Imaging Diagnosis and Management of Cystic Renal Masses: Introduction of an Update Proposal Bosniak Classification Version 2019
- Affiliations
-
- 1Department of Radiology, Chonnam National University Medical School, Chonnam National University Hwasun Hospital, Hwasun, Korea. sheo@jnu.ac.kr
- 2Department of Radiology, Chonnam National University Medical School, Chonnam National University Hospital, Gwangju, Korea.
- KMID: 2464905
- DOI: http://doi.org/10.3348/jksr.2019.80.6.1030
Abstract
- Cystic renal masses are commonly encountered in daily clinical practice. Improvements in the resolution of imaging modalities have led to an improved ability to detect cystic renal masses. It is important for radiologists to recognize and appropriately characterize cystic renal masses. Since 1986, the Bosniak classification system has been widely accepted for the evaluation of cystic renal masses, portions of which have been revised in 2019. Although the Bosniak classification system cannot fully differentiate aggressive lesions from indolent lesions, the system may help improve the specificity of detection for higher-risk classes for malignancy, increase the proportion of masses that are surveilled or ignored rather than resected, and select optimal management strategies.
MeSH Terms
Figure
-
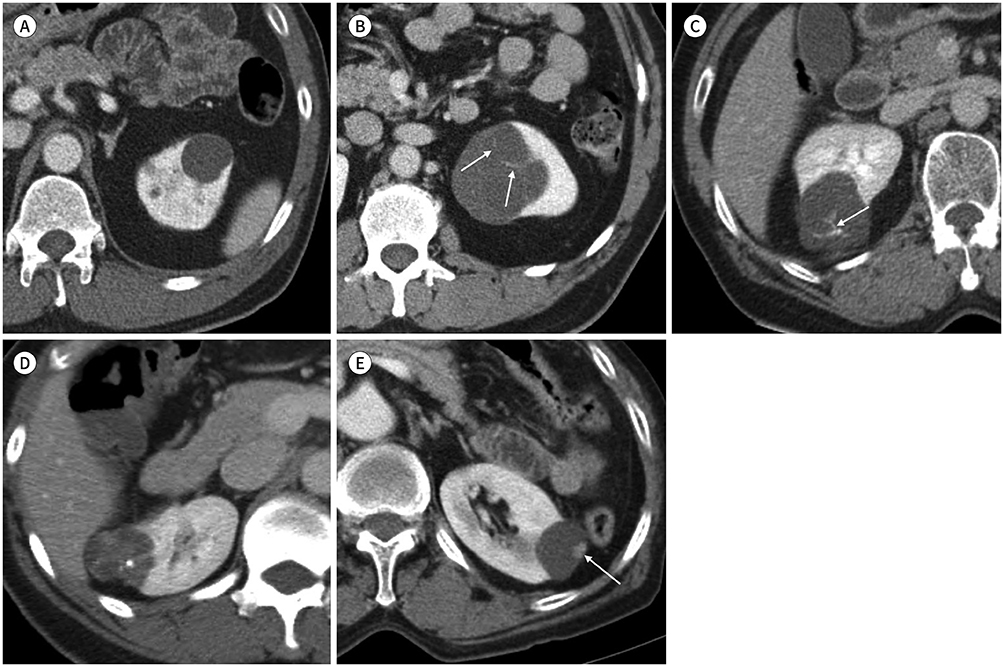
Fig. 1 Contrast-enhanced CT images of Bosniak classification of cystic renal masses. A. Class I simple cyst with homogeneous water attenuation density (0–20 Hounsfield unit) and no enhancement. B. Class II cyst with few hairline thin septa (arrows). C. Class IIF cystic mass with minimal smooth thickened septa and calcification (arrow). D. Class III cystic mass with thickened irregular septa and nodular calcification. E. Class IV cystic mass with mural enhancing soft tissue nodule (arrow).

Fig. 2 Drawings of the Bosniak classification version 2019. A. Class I. Well-defined cyst with thin (≤ 2 mm) smooth wall and homogeneous simple fluid (−9 to 20 HU on CT or SI similar to CSF); no septa or calcifications. B. Class II. Cystic mass with thin (≤ 2 mm) or few (1–3) enhancing septa; may have calcifications (green color) of any type; or homogeneous mass markedly hyperintense at T2WI (similar to CSF) or markedly hyperintense at T1WI (approximately × 2.5 normal parenchymal SI) at noncontrast MRI. C–E. Class IIF. Cystic masses with a smooth minimally thickened (3 mm) enhancing wall or smooth minimal thickening (3 mm) of one or more enhancing septa (C), or many (≥ 4) smooth thin (≤ 2 mm) enhancing septa (D) at CT or MRI; or heterogeneous hyperintensity at unenhanced fat-saturated T1WI (E). F. Class III. Cystic masses with one or more enhancing thick (≥ 4 mm) or enhancing irregular (≤ 3 mm obtusely margined convex protrusion[s]; blue color) walls or septa. G. Class IV. Cystic mass with one or more enhancing nodule(s) (≥ 4 mm convex protrusion with obtuse margins, or a convex protrusion of any size with acute margins; red color). CSF = cerebrospinal fluid, HU = Hounsfield unit, SI = signal intensity, T1WI = T1-weighted image, T2WI = T2-weighted image

Fig. 3 Cystic renal mass in a 44-year old man, which is initially classified Bosniak class IIF at CT and upgraded to Bosniak class III at MRI. A. Contrast-enhanced CT image shows a 2.5 cm Bosniak IIF cystic mass with multiple minimally smooth thickened septa in the right kidney. B, C. T2-weighted (B) and gadolinium-enhanced T1-weighted (C) MRI images show irregular thick septa (arrowheads) and some enhancing convex protrusions (arrows) within the cystic mass better than CT (A), being upgraded to Bosniak class III. The lesion was surgically resected and histopathological examination revealed multilocular cystic renal cell carcinoma.
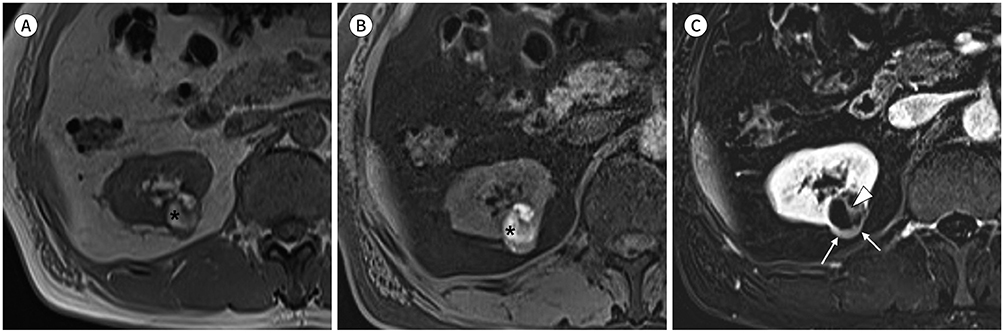
Fig. 4 Hemorrhagic cystic renal mass in a 58-year-old man. A, B. A 2.5 cm heterogeneous hyperintense mass (asterisks) both at in-phase T1-weighted (A) and unenhanced fat-saturated T1-weighted MR image (B) is seen in the right kidney. The hyperintense component is consistent with hemorrhage. C. Post-contrast subtraction image clearly shows the thick (≥ 4 mm) enhancing posterior wall (arrows) and thick (≥ 4 mm), irregular enhancing septum (arrowhead) of the mass, suggestive of Bosniak class III. The mass was resected and pathologically confirmed as a chromophobe renal cell carcinoma.

Fig. 5 Bosniak IIF cystic mass in the left kidney in a 49-year old man. A. Contrast-enhanced coronal CT image shows a 4 cm Bosniak IIF cystic mass in the upper pole of left kidney. B. At 18-month follow-up, number and thickening of the septa (arrows) within the cystic mass are increased, morphologic changes concerning for RCC. The mass was resected and pathologically confirmed as multilocular cystic RCC. RCC = renal cell carcinoma

Fig. 6 Bosniak IIF cystic mass in the right kidney in a 55-year old woman. A. A 3.5 cm cystic mass with multiple thin or minimal smooth thickened septa seen and considered to be Bosniak IIF. B. At 15-month follow-up, CT shows interval growth of the cystic mass from 3.5 cm to 4.5 cm. The mass was resected and pathologically confirmed as a benign multilocular cyst. Growth of a cystic mass without morphologic change is not indicative of malignancy.
Reference
-
1. Silverman SG, Israel GM, Herts BR, Richie JP. Management of the incidental renal mass. Radiology. 2008; 249:16–31.2. Hartman DS, Aronson S, Frazer H. Current status of imaging indeterminate renal masses. Radiol Clin North Am. 1991; 29:475–496.3. Tada S, Yamagishi J, Kobayashi H, Hata Y, Kobari T. The incidence of simple renal cyst by computed tomography. Clin Radiol. 1983; 34:437–439.4. Bosniak MA. The current radiological approach to renal cysts. Radiology. 1986; 158:1–10.5. Bosniak MA. Cystic renal masses: a reevaluation of the usefullness of the Bosniak Classification System. Acad Radiol. 1996; 3:981–984.6. Bosniak MA. The Bosniak renal cyst classification: 25 years later. Radiology. 2012; 262:781–785.7. Israel GM, Silverman SG. The incidental renal mass. Radiol Clin North Am. 2011; 49:369–383.8. Hindman NM. Cystic renal masses. Abdom Radiol (NY). 2016; 41:1020–1034.9. Hindman NM. Imaging of cystic renal masses. Urol Clin North Am. 2018; 45:331–349.10. Ward RD, Remer EM. Cystic renal masses: an imaging update. Eur J Radiol. 2018; 99:103–110.11. Sanz E, Hevia V, Gómez V, Álvarez S, Fabuel JJ, Martínez L, et al. Renal complex cystic masses: usefulness of contrast-enhanced ultrasound (CEUS) in their assessment and its agreement with computed tomography. Curr Urol Rep. 2016; 17:89.12. Graumann O, Osther SS, Karstoft J, Hørlyck A, Osther PJ. Bosniak classification system: a prospective comparison of CT, contrast-enhanced US, and MR for categorizing complex renal cystic masses. Acta Radiol. 2016; 57:1409–1417.13. Chen Y, Wu N, Xue T, Hao Y, Dai J. Comparison of contrast-enhanced sonography with MRI in the diagnosis of complex cystic renal masses. J Clin Ultrasound. 2015; 43:203–209.14. Quaia E, Bertolotto M, Cioffi V, Rossi A, Baratella E, Pizzolato R, et al. Comparison of contrast-enhanced sonography with unenhanced sonography and contrast-enhanced CT in the diagnosis of malignancy in complex cystic renal masses. AJR Am J Roentgenol. 2008; 191:1239–1249.15. Park BK, Kim B, Kim SH, Ko K, Lee HM, Choi HY. Assessment of cystic renal masses based on Bosniak classification: comparison of CT and contrast-enhanced US. Eur J Radiol. 2007; 61:310–314.16. Bertolotto M, Bucci S, Valentino M, Currò F, Sachs C, Cova MA. Contrast-enhanced ultrasound for characterizing renal masses. Eur J Radiol. 2018; 105:41–48.17. Ascenti G, Mazziotti S, Zimbaro G, Settineri N, Magno C, Melloni D, et al. Complex cystic renal masses: characterization with contrast-enhanced US. Radiology. 2007; 243:158–165.18. Xu Y, Zhang S, Wei X, Pan Y, Hao J. Contrast enhanced ultrasonography prediction of cystic renal mass in comparison to histopathology. Clin Hemorheol Microcirc. 2014; 58:429–438.19. O’Malley RL, Godoy G, Hecht EM, Stifelman MD, Taneja SS. Bosniak category IIF designation and surgery for complex renal cysts. J Urol. 2009; 182:1091–1095.20. Hindman NM, Hecht EM, Bosniak MA. Follow-up for Bosniak category 2F cystic renal lesions. Radiology. 2014; 272:757–766.21. Cloix P, Martin X, Pangaud C, Maréchal JM, Bouvier R, Barat D, et al. Surgical management of complex renal cysts: a series of 32 cases. J Urol. 1996; 156:28–30.22. Curry NS, Cochran ST, Bissada NK. Cystic renal masses: accurate Bosniak classification requires adequate renal CT. AJR Am J Roentgenol. 2000; 175:339–342.23. Smith AD, Remer EM, Cox KL, Lieber ML, Allen BC, Shah SN, et al. Bosniak category IIF and III cystic renal lesions: outcomes and associations. Radiology. 2012; 262:152–160.24. Reese AC, Johnson PT, Gorin MA, Pierorazio PM, Allaf ME, Fishman EK, et al. Pathological characteristics and radiographic correlates of complex renal cysts. Urol Oncol. 2014; 32:1010–1016.25. Smith AD, Allen BC, Sanyal R, Carson JD, Zhang H, Williams JH, et al. Outcomes and complications related to the management of Bosniak cystic renal lesions. AJR Am J Roentgenol. 2015; 204:W550–W556.26. Mousessian PN, Yamauchi FI, Mussi TC, Baroni RH. Malignancy rate, histologic grade, and progression of Bosniak category III and IV complex renal cystic lesions. AJR Am J Roentgenol. 2017; 209:1285–1290.27. Campbell S, Uzzo RG, Allaf ME, Bass EB, Cadeddu JA, Chang A, et al. Renal mass and localized renal cancer: AUA guideline. J Urol. 2017; 198:520–529.28. Silverman SG, Pedrosa I, Ellis JH, Hindman NM, Schieda N, Smith AD, et al. Bosniak classification of cystic renal masses, version 2019: an update proposal and needs assessment. Radiology. 2019; 292:475–488.29. Graumann O, Osther SS, Karstoft J, Hørlyck A, Osther PJ. Bosniak classification system: inter-observer and intra-observer agreement among experienced uroradiologists. Acta Radiol. 2015; 56:374–383.30. Pedrosa I, Sun MR, Spencer M, Genega EM, Olumi AF, Dewolf WC, et al. MR imaging of renal masses: correlation with findings at surgery and pathologic analysis. Radiographics. 2008; 28:985–1003.31. Dilauro M, Quon M, McInnes MD, Vakili M, Chung A, Flood TA, et al. Comparison of contrast-enhanced multiphase renal protocol CT versus MRI for diagnosis of papillary renal cell carcinoma. AJR Am J Roentgenol. 2016; 206:319–325.32. Israel GM, Bosniak MA. Follow-up CT of moderately complex cystic lesions of the kidney (Bosniak category IIF). AJR Am J Roentgenol. 2003; 181:627–633.33. Davarpanah AH, Spektor M, Mathur M, Israel GM. Homogeneous T1 hyperintense renal lesions with smooth borders: is contrast-enhanced MR imaging needed? Radiology. 2016; 280:128–136.34. Agochukwu N, Huber S, Spektor M, Goehler A, Israel GM. Differentiating renal neoplasms from simple cysts on contrast-enhanced CT on the basis of attenuation and homogeneity. AJR Am J Roentgenol. 2017; 208:801–804.35. Kim CW, Shanbhogue KP, Schreiber-Zinaman J, Deng FM, Rosenkrantz AB. Visual assessment of the intensity and pattern of T1 hyperintensity on MRI to differentiate hemorrhagic renal cysts from renal cell carcinoma. AJR Am J Roentgenol. 2017; 208:337–342.36. Herts BR, Silverman SG, Hindman NM, Uzzo RG, Hartman RP, Israel GM, et al. Management of the incidental renal mass on CT: a white paper of the ACR Incidental Findings Committee. J Am Coll Radiol. 2018; 15:264–273.37. Kashan M, Ghanaat M, Hötker AM, Duzgol C, Sanchez A, DiNatale RG, et al. Cystic renal cell carcinoma: a report on outcomes of surgery and active surveillance in patients retrospectively identified on pretreatment imaging. J Urol. 2018; 200:275–282.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Clinical Significance of Bosniak Classification in Cystic Renal Masses : Usefulness of Preoperative Computerized Tomography in Cystic Renal Masses
- Usefulness of the Bosniak Classification in Cystic Renal Mass on CT
- Assessment of Cystic Renal Masses Based on Bosniak Classification: Comparison of CT, Contrast-enhanced US, and MR Imaging
- Multislice computed tomography/contrast-enhanced ultrasound image fusion as a tool for evaluating unclear renal cysts
- Differential Diagnosis of Complex Renal Cysts Based on Lesion Size along with the Bosniak Renal Cyst Classification
