Clinical Features and Radiological Findings of Adenovirus Pneumonia Associated with Progression to Acute Respiratory Distress Syndrome: A Single Center Study in 19 Adult Patients
- Affiliations
-
- 1Department of Radiology, Chung-Ang University Hospital, Chung-Ang University College of Medicine, Seoul 06973, Korea.
- 2Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 06351, Korea. mj1.chung@samsung.com
- 3Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 06351, Korea.
- KMID: 2466291
- DOI: http://doi.org/10.3348/kjr.2016.17.6.940
Abstract
OBJECTIVE
To describe radiologic findings of adenovirus pneumonia and to understand clinico-radiological features associated with progression to acute respiratory distress syndrome (ARDS) in patients with adenovirus pneumonia.
MATERIALS AND METHODS
This study included 19 patients diagnosed with adenovirus pneumonia at a tertiary referral center, in the period between March 2003 and April 2015. Clinical findings were reviewed, and two radiologists assessed imaging findings by consensus. Chi-square, Fisher's exact, and Student's t tests were used for comparing patients with and without subsequent development of ARDS.
RESULTS
Of 19 patients, nine were immunocompromised, and 10 were immunocompetent. Twelve patients (63%) progressed to ARDS, six of whom (32%) eventually died from the disease. The average time for progression to ARDS from symptom onset was 9.6 days. Initial chest radiographic findings were normal (n = 2), focal opacity (n = 9), or multifocal or diffuse opacity (n = 8). Computed tomography (CT) findings included bilateral (n = 17) or unilateral (n = 2) ground-glass opacity with consolidation (n = 14) or pleural effusion (n = 11). Patients having subsequent ARDS had a higher probability of pleural effusion and a higher total CT extent compared with the non-ARDS group (p = 0.010 and 0.007, respectively). However, there were no significant differences in clinical variables such as patient age and premorbid condition.
CONCLUSION
Adenovirus pneumonia demonstrates high rates of ARDS and mortality, regardless of patient age and premorbid conditions, in the tertiary care setting. Large disease extent and presence of pleural effusion on CT are factors suggestive of progression to ARDS.
MeSH Terms
-
Acute Disease
Adenoviridae/isolation & purification
Adult
Aged
Disease Progression
Female
Humans
Immunocompromised Host
Male
Middle Aged
Pneumonia, Viral/complications/*diagnosis/diagnostic imaging/virology
Radiography
Respiratory Distress Syndrome, Adult/*diagnosis/etiology
Retrospective Studies
Tertiary Care Centers
Thorax/diagnostic imaging
Tomography, X-Ray Computed
Figure
-
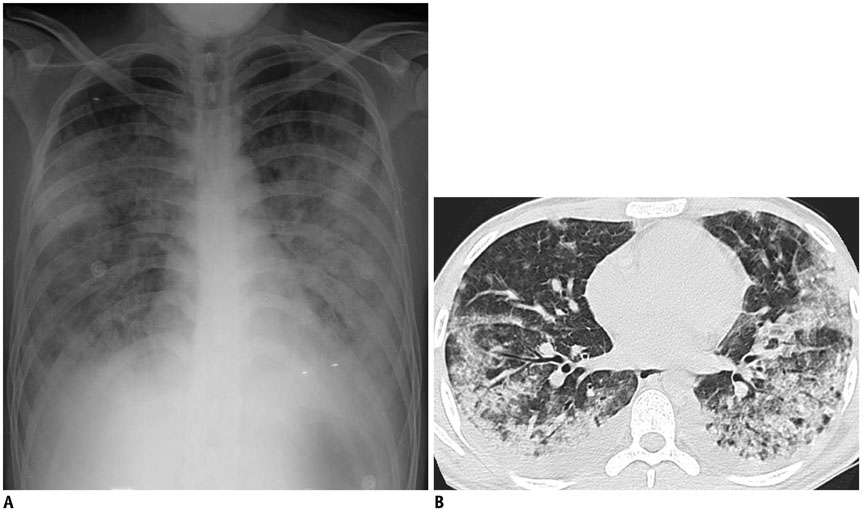
Fig. 1 20-year-old immunocompetent man complaining of fever, dyspnea, productive cough, and sputum. He visited our hospital on 10th day from onset of his symptoms, which were abruptly aggravated two days prior. A. Chest radiograph demonstrates multifocal or diffuse opacity. B. Chest CT scan obtained on same day demonstrates extensive airspace lesions in both lungs, with bilateral pleural effusions. Total CT score was 13. Culture of BAL fluid helped confirm adenovirus pneumonia. On next day, patient was transferred to intensive care unit, and he eventually expired on 21st day of hospitalization. BAL = bronchoalveolar lavage, CT = computed tomography
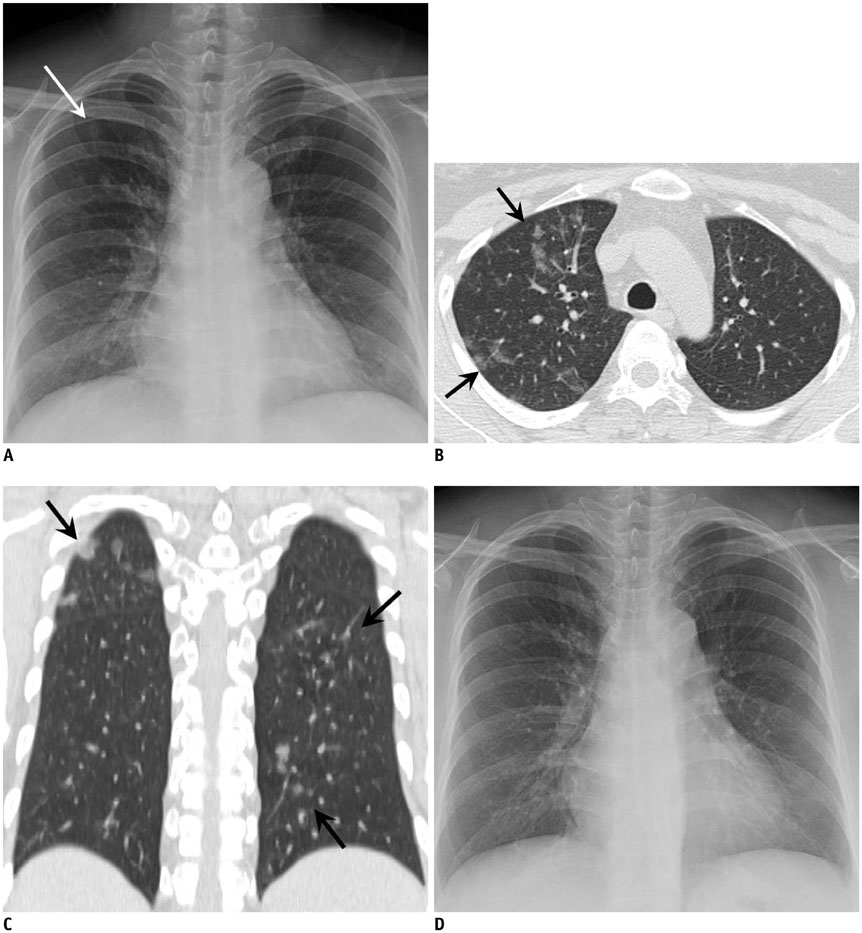
Fig. 2 38-year-old woman with acute myelogenous leukemia visited our institution for aggravated fever, cough, sputum, and dyspnea for four days. A. Chest radiograph at admission demonstrates subtle focal opacity in right upper lung zone (white arrow). B, C. Chest CT scans obtained on same day demonstrate patchy peribronchial ground-glass opacity in both lungs (black arrows). Total CT score was 3. Culture and RT-PCR of BAL fluid confirmed adenovirus pneumonia. D. Follow-up chest radiograph obtained after two weeks of treatment with cidofovir demonstrates disappearance of focal opacity in right upper lung zone, suggesting type 1 disease pattern. BAL = bronchoalveolar lavage, CT = computed tomography, RT-PCR = reverse transcription polymerase chain reaction
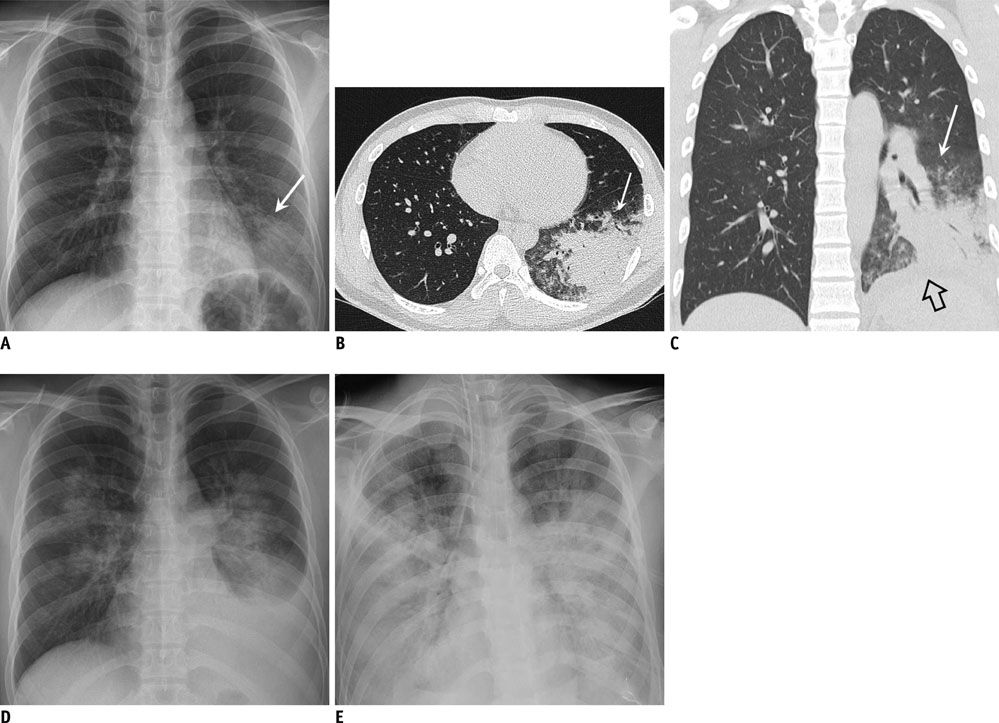
Fig. 3 20-year-old immunocompetent man suffering from acute fever and dyspnea. A. Chest radiograph obtained on fifth day of illness demonstrates focal opacity in left lower lobe (arrow). B, C. Chest CT scans demonstrate dense consolidation and ground-glass opacity in left lower lobe (arrow). Small left pleural effusion is indicated by open arrow. Total CT score was 7. D. Chest radiograph obtained on seventh day of illness demonstrates increased amount of left pleural effusion and bilateral multifocal areas of parenchymal opacity. E. Progressive diffuse opacity in both lungs and bilateral pleural effusions are shown on follow-up radiograph taken on 13th day, suggesting ARDS and type 4 disease pattern. Patient expired on 16th day of illness. ARDS = acute respiratory distress syndrome, CT = computed tomography
Cited by 1 articles
-
Characteristics and Outcomes of Patients with Pulmonary Acute Respiratory Distress Syndrome Infected with Influenza versus Other Respiratory Viruses
Jung-Wan Yoo, Sunmi Ju, Seung Jun Lee, Min-Chul Cho, Yu Ji Cho, Yi Yeong Jeong, Jong Deog Lee, Ho Choel Kim
Tuberc Respir Dis. 2019;82(4):328-334. doi: 10.4046/trd.2019.0017.
Reference
-
1. Han BK, Son JA, Yoon HK, Lee SI. Epidemic adenoviral lower respiratory tract infection in pediatric patients: radiographic and clinical characteristics. AJR Am J Roentgenol. 1998; 170:1077–1080.2. Krilov LR, Rubin LG, Frogel M, Gloster E, Ni K, Kaplan M, et al. Disseminated adenovirus infection with hepatic necrosis in patients with human immunodeficiency virus infection and other immunodeficiency states. Rev Infect Dis. 1990; 12:303–307.3. Echavarria MS, Ray SC, Ambinder R, Dumler JS, Charache P. PCR detection of adenovirus in a bone marrow transplant recipient: hemorrhagic cystitis as a presenting manifestation of disseminated disease. J Clin Microbiol. 1999; 37:686–689.4. Landry ML, Fong CK, Neddermann K, Solomon L, Hsiung GD. Disseminated adenovirus infection in an immunocompromised host. Pitfalls in diagnosis. Am J Med. 1987; 83:555–559.5. Ardehali H, Volmar K, Roberts C, Forman M, Becker LC. Fatal disseminated adenoviral infection in a renal transplant patient. Transplantation. 2001; 71:998–999.6. Klinger JR, Sanchez MP, Curtin LA, Durkin M, Matyas B. Multiple cases of life-threatening adenovirus pneumonia in a mental health care center. Am J Respir Crit Care Med. 1998; 157:645–649.7. Tate JE, Bunning ML, Lott L, Lu X, Su J, Metzgar D, et al. Outbreak of severe respiratory disease associated with emergent human adenovirus serotype 14 at a US air force training facility in 2007. J Infect Dis. 2009; 199:1419–1426.8. Bryant RE, Rhoades ER. Clinical features of adenoviral pneumonia in Air Force recruits. Am Rev Respir Dis. 1967; 96:717–723.9. Hwang SM, Park DE, Yang YI, Park SJ, Lee HK, Kim MJ, et al. Outbreak of febrile respiratory illness caused by adenovirus at a South Korean military training facility: clinical and radiological characteristics of adenovirus pneumonia. Jpn J Infect Dis. 2013; 66:359–365.10. Chong S, Lee KS, Kim TS, Chung MJ, Chung MP, Han J. Adenovirus pneumonia in adults: radiographic and high-resolution CT findings in five patients. AJR Am J Roentgenol. 2006; 186:1288–1293.11. Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med. 1994; 149(3 Pt 1):818–824.12. Montgomery EA, Popek EJ. Intussusception, adenovirus, and children: a brief reaffirmation. Hum Pathol. 1994; 25:169–174.13. Rheem I, Park J, Kim TH, Kim JW. Evaluation of a multiplex real-time PCR assay for the detection of respiratory viruses in clinical specimens. Ann Lab Med. 2012; 32:399–406.14. Mahony J, Chong S, Merante F, Yaghoubian S, Sinha T, Lisle C, et al. Development of a respiratory virus panel test for detection of twenty human respiratory viruses by use of multiplex PCR and a fluid microbead-based assay. J Clin Microbiol. 2007; 45:2965–2970.15. Paul NS, Roberts H, Butany J, Chung T, Gold W, Mehta S, et al. Radiologic pattern of disease in patients with severe acute respiratory syndrome: the Toronto experience. Radiographics. 2004; 24:553–563.16. Wong KT, Antonio GE, Hui DS, Lee N, Yuen EH, Wu A, et al. Thin-section CT of severe acute respiratory syndrome: evaluation of 73 patients exposed to or with the disease. Radiology. 2003; 228:395–400.17. Das KM, Lee EY, Enani MA, AlJawder SE, Singh R, Bashir S, et al. CT correlation with outcomes in 15 patients with acute Middle East respiratory syndrome coronavirus. AJR Am J Roentgenol. 2015; 204:736–742.18. Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology. 2008; 246:697–672.19. Ooi GC, Khong PL, Müller NL, Yiu WC, Zhou LJ, Ho JC, et al. Severe acute respiratory syndrome: temporal lung changes at thin-section CT in 30 patients. Radiology. 2004; 230:836–844.20. Dudding BA, Wagner SC, Zeller JA, Gmelich JT, French GR, Top FH Jr. Fatal pneumonia associated with adenovirus type 7 in three military trainees. N Engl J Med. 1972; 286:1289–1292.21. Zahradnik JM, Spencer MJ, Porter DD. Adenovirus infection in the immunocompromised patient. Am J Med. 1980; 68:725–732.22. Retalis P, Strange C, Harley R. The spectrum of adult adenovirus pneumonia. Chest. 1996; 109:1656–1657.23. Kang H, Lee KS, Jeong YJ, Lee HY, Kim KI, Nam KJ. Computed tomography findings of influenza A (H1N1) pneumonia in adults: pattern analysis and prognostic comparisons. J Comput Assist Tomogr. 2012; 36:285–290.24. Hakim FA, Tleyjeh IM. Severe adenovirus pneumonia in immunocompetent adults: a case report and review of the literature. Eur J Clin Microbiol Infect Dis. 2008; 27:153–158.25. Guo RF, Ward PA. Role of C5a in inflammatory responses. Annu Rev Immunol. 2005; 23:821–852.26. Wang R, Xiao H, Guo R, Li Y, Shen B. The role of C5a in acute lung injury induced by highly pathogenic viral infections. Emerg Microbes Infect. 2015; 4:e28.27. Tisoncik JR, Korth MJ, Simmons CP, Farrar J, Martin TR, Katze MG. Into the eye of the cytokine storm. Microbiol Mol Biol Rev. 2012; 76:16–32.28. Franquet T. Imaging of pulmonary viral pneumonia. Radiology. 2011; 260:18–39.29. Louie JK, Kajon AE, Holodniy M, Guardia-LaBar L, Lee B, Petru AM, et al. Severe pneumonia due to adenovirus serotype 14: a new respiratory threat? Clin Infect Dis. 2008; 46:421–425.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Successful Treatment in Fatal Adenovirus Pneumonia with the Use of Extracorporeal Membrane Oxygenation
- Acute Eosinophilic Pneumonia
- A Clinical Study on Acute Lower Respiratory Tract Infections by Adenovirus in Children
- A Clinical Study of Adenoviral Respiratory Infection in Children
- A Case of Parainfluenza Virus Related Acute Respiratory Distress Syndrome in Immune Competent Adult Patient: A Case Report
