Clinical Features and Treatment Outcomes of Acute Multiple Thoracic and Lumbar Spinal Fractures: A Comparison of Continuous and Noncontinuous Fractures
- Affiliations
-
- 1Department of Neurosurgery, Ewha Womans University College of Medicine, Seoul, Korea. yongcho@ewha.ac.kr
- KMID: 2463662
- DOI: http://doi.org/10.3340/jkns.2019.0093
Abstract
OBJECTIVE
The treatment of multiple thoracolumbar spine fractures according to fracture continuity has rarely been reported. Herein we evaluate the clinical features and outcomes of multiple thoracolumbar fractures depending on continuous or noncontinuous status.
METHODS
From January 2010 to January 2016, 48 patients with acute thoracic and lumbar multiple fractures who underwent posterior fusion surgery were evaluated. Patients were divided into two groups (group A : continuous; group B : noncontinuous). We investigated the causes of the injuries, the locations of the injuries, the range of fusion levels, and the functional outcomes based on the patients' general characteristics.
RESULTS
A total of 48 patients were enrolled (group A : 25 patients; group B : 23 patients). Both groups had similar pre-surgical clinical and radiologic features. The fusion level included three segments (group A : 4; group B : 5) or four segments (group A : 19; group B : 5). Group B required more instrumented segments than did group A. Group A scored 23.5 and group B scored 33.4 on the Korean Oswestry Disability Index (KODI) at the time of last follow-up. In both groups, longer fusion was associated with worse KODI score.
CONCLUSION
In this study, due to the assumption of similar initial clinical and radiologic features in both group, the mechanism of multiple fractures is presumed to be the same between continuous and noncontinuous fractures. The noncontinuous fracture group had worse KODI scores in long-term follow-up, thought to be due to long fusion level. Therefore, we recommend minimizing the number of segments that are fused in multiple thoracolumbar and lumbar fractures when decompression is not necessary.
Keyword
Figure
-
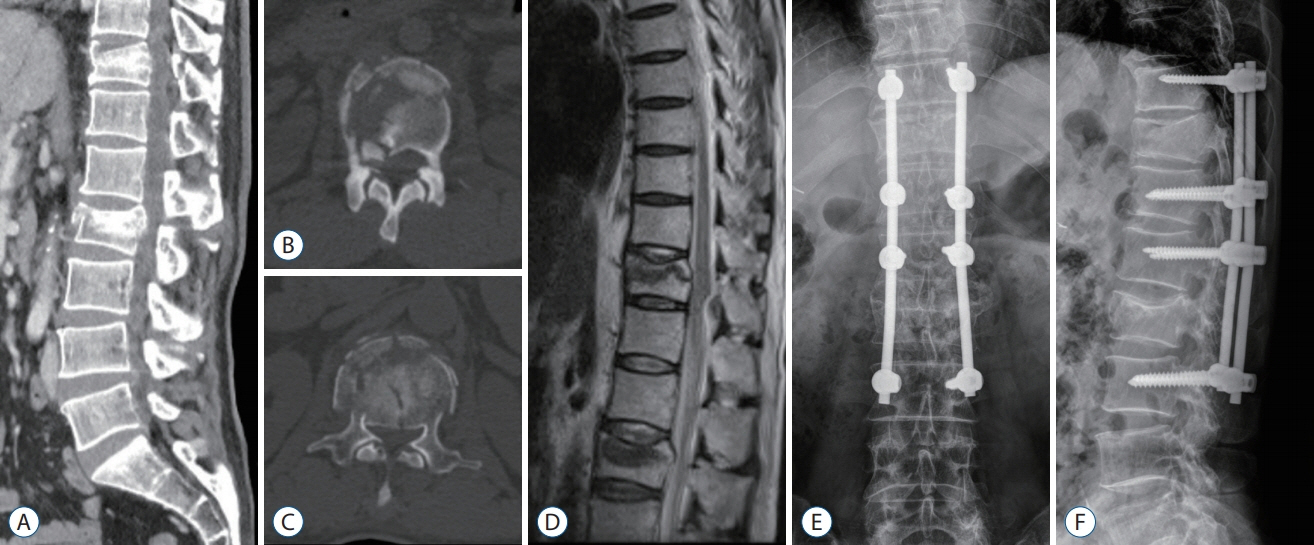
Fig. 1. A 32-year-old man with noncontinous thoracolumbar fractures. He fell from the second floor and the physical exam at the emergency department showed motor grade II below the L2 level and a tingling sensation in both lower limbs. A-C : A lumbar CT shows fractures on the T11 and L2 vertebral bodies. Axial CT scan shows severe canal compromise at both T11 and L2. D : MR sagittal scan demonstrates spinal canal compromise. E and F : Instrumentation and posterolateral fusion of T10–L3 with posterior decompression of L2 was performed. T11 fracture had spinous process fracture and then we included T11 into instrumented level. CT : computed tomography, MR : magnetic resonance.
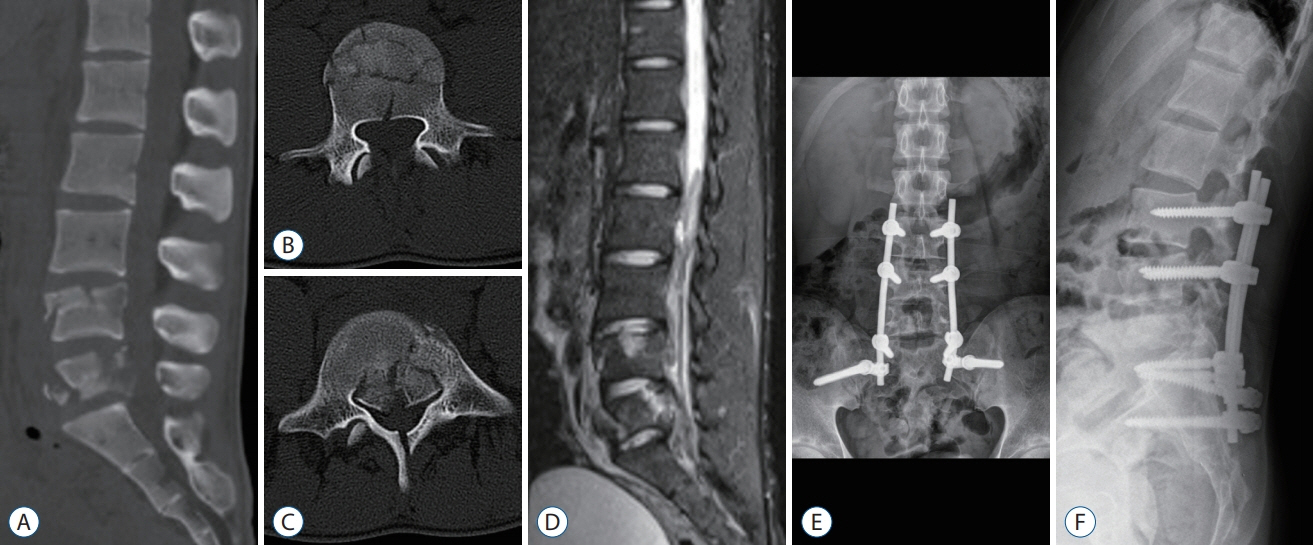
Fig. 2. A 20-year-old man with continous thoracolumbar fractures. He injured from traffic accident. The physical exam at the emergency department showed motor grade III below the L4 level and a tingling sensation in both lower limbs. A-C : A lumbar CT and MRI show stable burst fracture and unstable burst fractures on the L4, L5 on each other. Axial CT scan shows severe canal compromise at L5. D : MR sagittal T2 scan demonstrates cauda equina compression and instability. E and F : Instrumentation from L3 to pelvis and posterolateral fusion with posterior decompression of L5 was performed. We could reduce instrumentation level by inserting screws into L4 fractured vertebral body. CT : computed tomography, MR : magnetic resonance, MRI : magnetic resonance imaging.
Reference
-
References
1. Calenoff L, Chessare JW, Rogers LF, Toerge J, Rosen JS. Multiple level spinal injuries: importance of early recognition. AJR Am J Roentgenol. 130:665–669. 1978.
Article2. Chen F, Kang Y, Li H, Lv G, Lu C, Li J, et al. Treatment of lumbar split fracture-dislocation with short-segment or long-segment posterior fixation and anterior fusion. Clin Spine Surg. 30:E310–E316. 2017.
Article3. Dai LY, Jia LS. Multiple non-contiguous injuries of the spine. Injury. 27:573–575. 1996.
Article4. Guven O, Kocaoglu B, Bezer M, Aydin N, Nalbantoglu U. The use of screw at the fracture level in the treatment of thoracolumbar burst fractures. J Spinal Disord Tech. 22:417–421. 2009.
Article5. Hebert JS, Burnham RS. The effect of polytrauma in persons with traumatic spine injury. A prospective database of spine fractures. Spine (Phila Pa 1976). 25:55–60. 2000.6. Heidari P, Zarei MR, Rasouli MR, Vaccaro AR, Rahimi-Movaghar V. Spinal fractures resulting from traumatic injuries. Chin J Traumatol. 13:3–9. 2010.7. Henderson RL, Reid DC, Saboe LA. Multiple noncontiguous spine fractures. Spine (Phila Pa 1976). 16:128–131. 1991.
Article8. Jo DJ, Kim SM, Kim KT, Seo EM. Surgical experience of neglected lower cervical spine fracture in patient with ankylosing spondylitis. J Korean Neurosurg Soc. 48:66–69. 2010.
Article9. Kano S, Tanikawa H, Mogami Y, Shibata S, Takanashi S, Oji Y, et al. Comparison between continuous and discontinuous multiple vertebral compression fractures. Eur Spine J. 21:1867–1872. 2012.
Article10. Kerttula LI, Serlo WS, Tervonen OA, Pääkkö EL, Vanharanta HV. Posttraumatic findings of the spine after earlier vertebral fracture in young patients: clinical and MRI study. Spine (Phila Pa 1976). 25:1104–1108. 2000.
Article11. Kim DY, Lee SH, Lee HY, Lee HJ, Chang SB, Chung SK, et al. Validation of the Korean version of the oswestry disability index. Spine (Phila Pa 1976). 30:E123–E127. 2005.
Article12. Knop C, Oeser M, Bastian L, Lange U, Zdichavsky M, Blauth M. Development and validation of the visual analogue scale (VAS) spine score. Unfallchirurg. 104:488–497. 2001.13. Korres DS, Boscainos PJ, Papagelopoulos PJ, Psycharis I, Goudelis G, Nikolopoulos K. Multiple level noncontiguous fractures of the spine. Clin Orthop Relat Res. 95–102. 2003.
Article14. Korres DS, Katsaros A, Pantazopoulos T, Hartofilakidis-Garofalidis G. Double or multiple level fractures of the spine. Injury. 13:147–152. 1981.
Article15. Lian XF, Zhao J, Hou TS, Yuan JD, Jin GY, Li ZH. The treatment for multilevel noncontiguous spinal fractures. Int Orthop. 31:647–652. 2007.
Article16. Liu Z, Zhang P, Zeng H, Xu Z, Wang X. A comparative study of singlestage transpedicular debridement, fusion, and posterior long-segment versus short-segment fixation for the treatment of thoracolumbar spinal tuberculosis in adults: minimum five year follow-up outcomes. Int Orthop. 42:1883–1890. 2018.
Article17. McAfee PC, Yuan HA, Fredrickson BE, Lubicky JP. The value of computed tomography in thoracolumbar fractures. An analysis of one hundred consecutive cases and a new classification. J Bone Joint Surg Am. 65:461–473. 1983.
Article18. McLain RF. The biomechanics of long versus short fixation for thoracolumbar spine fractures. Spine (Phila Pa 1976). 31:S70–S79. discussion S104. 2006.
Article19. Niedermeier SR, Khan SN. Polytrauma patients with associated spine fractures: an assessment of surgical intervention on patient outcome. Clin Spine Surg. 30:E38–E43. 2017.20. Powell JN, Waddell JP, Tucker WS, Transfeldt EE. Multiple-level noncontiguous spinal fractures. J Trauma. 29:1146–1150. discussion 1150-1151. 1989.
Article21. Ruan DK. Fixation for the thoracolumbar spine fracture: long-segment versus short-segment. Zhongguo Gu Shang. 22:483–484. 2009.22. Seçer M, Alagöz F, Uçkun O, Karakoyun OD, Ulutas MÖ, Polat Ö, et al. Multilevel noncontiguous spinal fractures: surgical approach towards clinical characteristics. Asian Spine J. 9:889–894. 2015.
Article23. Wittenberg RH, Hargus S, Steffen R, Muhr G, Bötel U. Noncontiguous unstable spine fractures. Spine (Phila Pa 1976). 27:254–257. 2002.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Multiple Thoracolumbar and Lumbar Spine Fractures: Comparison of Contiguous and Non-Contiguous Fractures in Non-Osteoporotic Patients
- The Value of Radionuclide Imaging as a Screening Test for the Diagnosis of an Acute Thoracic Spinal Fractures
- The Usefulness of Bone Scan in the Osteoporotic Vertebral Compression Fracture Patients Treated With Kyphoplasty
- Multiple Fractures in Thoracic Vertebrae after Epilepsy
- Treatment of a 3rd Lumbar Vertebra Translational Injury Combined with Incomplete Cauda Equina Syndrome in Ankylosing Spondylitis: A Case Report
