High-resolution Imaging of Neural Anatomy and Pathology of the Neck
- Affiliations
-
- 1Department of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul 05505, Korea. jeonghlee@amc.seoul.kr
- 2Department of Medical Imaging, Chung Shan Medical University Hospital, Taichung 402, Taiwan.
- 3School of Medical Imaging and Radiological Sciences, Chung Shan Medical University, Taichung 402, Taiwan.
- 4Department of Veterinary Medicine, National Chung Hsing University, Taichung 402, Taiwan.
- KMID: 2468132
- DOI: http://doi.org/10.3348/kjr.2017.18.1.180
Abstract
- The neck has intricately connected neural structures, including cervical and brachial plexi, the sympathetic system, lower cranial nerves, and their branches. Except for brachial plexus, there has been little research regarding the normal imaging appearance or corresponding pathologies of neural structures in the neck. The development in imaging techniques with better spatial resolution and signal-to-noise ratio has made it possible to see many tiny nerves to predict complications related to image-guided procedures and to better assess treatment response, especially in the management of oncology patients. The purposes of this review is to present imaging-based anatomy of major nerves in the neck and explain their relevant clinical significance according to representative pathologies of regarded nerves in the neck.
Keyword
MeSH Terms
Figure
-

Fig. 1 Diagram of cervical sympathetic trunk (A) and brachial plexus (B). AS = ansa subclavia, AScM = anterior scalene muscle, C1–C8 = 1st to 8th cervical nerves, ICSG = inferior cervical sympathetic ganglion, ITA = inferior thyroid artery, LC = lateral cord, LCM = longus capitis muscle, LT = lower trunk, MC = middle cord, MCSG = middle cervical sympathetic ganglion, MPScM = middle and posterior scalene muscles, MT = middle trunk, PC = posterior cord, PhN = phrenic nerve, SCA = subclavian artery, SCSG = superior cervical sympathetic ganglion, UT = upper trunk, VA = vertebral artery, XII = hypoglossal nerve

Fig. 2 Normal MRI appearance of cervical sympathetic ganglia (CSGs). A-C. Coronal fat-suppressed (FS) T2-weighted image (T2WI) (A), axial contrast-enhanced fat-suppressed T1-weighted image (B), and axial T2WI (C) demonstrating typical locations and signal characteristics of superior (triple arrows on A), middle (single arrow on B), and inferior (double arrows on A and C) CSGs. Coronal FS T2WI (A) clearly shows that connecting nerve branches with superior CSG (dotted triple arrows) and inferior CSG (dotted double arrows). Note that middle CSG is located posterior to common carotid artery (empty arrow on B), anterior to vertebral artery (VA, short arrow on B), and lateral to longus colli muscle (arrowhead on B). Inferior CSG on either side is present as stellate ganglion lateral to longus colli muscle (arrowhead on C) and posteromedial to origin of VA (short arrows on C). Asterisk = subclavian artery, C2 = 2nd vertebra, C7 = 7th vertebra, dotted arrow = T1 nerve root, T1 = 1st thoracic vertebra
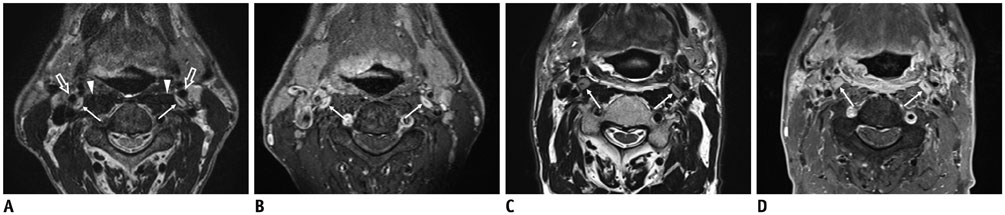
Fig. 3 60-year-old male with squamous cell carcinoma of right pyriform sinus (T3N1M0) after definitive concurrent chemoradiation therapy. Pretreatment (A, B) and post treatment (C, D) axial T2-weighted images (T2WIs) and contrast-enhanced fat-suppressed T1-weighted images (CE FS T1WIs) demonstrate homogeneously enhanced superior cervical sympathetic ganglia (CSG, thin arrows on A-D) on either side lateral to longus capitis muscle (arrowheads on A) and posterior to internal carotid artery (empty arrows on A). Note that there is typical intraganglionic hypointensity at center of superior CSGs both on T2WI and CE FS T1WI. Superior CSGs become enlarged in anterior to posterior dimensions along with diffuse radiation-induced change in retropharyngeal space, pharyngeal wall, and bilateral cervical level II.

Fig. 4 Schwannomas arising from cervical sympathetic ganglia (CSGs). Axial contrast-enhanced fat-suppressed T1-weighted images (A, B) and axial T2-weighted image (C) showing shwannomas arising from superior (thick arrow on A), middle (thick arrow on B), and inferior (thick arrow on C) CSGs. Masses arising from superior and middle CSGs typically displace internal carotid artery (empty arrow on A) or common carotid artery (empty arrow on B) to lateral side with internal jugular vein (arrowhead on A). Triple and double arrows on A and C showing normal superior and inferior CSGs, respectively.
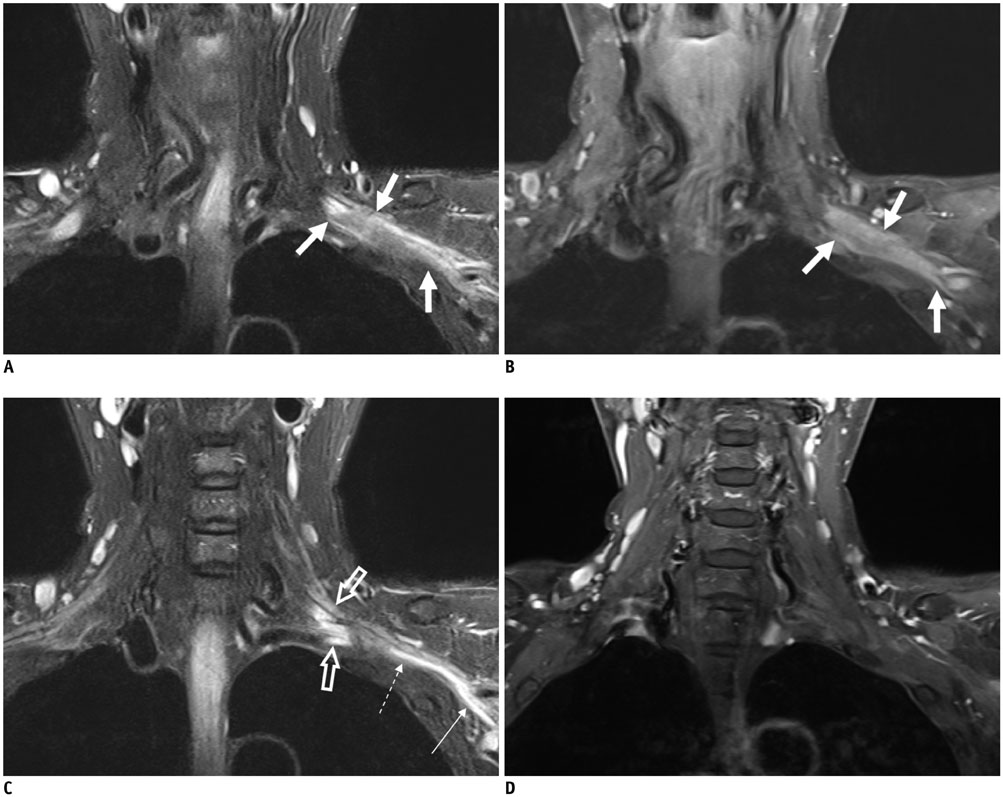
Fig. 5 58-year-old female with left breast cancer. Coronal fat-suppressed T2-weighted images (FS T2WIs) (A) and contrast-enhanced (CE) FS T1-weighted image (T1WI) (B) showing infiltrative and enhanced tumor involving entire trunks of left brachial plexus (arrows). Coronal FS T2WI (C) depicts hyperintense change without enhancement of roots (empty arrows), part of lower trunk (dotted arrow), and medial cord (thin arrow) originating from secondary compressive plexopathy, different from infiltrative tumor (thick arrows on A and B). There is no enhancement at corresponding segments of left brachial plexus on coronal CE FS T1WI (D).
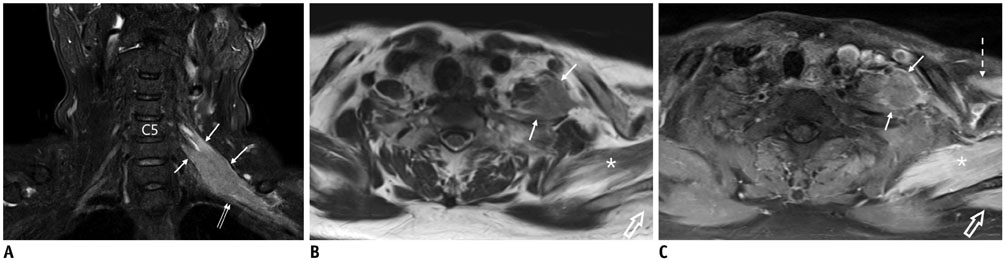
Fig. 6 66-year-old female with diffuse and large B-cell lymphoma involving brachial plexus. Coronal fat-suppressed (FS) T2-weighted image (T2WI) (A), axial T2WI (B), and contrast-enhanced (CE) FS T1-weighted image (C) demonstrating ill-defined infiltrating mass (arrows on A-C) involving left C5 and C6 nerve roots and upper trunk that displaces left middle trunk (double arrows on A) inferiorly. Note denervation changes with T2 hyperintensity and homogeneous enhancement of subscapularis (asterisk on B and C), supraspinatus (empty arrows on B and C), and pectoralis major (dotted arrow on C) muscles.

Fig. 7 56-year-old male with left shoulder weakness after radiation therapy for metastatic lymph nodes in left supraclavicular area due to right lung cancer. Coronal fat-suppressed (FS) T2-weighted images (T2WIs) (A, B) and axial T2WI (C) showing marked T2 hyperintensity of left C6 (long arrow on A), C7 (short arrows on A and B), and C8 (long arrow on B and C) nerve roots caused by radiation-induced brachial plexopathy. There are atrophy, T2 hyperintense change, enhancement of left paravertebral (thick arrow on C and D), middle and posterior scalene (asterisk on C and D), and levator scapulae (dotted arrow on C and D) muscles secondary to plexopathy. Note that C8 nerve roots (long arrow on D) are also diffusely enhanced by contrast agent on axial contrast-enhanced FS T1-weighted image (D). Short arrows on C denote normal right C6 and C7 nerve roots in interscalene triangle.

Fig. 8 55-year-old female with breast cancer and history of lymph node metastasis in left supraclavicular area. A-D. Axial T2-weighted images for evaluation of recent left Horner's syndrome and brachial plexopathy depicting infiltrating tumor invading longus colli, anterior, middle, and posterior scalene muscles, intervening brachial plexus (short arrows on A and B), and inferior cervical sympathetic ganglion (CSG, short arrows on C and D) on left side. Note normal middle CSG (long arrow on A) and inferior CSG (long arrow on D) on right side. Dotted arrows on B and D denote C8 and T1 nerve roots, respectively.

Fig. 9 Diagram of cervical plexus and its branches. A = greater auricular nerve, B = lesser occipital nerve, C = transverse cervical nerve, C2–C5 = 2nd to 5th cervical nerves, D = supraclavicular nerve, DI = intermediate branch, DL = lateral branch, DM = medial branch, E = phrenic nerve, EJV = external jugular vein, F = ansa cervicalis, G = trapezius muscle, H = platysma, I = cervical branch of facial nerve, J = parotid gland, K = SCM muscle, XI = spinal accessory nerve, XII = hypoglossal nerve

Fig. 10 Imaging appearance of normagreater auricular nerve and its pathology. A-E. Axial T2-weighted images depicting greater auricular nerve (long arrows) branching off from cervical plexus (dotted arrow on A and B), running posterolaterally in posterior cervical triangle, and wrapping around edge of sternocleidomastoid muscle (SCM, asterisk) to proceed to parotid gland. Note external jugular vein (EJV, arrowheads) running just anterior to greater auricular nerve on surface of SCM. F. Axial CT image showing typical case of schwannoma (arrow) arising from greater auricular nerve on outer surface of SCM (asterisk) posterior to EJV (arrowhead).

Fig. 11 24-year-old female with venolymphatic malformation in left posterior cervical triangle treated with radiofrequency ablation. Pre-treatment axial CT images (A-C) showing that part of non-enhancing lobulating mass (arrowheads on A-C) is incorporating greater auricular nerve (arrow on A). Patient had decreased sensation of left auricle and mastoid area following her treatment. Post-treatment axial contrast-enhanced CT images (D-F) showing decreased size with post-treatment enhancement of lesion at edge and posterior surface of sternocleidomastoid muscle (arrowheads on E and F). Note greater auricular nerve (arrow on D) at same location on A.

Fig. 12 56-year-old female with metastatic lymph node in left level IV after total thyroidectomy and left lateral neck dissection. A. Axial CT image showing enhancing lymph node with cystic change in left level IV (thick arrows) posterior to internal jugular vein (IJV, arrowhead) and anteromedial to left anterior scalene muscle (asterisk). B. Transverse ultrasonography image before radiofrequency ablation of lymph node clearly showing that phrenic nerve (thin arrow) is in close contact with metastatic lymph node (thick arrows) anteromedial to left scalene muscle (asterisk). Arrowhead denotes IJV. C. Axial T2-weighted image in another patient demonstrating relationship of phrenic nerve (thin arrow), IJV (arrowhead), anterior scalene muscle (asterisk), and vagus nerve (dotted arrow).

Fig. 13 66-year-old male after total thyroidectomy and right modified radical neck dissection for thyroid carcinoma. A. Postoperative axial CT image showing small ill-defined hypoattenuating mass in right level III (arrow). B. Ultrasonography image clearly showing C4 spinal nerve (short arrows) continuous from neural foramen to heterogeneous hypoechoic mass (long arrow), thus confirming traumatic neuroma.

Fig. 14 Distribution of vagus (A) and spinal accessory (B) nerves in neck. A = pharyngeal branch, B = superior laryngeal nerve, BE = external branch, BI = internal branch, C = left recurrent laryngeal nerve, D = superior, middle, and inferior cardiac nerves, E = right recurrent laryngeal nerve, F = trapezius muscle, G = sternocleidomastoid muscle, H = lymph node (level V), IX = glossopharyngeal nerve, SCA = right subclavian artery, SLA = superior laryngeal artery, STA = superior thyroid artery, X = vagus nerve, Xs = superior ganglion, Xi = inferior ganglion, XI = spinal accessory nerve

Fig. 15 A, B. Axial three-dimensional contrast-enhanced (CE) T1-weighted turbo field echo (T1-TFE) images (acquisition, 0.6 mm; reconstruction, 1.2 mm) showing relationship of glossopharyngeal (thin arrow on A) and spinal accessory (dotted arrow on A) nerves and superior vagal ganglion (thick arrow on A) at jugular foramen. After exiting jugular foramen, vagus nerve becomes prominent, forming inferior vagal ganglion (thick arrow on B). C. On CE fat-suppressed (FS) T1-weighted image (turbo spin echo; image acquisition, 3-mm slice thickness with no gap) in different patient, inferior vagal ganglion (thick arrow) is homogeneously enhanced by contrast agent similar to top of superior sympathetic ganglion (arrowhead) located medial to ICA. D. Axial CE FS T1-TFE image of patient with metastasis to skull base showing large enhancing mass invading right occipitotemporal bone, including jugular foramen (short arrows) but not containing discernible lower cranial nerves. Note normal, superior vagal ganglion (long arrow), and glossopharyngeal nerve (thin arrow) on left side.

Fig. 16 Axial CT (A-C) and axial contrast-enhanced fat-suppressed T1-weighted (D) images in four different patients with vagal schwannomas (long arrows) demonstrating anatomical variations of vagus nerve within carotid sheath displacing internal jugular vein (short arrows) and internal carotid artery (thin arrow on A) or common carotid artery (thin arrows on B-D) in different directions. Note vocal-cord atrophy (asterisk) caused by vagus nerve palsy on ipsilateral side in B.
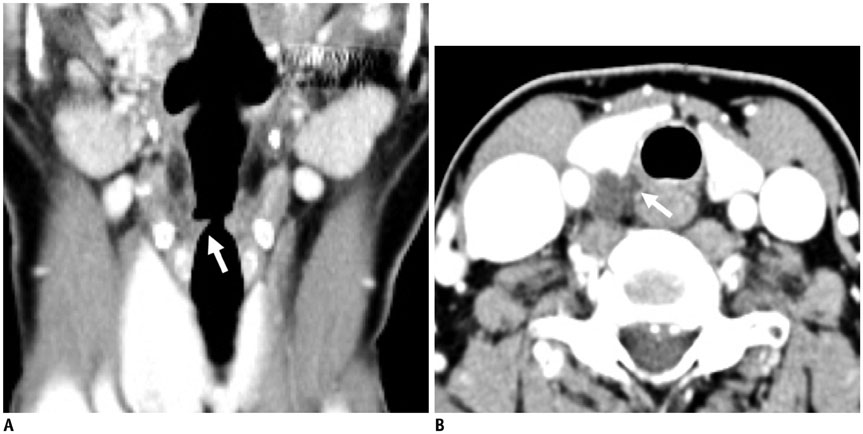
Fig. 17 A 54-year-old male with recent voice change. A. Reconstructed coronal CT image showing subtle fatty atrophy of right vocal cord (arrow) with secondary dilatation of ipsilateral laryngeal ventricle from vocal cord palsy. B. Axial CT image at level of thyroid demonstrating irregular cystic mass insinuating into right tracheoesophageal groove (arrow). Lesion was confirmed as ruptured parathyroid cyst with intracystic bleeding.

Fig. 18 55-year-old male with voice change after interbody fusion of C6/7 using anterior approach. A-C. There is metallic fusion device at C6/7 level (A). Laryngeal ventricle is dilated (asterisk on B) due to atrophy of thyroarytenoid muscle on right side. Note aberrant right subclavian artery (arrow on C) running posterior to esophagus at thoracic inlet, implying presence of right non-recurrent laryngeal nerve.

Fig. 19 32-year-old female who underwent radical neck dissection for advanced tongue cancer. There is neither internal jugular vein nor sternocleidomastoid muscle on left side caused by previous surgery. Note denervation atrophy of left trapezius muscle (arrows) and secondary hypertrophy of rhomboid muscle (arrowheads).
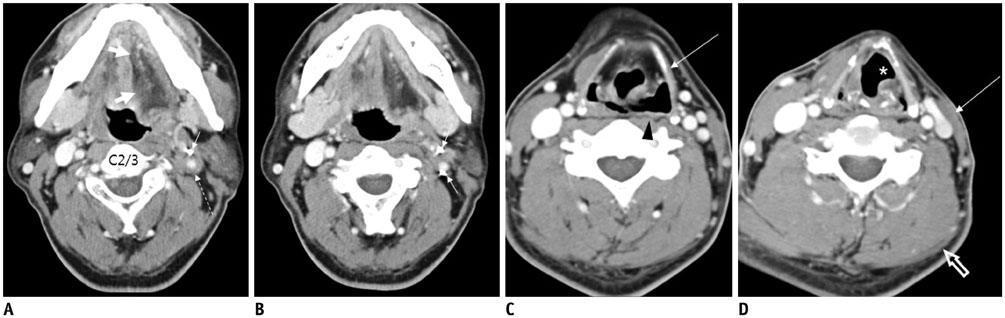
Fig. 20 47-year-old male with multiple cranial nerve palsy after explosion. A-D. Axial CT images demonstrating tiny metallic foreign bodies with hematoma (dotted arrow) surrounding left internal carotid artery (short arrows on A and B). Note that left internal jugular vein is obliterated on A and B. Left side of tongue (thick arrows on A) and left thyrohyoid muscle (long arrow on C) are atrophic due to hypoglossal nerve injury. Atrophy of left vocal cord (asterisk on D) and left side of hypopharyngeal wall (arrowhead on C) suggest vagus nerve injury. Atrophy of left sternocleidomastoid muscle (long arrow on D) and left trapezius muscle (empty arrow on D) implies damage to spinal accessory nerve.
Cited by 1 articles
-
Use of Magnetic Resonance Neurography for Evaluating the Distribution and Patterns of Chronic Inflammatory Demyelinating Polyneuropathy
Xiaoyun Su, Xiangquan Kong, Zuneng Lu, Min Zhou, Jing Wang, Xiaoming Liu, Xiangchuang Kong, Huiting Zhang, Chuansheng Zheng
Korean J Radiol. 2020;21(4):483-493. doi: 10.3348/kjr.2019.0739.
Reference
-
1. Kiray A, Arman C, Naderi S, Güvencer M, Korman E. Surgical anatomy of the cervical sympathetic trunk. Clin Anat. 2005; 18:179–185.2. Saylam CY, Ozgiray E, Orhan M, Cagli S, Zileli M. Neuroanatomy of cervical sympathetic trunk: a cadaveric study. Clin Anat. 2009; 22:324–330.3. Lee JH, Lee HK, Lee DH, Choi CG, Kim SJ, Suh DC. Neuroimaging strategies for three types of Horner syndrome with emphasis on anatomic location. AJR Am J Roentgenol. 2007; 188:W74–W81.4. Lee JY, Lee JH, Song JS, Song MJ, Hwang SJ, Yoon RG, et al. Superior cervical sympathetic ganglion: normal imaging appearance on 3T-MRI. Korean J Radiol. 2016; 17:e72.5. Hogan QH, Erickson SJ. MR imaging of the stellate ganglion: normal appearance. AJR Am J Roentgenol. 1992; 158:655–659.6. Shin JE, Baek JH, Ha EJ, Choi YJ, Choi WJ, Lee JH. Ultrasound features of middle cervical sympathetic ganglion. Clin J Pain. 2015; 31:909–913.7. Mancall EL, Brock DG. Cervical plexus. In : Mancall EL, Brock DG, editors. Gray's clinical neuroanatomy: the anatomic basis for clinical neuroscience. Philadelphia: Elsevier Health Sciences;2011. p. 315–317.8. Bowen BC, Pattany PM, Saraf-Lavi E, Maravilla KR. The brachial plexus: normal anatomy, pathology, and MR imaging. Neuroimaging Clin N Am. 2004; 14:59–85. vii–viii.9. Aralasmak A, Karaali K, Cevikol C, Uysal H, Senol U. MR imaging findings in brachial plexopathy with thoracic outlet syndrome. AJNR Am J Neuroradiol. 2010; 31:410–417.10. van Es HW, Bollen TL, van Heesewijk HP. MRI of the brachial plexus: a pictorial review. Eur J Radiol. 2010; 74:391–402.11. Ha EJ, Lee JH, Lim HK, Bae Kim W, Baek JH. Identification of continuity of transected nerve on sonography after neck dissection: direct sign of traumatic neuroma. Thyroid. 2011; 21:1385–1387.12. Ha EJ, Baek JH, Lee JH, Kim YJ, Kim JK, Kim TY, et al. Characteristic ultrasound feature of traumatic neuromas after neck dissection: direct continuity with the cervical plexus. Thyroid. 2012; 22:820–826.13. Ha EJ, Baek JH, Lee JH, Kim JK, Shong YK. Clinical significance of vagus nerve variation in radiofrequency ablation of thyroid nodules. Eur Radiol. 2011; 21:2151–2157.14. Felten DL, O'Banion MK, Maida ME. Brain stem and cerebellum. In : Felten DL, O'Banion MK, Maida ME, editors. Netter's atlas of neuroscience. Philadelphia: Elsevier Health Sciences;2015. p. 247–287.15. Park JK, Jeong SY, Lee JH, Lim GC, Chang JW. Variations in the course of the cervical vagus nerve on thyroid ultrasonography. AJNR Am J Neuroradiol. 2011; 32:1178–1181.16. Henry JF, Audiffret J, Denizot A, Plan M. The nonrecurrent inferior laryngeal nerve: review of 33 cases, including two on the left side. Surgery. 1988; 104:977–984.17. Toniato A, Mazzarotto R, Piotto A, Bernante P, Pagetta C, Pelizzo MR. Identification of the nonrecurrent laryngeal nerve during thyroid surgery: 20-year experience. World J Surg. 2004; 28:659–661.18. Chen CC, Huang YC, Lee ST, Chen JF, Wu CT, Tu PH. Long-term result of vocal cord paralysis after anterior cervical disectomy. Eur Spine J. 2014; 23:622–626.19. Jung A, Schramm J. How to reduce recurrent laryngeal nerve palsy in anterior cervical spine surgery: a prospective observational study. Neurosurgery. 2010; 67:10–15. discussion 15.20. Saman M, Etebari P, Pakdaman MN, Urken ML. Anatomic relationship between the spinal accessory nerve and the jugular vein: a cadaveric study. Surg Radiol Anat. 2011; 33:175–179.21. Hong MJ, Baek JH, Kim DY, Ha EJ, Choi WJ, Choi YJ, et al. Spinal accessory nerve: ultrasound findings and correlations with neck lymph node levels. Ultraschall Med. 2014; 12. 17. [Epub]. DOI: 10.1055/s-0034-1385673.22. Kim DH, Cho YJ, Tiel RL, Kline DG. Surgical outcomes of 111 spinal accessory nerve injuries. Neurosurgery. 2003; 53:1106–1112. discussion 1102-1103.23. Cappiello J, Piazza C, Nicolai P. The spinal accessory nerve in head and neck surgery. Curr Opin Otolaryngol Head Neck Surg. 2007; 15:107–111.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- High-Resolution Finger MRI: What Should You Look for in Trauma of the Fingers?
- Ansa cervicalis: a comprehensive review of its anatomy, variations, pathology, and surgical applications
- Imaging of the Brachial Plexus
- Magnetic Resonance Imaging in Diplopia: Neural Pathway, Imaging, and Clinical Correlation
- Anatomy and Pathology of the L5 Exiting Nerve in the Lumbosacral Spine
