Perirectal Cystic Lesions - Comprehensive CT and MRI Findings
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. ljs@amc.seoul.kr
- KMID: 2468047
- DOI: http://doi.org/10.13104/imri.2019.23.4.283
Abstract
- Perirectal cystic lesions are rare entities, for which only a relatively few research publications are available. These lesions are heterogeneous in nature and can range from benign lesions to malignant lesions; thus, they are sometimes difficult to differentiate. Some studies have reported on retrorectal or presacral cystic lesions, but to our knowledge, there have been only a few reports on perirectal cystic lesions. Cystic lesions arise from the retrorectal space as well as the rectal lumen or adjacent organ, and they should be differentiated based on their characteristics and anatomic location. Thus, we comprehensively studied diseases with a cystic component around the rectum, which are perirectal cystic lesions. A clinical challenge with perirectal cystic lesions is that it is sometimes difficult to distinguish malignant lesions from benign lesions and is thus difficult to determine the extent for surgical excision. We thus attempted to identify benign and malignant imaging features of perirectal cystic lesions.
Keyword
MeSH Terms
Figure
-
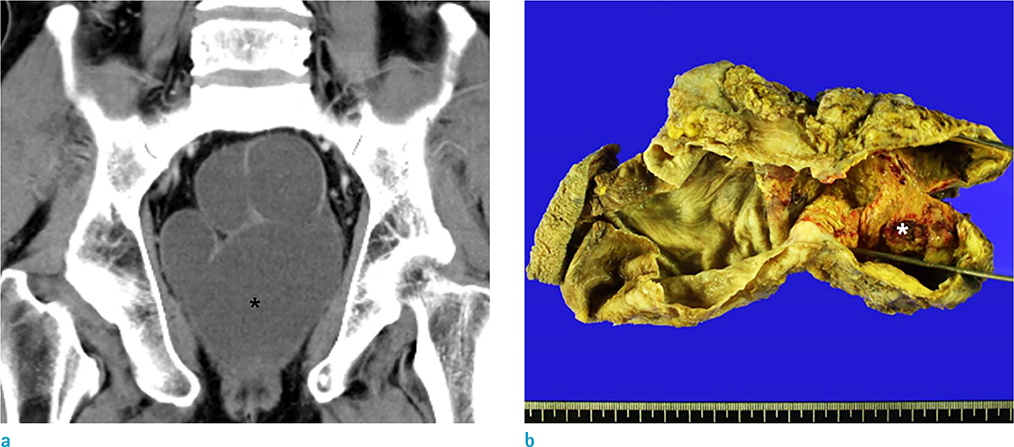
Fig. 1 Tailgut cyst in an age 59 male. (a) Contrast-enhanced coronal CT scan shows a multilocular cystic lesion (*) without solid component in the perirectal region. (b) Photograph of the gross pathologic specimen of the tailgut cyst shows a welldemarcated, multilocular, cystic mass (*) without a solid component.

Fig. 2 Tailgut cyst in an age 54 male. (a, b) T1-weighted and T2-weighted axial MR image show a well-defined, thin-walled cystic mass with inhomogeneous signal intensity between the lower rectum and the coccyx (*).
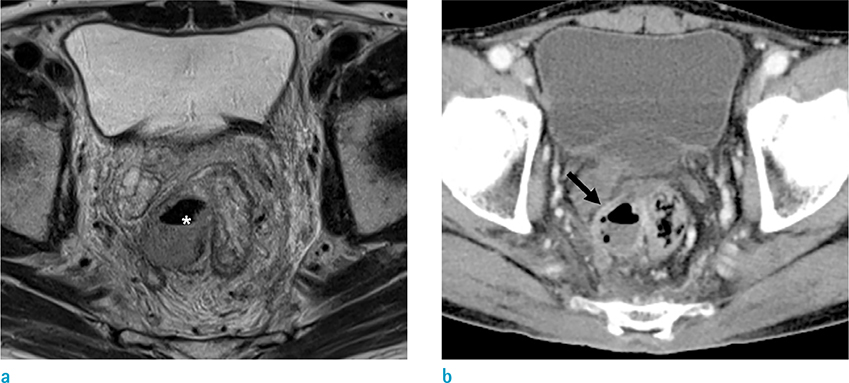
Fig. 3 Rectal abscess in an age 70 male who presented with fever and abdominal pain. (a) T2-weighted axial MR image shows a well-demarcated lesion with air-fluid level (*). (b) Contrast-enhanced axial CT scan shows capsular ring enhancement with contrast (arrow). Mild fat infiltration around the rectum also is observed.
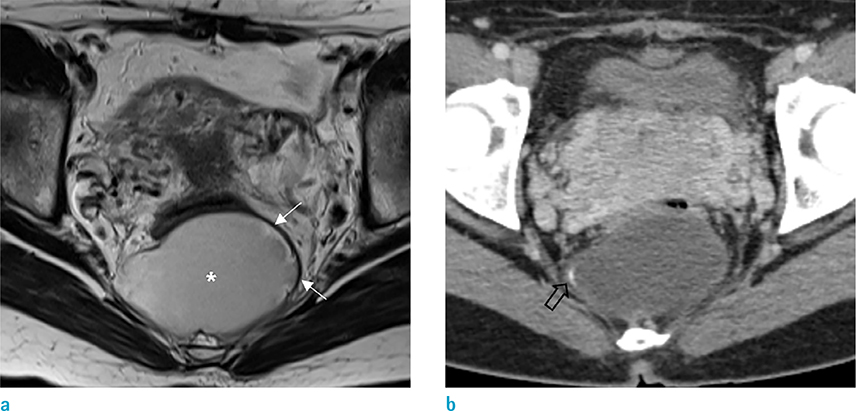
Fig. 4 Teratoma in an age 36 female. (a) T2-weighted axial MR image shows a well-defined cystic lesion (*) with unevenly surrounded wall (arrows). (b) Contrast-enhanced axial CT scan shows a lobulated cystic lesion with focal calcification in the wall (empty arrow).
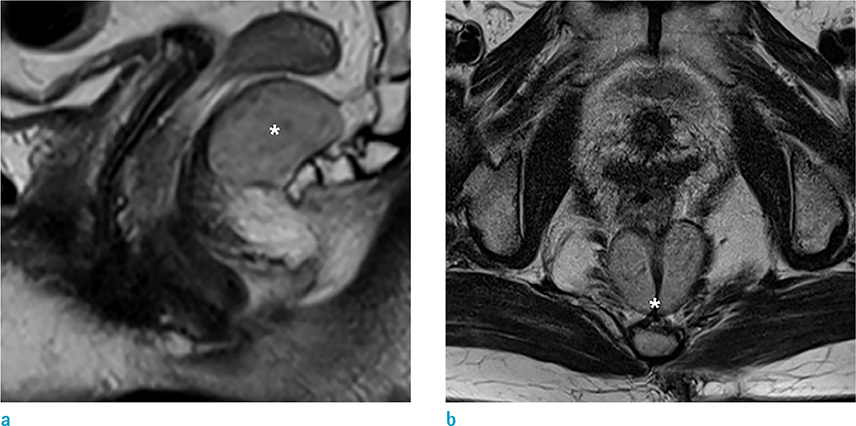
Fig. 5 Epidermoid cyst in an age 65 female. (a, b) axial T2-weighted MR image shows a thin-walled lobulated lesion (*) with mainly high and overall heterogeneous signal intensity in the rectum.

Fig. 6 A dermoid cyst in an age 48 female. (a, b) Sagittal and axial T2- and T1-weighted MR image show a thin-walled lobulated cystic mass (*) without internal solid portion. (c) Contrast enhanced T1-weighted MR image shows no visible enhancement in the cystic mass (*).
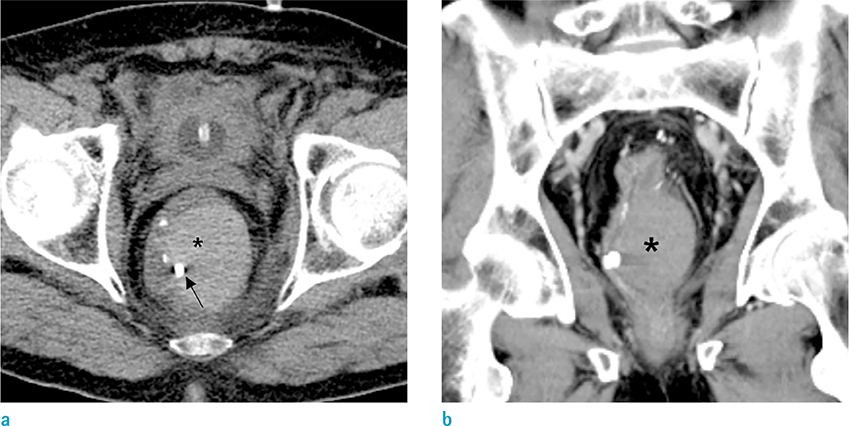
Fig. 7 Intramural hematoma of the rectum in an age 74 male who presented with hematochezia and treated by endoscopic clipping. (a) Non-enhanced axial CT scan shows a hyperdense lesion (*) with the endoscopic clip (arrow). (b) Contrastenhanced coronal CT image shows a non-enhanced lesion (*) and no contrast extravasation.
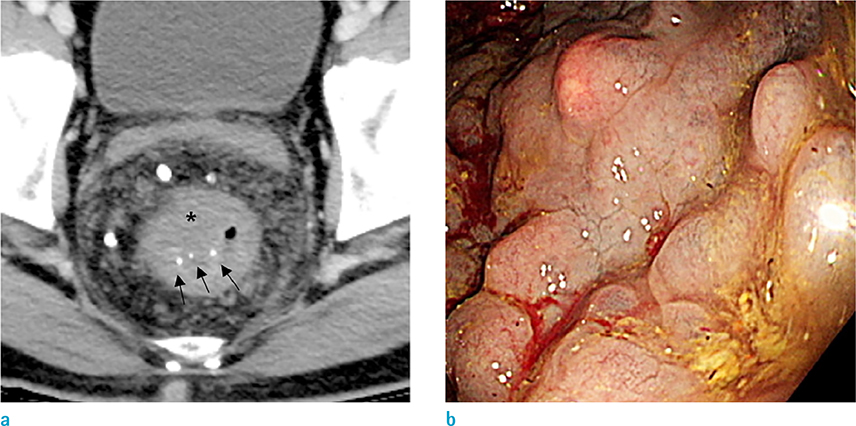
Fig. 8 Endoscopic diagnosis of a diffuse cavernous hemangioma in an age 41 male. (a) Contrast-enhanced axial CT image shows an eccentric wall thickening of the rectum (*) with some internal calcification (arrows) and low attenuating portions. (b) Colonoscopy shows numerous, prune-colored, polypoid lesions.
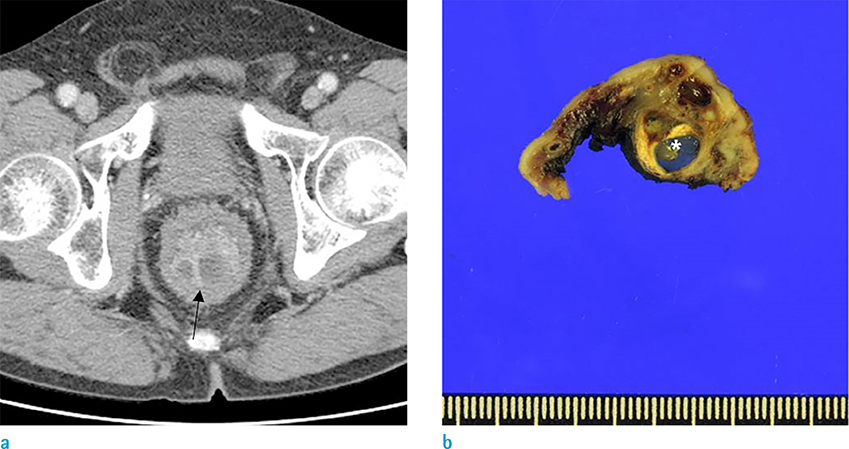
Fig. 9 Colitis cystica profunda in an age 67 male. (a) Contrast-enhanced axial CT scan shows edematous rectal wall thickening with a septated submucosal cystic lesion (arrow) in the posterior wall of the rectum. (b) The photograph of the gross pathologic specimen of colitis cystica profunda shows a well-demarcated submucosal cyst (*).
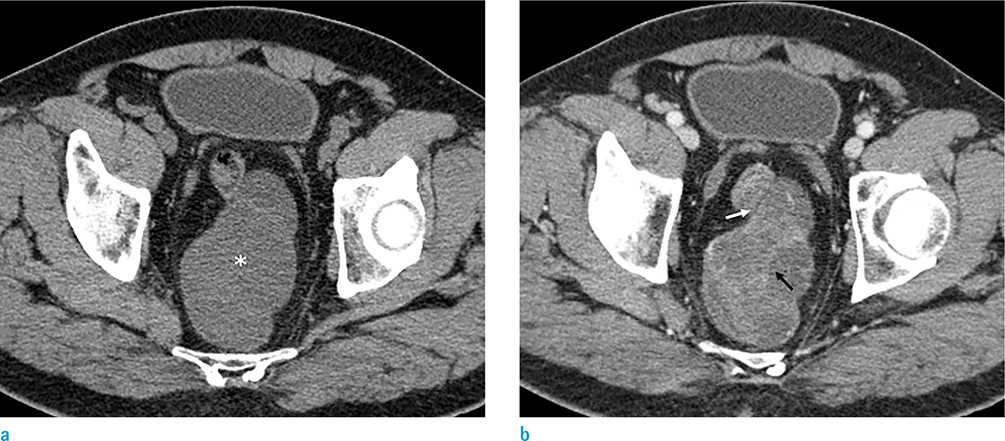
Fig. 10 Primary extracranial meningioma in an age 67 male. (a) Pre-enhanced axial CT scan shows a well-defined and lobulated mass with inhomogeneous low density that mainly consists of a cystic component (*). (b) Contrast-enhanced axial CT image shows enhancing peripheral areas and internal septa-like enhancement (black arrow). This mass is closely abutting to the rectum with maintained fat planes (white arrow).
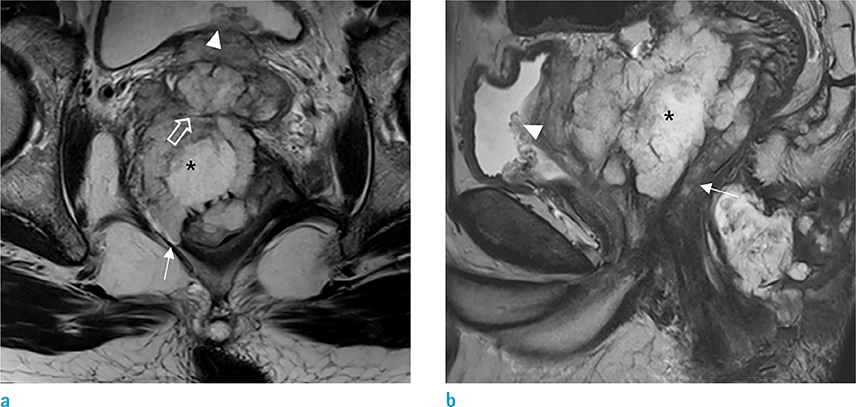
Fig. 11 Mucinous adenocarcinoma in an age 52 male who presented with anal pain. (a, b) Axial and sagittal T2-weighted MR image shows a lobulated, high signal intensity lesion around the rectum (*) and with invasion of the prostate (empty arrow), posterior wall of the urinary bladder (arrowheads), and right levator ani muscle (arrows).
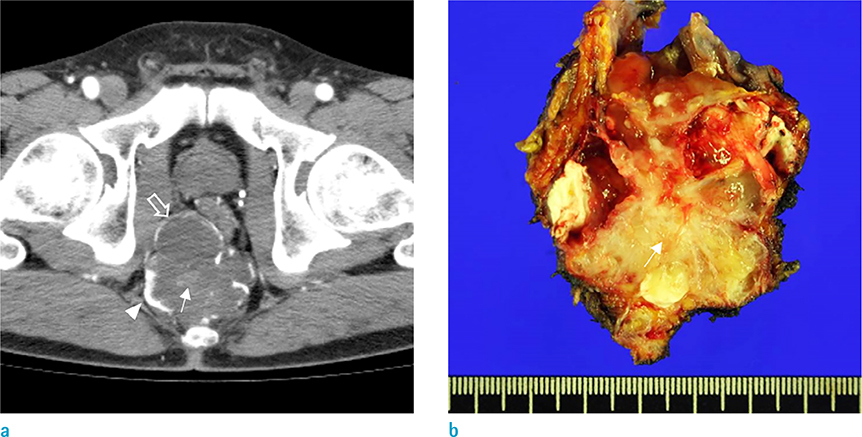
Fig. 12 Mucinous adenocarcinoma arising from a tailgut cyst in an age 66 male. (a) Contrast-enhanced axial CT scan shows a multiseptated cystic lesion with a thickened wall (empty arrow), rim calcification (arrowhead), and internal enhancing solid component (arrow). (b) Photograph of the gross pathologic specimen of the cystic lesion shows a well-demarcated multilocular cystic mass with an internal solid component (arrow).
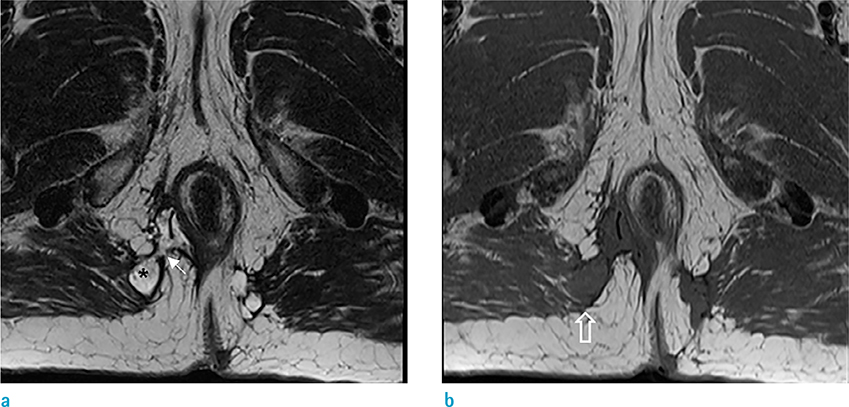
Fig. 13 An age 60 male with mucinous adenocrcinoma arising from a fistula-in-ano who presented with anal pain. (a) Axial T2-weighted MR image shows a trans-sphincteric fistula (arrow) and a multiloculated cystic lesion arising from the fistula (*). (b) Axial T1-weighted image shows a low signal intensity lesion that extends to the right gluteus muscle (empty arrow).
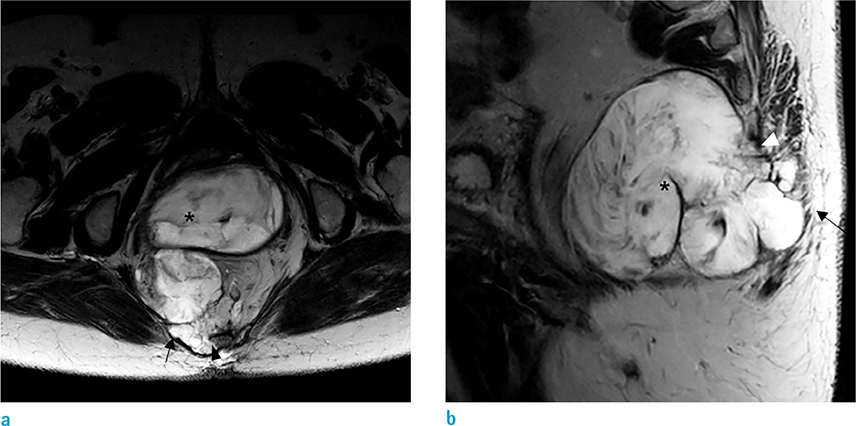
Fig. 14 Mucinous adenocarcinoma arising from mature teratoma in an age 61 female who presented with a palpable, coccygeal mass. (a, b) Axial and sagittal T2-weighted MR image shows a multiloculated, cystic lesion with heterogeneous signal intensity (*) that extends to the gluteus maximus (arrows) and coccyx (arrowheads).
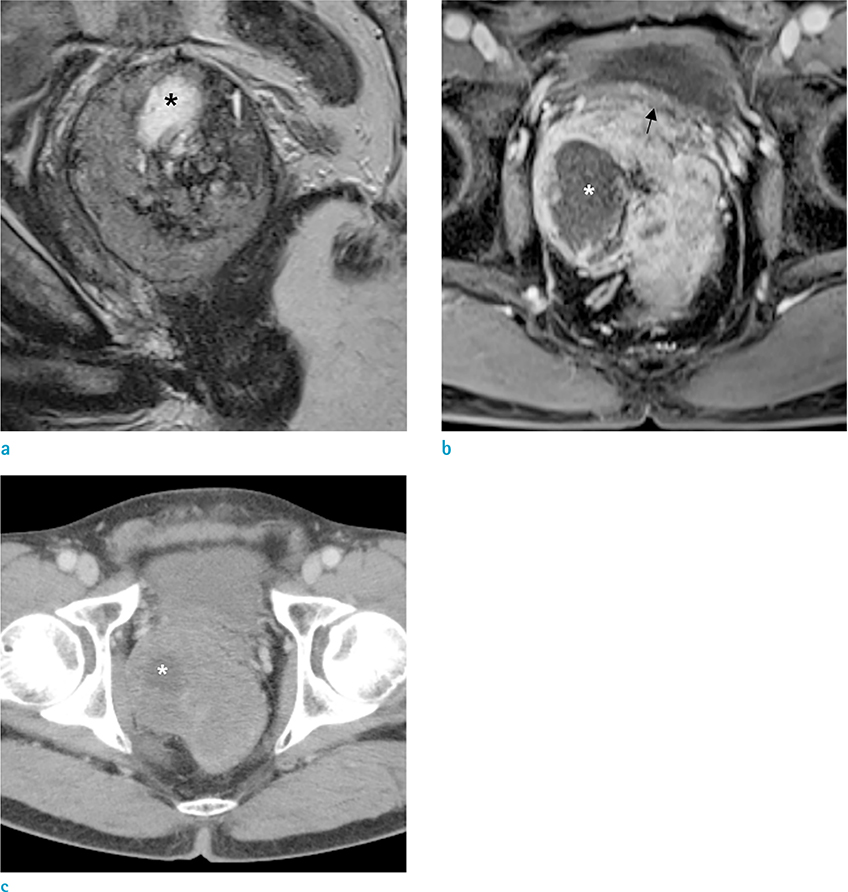
Fig. 15 Rectal GIST in an age 60 female. (a) Sagittal T2-weighted, MR image shows a mass abutting to the rectum with heterogeneous signal intensity and internal bright signal intensity (*). (b) Contrast-enhanced T1-weighted MR image shows an inhomogeneous enhancing mass with unenhanced cystic portion (*) that displaced the bladder anteriorly (arrow). (c) Contrast-enhanced axial CT scan shows a heterogeneously enhancing mass with internal cystic portion (*).
Reference
-
1. Lee J, Park CM, Kim KA, et al. Cystic lesions of the gastrointestinal tract: multimodality imaging with pathologic correlations. Korean J Radiol. 2010; 11:457–468.2. Purysko AS, Coppa CP, Kalady MF, et al. Benign and malignant tumors of the rectum and perirectal region. Abdom Imaging. 2014; 39:824–852.3. Yang DM, Park CH, Jin W, et al. Tailgut cyst: MRI evaluation. AJR Am J Roentgenol. 2005; 184:1519–1523.4. Llauger J, Palmer J, Perez C, Monill J, Ribe J, Moreno A. The normal and pathologic ischiorectal fossa at CT and MR imaging. Radiographics. 1998; 18:61–82.5. Guillaumin E, Jeffrey RB Jr, Shea WJ, Asling CW, Goldberg HI. Perirectal inflammatory disease: CT findings. Radiology. 1986; 161:153–157.6. Afuwape OO, Ogundoyin OO, Ogunlana DI, Adeleye AO. Adult sacrococcygeal teratoma: a case report. Ghana Med J. 2009; 43:40–42.7. Kumar N, Khosla D, Kumar R, Saikia UN, Singh S. Sacrococcygeal teratoma in adult: Two rare case reports and review of literature. Int J Appl Basic Med Res. 2014; 4:122–124.8. Alvi MI, Mubarak F, Khandwala K, Barakzai MD, Memon A. A rare case of presacral epidermoid cyst in an adult male: Emphasis on diffusion weighted magnetic resonance sequences in preoperative imaging. Cureus. 2018; 10:e2050.9. Kesici U, Sakman G, Mataraci E. Retrorectal/Presacral epidermoid cyst: report of a case. Eurasian J Med. 2013; 45:207–210.10. Dahan H, Arrive L, Wendum D, Docou le Pointe H, Djouhri H, Tubiana JM. Retrorectal developmental cysts in adults: clinical and radiologic-histopathologic review, differential diagnosis, and treatment. Radiographics. 2001; 21:575–584.11. Dwarkasing RS, Verschuuren SI, van Leenders G, Braun LMM, Krestin GP, Schouten WR. Primary cystic lesions of the retrorectal space: MRI evaluation and clinical assessment. AJR Am J Roentgenol. 2017; 209:790–796.12. O'Malley CM, Remer EM, Delaney C. Imaging of the presacral space. Semin Colon Rectal Surg. 2004; 15:2–11.13. Battal B, Kocaoglu M, Ors F, Akgun V, Tasar M. Obstructive rectal intramural hematoma caused by a foreign body. Emerg Radiol. 2009; 16:75–77.14. Dhawan V, Mohamed A, Fedorak RN. Gastric intramural hematoma: a case report and literature review. Can J Gastroenterol. 2009; 23:19–22.15. Sztarkier I, Benharroch D, Walfisch S, Delgado J. Colitis cystica profunda and solitary rectal ulcer syndrome-polypoid variant: Two confusing clinical conditions. Eur J Intern Med. 2006; 17:578–579.16. Inan N, Arslan AS, Akansel G, Anik Y, Gurbuz Y, Tugay M. Colitis cystica profunda: MRI appearance. Abdom Imaging. 2007; 32:239–242.17. Lang FF, Macdonald OK, Fuller GN, DeMonte F. Primary extradural meningiomas: a report on nine cases and review of the literature from the era of computerized tomography scanning. J Neurosurg. 2000; 93:940–950.18. Kyalakond K, Saini S, Rajagopal K, Karegowda LH. Radiological appearance of primary extracranial meningioma of the pelvis in a middle-aged woman. BMJ Case Rep. 2018; 2018.19. Taori K, Kundaragi NG, Disawal A, et al. Imaging features of extra cranial parapharyngeal space meningioma: case report. Iran J Radiol. 2011; 8:176–181.20. Rullier A, Laurent C, Vendrely V, Le Bail B, Bioulac-Sage P, Rullier E. Impact of colloid response on survival after preoperative radiotherapy in locally advanced rectal carcinoma. Am J Surg Pathol. 2005; 29:602–606.21. Hanski C. Is mucinous carcinoma of the colorectum a distinct genetic entity? Br J Cancer. 1995; 72:1350–1356.22. Sjodahl RI, Myrelid P, Soderholm JD. Anal and rectal cancer in Crohn's disease. Colorectal Dis. 2003; 5:490–495.23. Lee NK, Kim S, Kim HS, et al. Spectrum of mucin-producing neoplastic conditions of the abdomen and pelvis: cross-sectional imaging evaluation. World J Gastroenterol. 2011; 17:4757–4771.24. Chhabra S, Wise S, Maloney-Patel N, Rezac C, Poplin E. Adenocarcinoma associated with tail gut cyst. J Gastrointest Oncol. 2013; 4:97–100.25. Au E, Anderson O, Morgan B, Alarcon L, George ML. Tailgut cysts: report of two cases. Int J Colorectal Dis. 2009; 24:345–350.26. Gonul , II , Baglan T, Pala I, Mentes B. Tailgut cysts: diagnostic challenge for both pathologists and clinicians. Int J Colorectal Dis. 2007; 22:1283–1285.27. Johnson AR, Ros PR, Hjermstad BM. Tailgut cyst: diagnosis with CT and sonography. AJR Am J Roentgenol. 1986; 147:1309–1311.28. Lim KE, Hsu WC, Wang CR. Ta i lgut cyst wi th malignancy: MR imaging findings. AJR Am J Roentgenol. 1998; 170:1488–1490.29. Moulopoulos LA, Karvouni E, Kehagias D, Dimopoulos MA, Gouliamos A, Vlahos L. MR imaging of complex tail-gut cysts. Clin Radiol. 1999; 54:118–122.30. Getz SB Jr, Ough YD, Patterson RB, Kovalcik PJ. Mucinous adenocarcinoma developing in chronic anal fistula: report of two cases and review of the literature. Dis Colon Rectum. 1981; 24:562–566.31. Heidenreich A, Collarini HA, Paladino AM, Fernandez JM, Calvo TO. Cancer in anal fistulas: report of two cases. Dis Colon Rectum. 1966; 9:371–376.32. Hama Y, Makita K, Yamana T, Dodanuki K. Mucinous adenocarcinoma arising from fistula in ano: MRI findings. AJR Am J Roentgenol. 2006; 187:517–521.33. Kim JH, Lee TS, Oh HK, Choi YS. A case of mucinous adenocarcinoma arising from retroperitoneal teratoma treated with chemoradiation. J Gynecol Oncol. 2009; 20:126–128.34. Chang YL, Wu CT, Lee YC. Mediastinal and retroperitoneal teratoma with focal gastrointestinal adenocarcinoma. J Thorac Oncol. 2006; 1:729–731.35. Jiang ZX, Zhang SJ, Peng WJ, Yu BH. Rectal gastrointestinal stromal tumors: imaging features with clinical and pathological correlation. World J Gastroenterol. 2013; 19:3108–3116.36. Hong X, Choi H, Loyer EM, Benjamin RS, Trent JC, Charnsangavej C. Gastrointestinal stromal tumor: role of CT in diagnosis and in response evaluation and surveillance after treatment with imatinib. Radiographics. 2006; 26:481–495.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparative Diagnostic Performance of Multidetector Computed Tomography and MRI for Characterization of Pancreatic Cystic Lesions
- Radiologic Findings of Pancreatic Cystic Neoplasms
- Computed tomography of the rectal and anal cancer
- Pancreatic Tumors: Emphasis on CT Findings and Pathologic Classification
- CT and MRI Findings of Malignant Meningiomas: Comparison with Benign Meningiomas
