy without other cause, and acute tubular injury without any other cause. Presence of donor-specific antibody (e.g., human leukocyte antigen-incompatible or other antigens) is needed for confirming ABMR. Evidence of their interaction with the vascular endothelium is needed, which include linear C4d staining of peritubular capillaries, at least moderate microvascular injury, and molecular markers [4]. (A) H&E, ×400. (B) Immunohistochemistry staining with peroxidase yielding a brown reaction product for C4d, ×100.
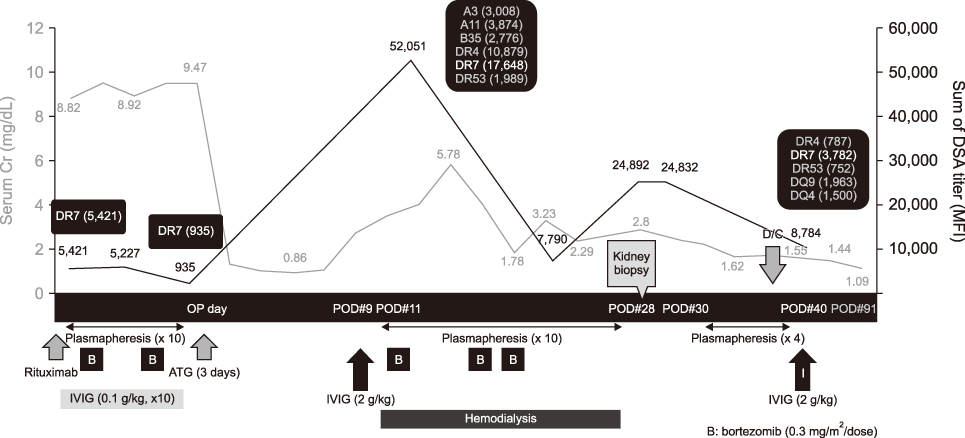
Fig. 2 Laboratory results and treatment over time. This figure shows treatments and changes in serum creatinine (Cr) level (mg/dL) and sum of donor-specific antibody (DSA; mean fluorescence intensity [MFI]) over a certain period. Immediately after transplantation, the serum Cr level decreased to near normal levels but increased on postoperative day 8 (POD8). DSA level was measured to evaluate such changes. The sum of serum DSA level increased and several de novo DSAs were newly discovered. After a combination of 14 therapeutic plasmapheresis sessions, steroid pulse therapy, high-dose intravenous immunoglobulin, and bortezomib administration, the sum of DSA and serum Cr level decreased. Decreased renal function was supported by hemodialysis. Kidney Doppler ultrasound examination showed an increase in resistance index (0.81–0.89). Antibody-mediated rejection (ABMR) was confirmed with biopsy on POD28. OP, operation; ATG, antithymocyte globulin; IVIG, intravenous immunoglobulin.
Cited by 1 articles
-
Clinical significance of de novo donor-specific antibody in kidney transplant recipients with chronic antibody-mediated rejection
Woo Yeong Park, Yaerim Kim, Jin Hyuk Paek, Kyubok Jin, Seungyeup Han
Korean J Transplant. 2021;35(1):33-40. doi: 10.4285/kjt.20.0052.
Reference
-
1. Davis S, Cooper JE. Acute antibody-mediated rejection in kidney transplant recipients. Transplant Rev (Orlando). 2017; 31:47–54.
Article2. Cardinal H, Dieudé M, Hébert MJ. The emerging importance of non-HLA autoantibodies in kidney transplant complications. J Am Soc Nephrol. 2017; 28:400–406.
Article3. Tasaki M, Saito K, Nakagawa Y, Tomita Y, Takahashi K. Ch12. ABO-incompatible kidney transplantation. In : Abdeldayem H, El-Kased AF, El-Shaarawy A, editors. Frontiers in transplantology. London, UK: Rijeka: InTech;2016. p. 285–300.4. Kwun J, Burghuber C, Manook M, Iwakoshi N, Gibby A, Hong JJ, et al. Humoral compensation after bortezomib treatment of allosensitized recipients. J Am Soc Nephrol. 2017; 28:1991–1996.
Article5. Haas M, Loupy A, Lefaucheur C, Roufosse C, Glotz D, Seron D, et al. The Banff 2017 Kidney Meeting Report: revised diagnostic criteria for chronic active T cell-mediated rejection, antibody-mediated rejection, and prospects for integrative endpoints for next-generation clinical trials. Am J Transplant. 2018; 18:293–307.
Article6. Kong JM, Ahn J, Park JB, Chung BH, Yang J, Kim JK, et al. ABO incompatible living donor kidney transplantation in Korea: highly uniform protocols and good medium-term outcome. Clin Transplant. 2013; 27:875–881.
Article7. Korean Organ Transplant Registry. KOTRY annual data report 2018 [Internet]. Seoul: Korean Organ Transplant Registry;2019. cited 2019 Dec 20. Available from: http://www.kotry.org/.8. Orandi BJ, Luo X, Massie AB, Garonzik-Wang JM, Lonze BE, Ahmed R, et al. Survival benefit with kidney transplants from HLA-incompatible live donors. N Engl J Med. 2016; 374:940–950.
Article9. Orandi BJ, Garonzik-Wang JM, Massie AB, Zachary AA, Montgomery JR, Van Arendonk KJ, et al. Quantifying the risk of incompatible kidney transplantation: a multicenter study. Am J Transplant. 2014; 14:1573–1580.
Article10. Orandi BJ, Chow EH, Hsu A, Gupta N, Van Arendonk KJ, Garonzik-Wang JM, et al. Quantifying renal allograft loss following early antibody-mediated rejection. Am J Transplant. 2015; 15:489–498.
Article11. Hart A, Smith JM, Skeans MA, Gustafson SK, Stewart DE, Cherikh WS, et al. OPTN/SRTR 2015 annual data report: kidney. Am J Transplant. 2017; 17 Suppl 1:21–116.
Article12. Schinstock C, Stegall MD. Acute antibody-mediated rejection in renal transplantation: current clinical management. Curr Transplant Rep. 2014; 1:78–85.
Article13. Woodle ES, Shields AR, Ejaz NS, Sadaka B, Girnita A, Walsh RC, et al. Prospective iterative trial of proteasome inhibitor-based desensitization. Am J Transplant. 2015; 15:101–118.
Article14. Haas M, Sis B, Racusen LC, Solez K, Glotz D, Colvin RB, et al. Banff 2013 meeting report: inclusion of c4d-negative antibody-mediated rejection and antibody-associated arterial lesions. Am J Transplant. 2014; 14:272–283.
Article15. Burghuber CK, Manook M, Ezekian B, Gibby AC, Leopardi FV, Song M, et al. Dual targeting: combining costimulation blockade and bortezomib to permit kidney transplantation in sensitized recipients. Am J Transplant. 2019; 19:724–736.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- ABO-Incompatible Living Donor Liver Transplantation
- Overcoming high pre-transplant isoagglutinin titers using high-dose intravenous immunoglobulin, salvage plasmapheresis, and booster rituximab without splenectomy in ABO-incompatible living donor liver transplantation: a case report
- Successful Pediatric ABO-Incompatible Kidney Transplantation without Pretransplant Plasmapheresis: Report of a Case
- The Diagnosis of Acute Antibody-Mediated Rejection in ABO-Incompatible Liver Transplants
- Effect of preexisting human leukocyte antigen donor-specific antibodies especially human leukocyte antigen-DQ on kidney transplant outcome
