Intrusion of the extruded maxillary central incisor using skeletal anchorage system and unilateral segmental intrusion arch
- Affiliations
-
- 1Dental Clinic Center, Pusan National University Hosptial, Busan, Republic of Korea. youngyng@hanmail.net
- 2Department of Orthodontics, School of Dentistry, Pusan National University, Yangsan, Republic of Korea.
- KMID: 2463627
- DOI: http://doi.org/10.14368/jdras.2019.35.3.180
Abstract
- Patients who have a moderate periodontitis with pathologic tooth migration of maxillary incisors, it is necessary not only periodontal treatment for reduce periodontal inflammation, but also orthodontic treatment to teeth repositioning. For orthodontic treatment, it is necessary to apply less force and careful considerations of the center of resistance of the tooth and optimal force of tooth movement. At this time, the segmental arch applied only to the target teeth, is more effective and predictable, because applied force and direction can be controlled. In addition, to design the orthodontic appliance that can prevent the unwanted tooth movement that used as an anchorage is important. In recent years, various types of skeletal anchorage system have been used for preventing loss of the anchorage. We reported the patient who had extruded maxillary central incisor due to pathologic tooth migration, treated by a successful periodontal-orthodontic multidisciplinary treatment using an orthodontic appliance designed to apply less traumatic force and reduce an anchorage loss.
MeSH Terms
Figure
-
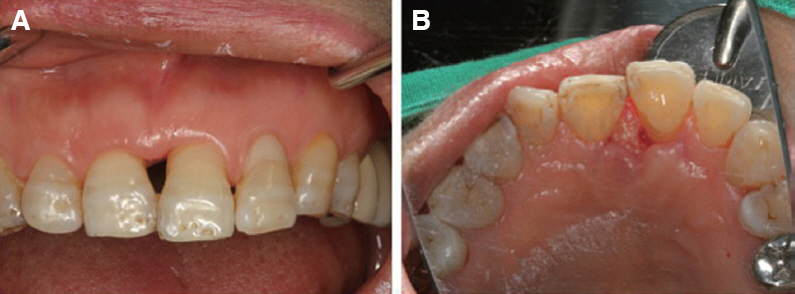
Fig. 1 Pre-treatment intraoral photographs. (A) #21 was extruded. Large black triangle was observed between #11 and #21, (B) #21 was protruded.
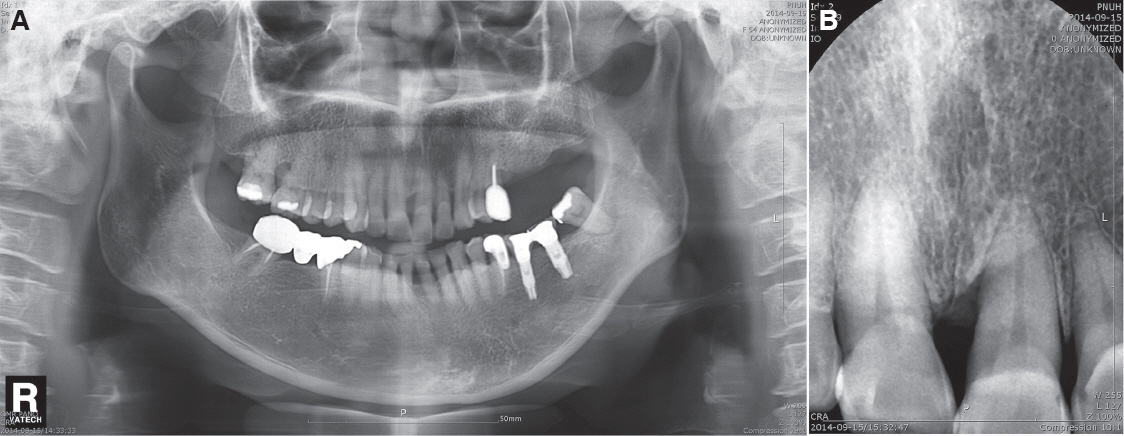
Fig. 2 Pre-treatment panoramic (A) and periapical (B) radiographs. (A) Generalized alveolar bone loss was observed. #26 and #27 were extracted, (B) Angular alveolar bone loss was observed on the mesial root surface of # 21.

Fig. 3 Procedure of periodontal surgery with bone graft. (A) Deep periodontal pocket and alveolar bone loss were observed, (B) Flap design to preserve interdental papilla was designed, (C) During periodontal surgery, bovine bone graft (Bio-Oss®) materials were used for bone graft.

Fig. 4 Intraoral photograph before orthodontic treatment (3 months after periodontal surgery).
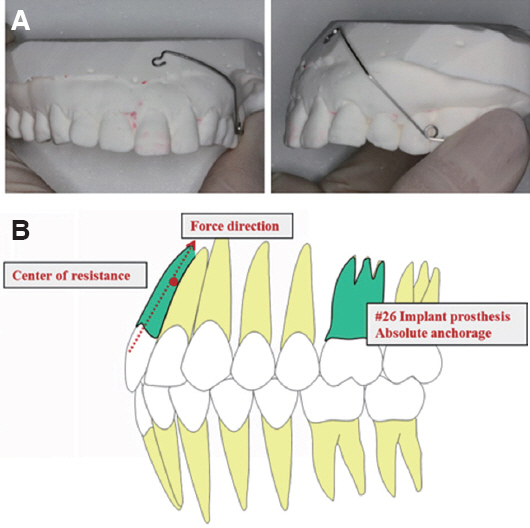
Fig. 5 Segmental intrusion arch design. (A) 0.016 × 0.025-inch TMA wire was used for segmental intrusion arch, (B) The segmental intrusion arch was designed to allow the force to pass through the center of resistance of #21.

Fig. 6 Intraoral photographs of orthodontic treatment (initiation, bracket bonding). The segmental intrusion arch was applied to #21 and 26. The segmental intrusion arch was activated and pulled toward bracket to apply a force of 12 gm.

Fig. 7 Progression of orthodontic treatment (during 5 months). #21 was gradually intruded by segmental intrusion arch.

Fig. 8 Post-orthodontic treatment (bracket removal) intraoral photographs. #21 was intruded and retracted. Fixed retainer was placed on maxilla anterior teeth (#13-23).
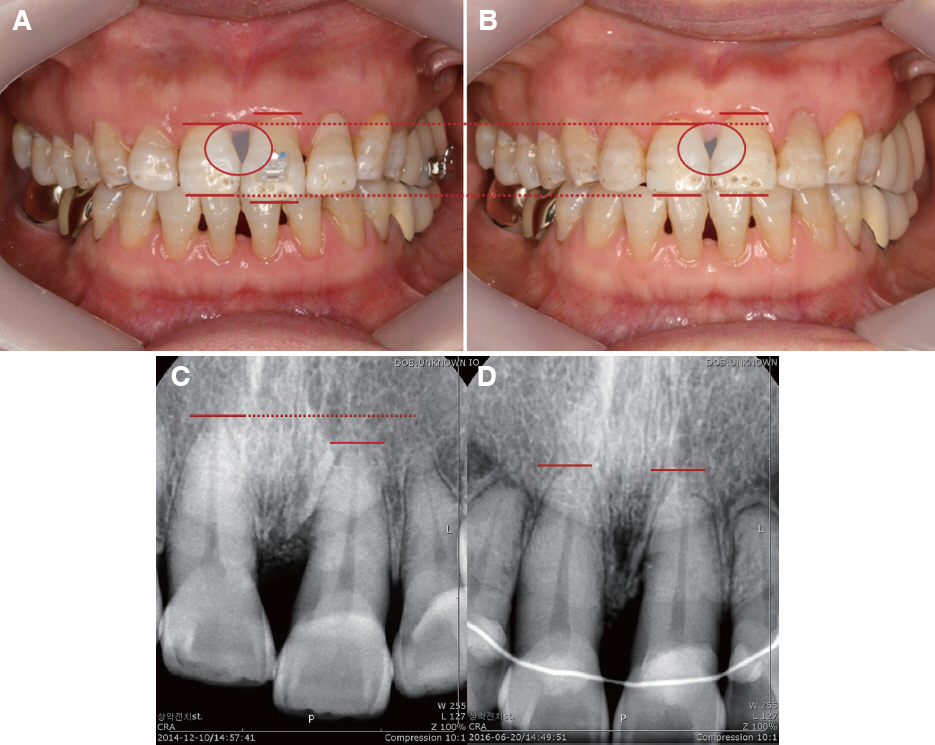
Fig. 9 Comparisons of pre-treatment (A, C) and post-treatment (B, D). (A, B) Intraoral photographs. #21 was intruded. The gingival margin of #21 was maintained during orthodontic treatment and black triangle between #11 and #21 was reduced. (C, D) Periapical radiographs. After orthodontic treatment, #21 was intruded.

Fig. 10 Intraoral photographs (A) and periapical radiograph (B) for 4-year retention period
Reference
-
References
1. Disease Statistics. Healthcare Bigdata Hub. Wonju: Healthcare Insurance Review & Assessment Service;Available from: http://opendata.hira.or.kr/op/opc/olapHifrqSickInfo.do. (updated 2019 May 24).2. Melsen B. Adult Orthodontics:Aetiology. 3rd ed. West Sussex: Wiley-Blackwell;2012. p. 48–50. DOI: 10.1002/9781118702925.3. Proffit WR, Field HW, Sarver DM. Contemporary Orthodontics. 4th ed. New York: Elsevier;2007. p. 142–4.4. Towfighi PP, Brunsvold MA, Storey AT, Arnold RM, Willman DE, McMaham CA. Pathologic migration of anterior teeth in patients with moderate to severe periodontitis. J Periodontol. 1997; 68:967–72. DOI: 10.1902/jop.1997.68.10.967. PMID: 9358363.5. Artun J, Urbye KS. The effect of orthodontic treatment on periodontal bone support in patients with advanced loss of marginal periodontium. Am J Orthod Dentofac Orthop. 1988; 93:143–8. DOI: 10.1016/0889-5406(88)90292-2. PMID: 3422529.6. Melsen B, Agerbaek N, Erikson J, Terp S. New attachment through periodontal treatment and orthodontic intrusion. Am J Orthod Dentofac Orthop. 1988; 94:104–16. DOI: 10.1016/0889-5406(88)90358-7. PMID: 3165238.7. Erkan M, Pikdoken L, Usumez S. Gingival response to mandibular incisor intrusion. Am J Orthod Dentofacial Orthop. 2007; 132:143.e9–13. DOI: 10.1016/j.ajodo.2006.10.015. PMID: 17693359.8. Ericsson I, Thilander B, Lindhe J, Okamoto H. The effect of orthodontic tilting movements on the periodontal tissures of infected and non-infected dentitions in dogs. J Clin Periodontol. 1977; 4:278–93. DOI: 10.1111/j.1600-051X.1977.tb01900.x. PMID: 271655.9. Melsen B, Agerbaek N, Markenstam G. Intrusion of incisors in adult patients with marginal bone loss. Am J Orthod Dentofacial Orthop. 1989; 96:232–41. DOI: 10.1016/0889-5406(89)90460-5. PMID: 2773869.10. Ryph P. Ultrastructural vascular changes in pressure zones of rat molar periodontium incident to orthodontic movement. Scand J Dent Res. 1972; 80:307–21. DOI: 10.1111/j.1600-0722.1972.tb00296.x. PMID: 4115917.11. Weltman B, Vig KW, Fields HW, Shanker S, Kaizar EE. Root resorption associated with orthodontic tooth movement:a systematic review. Am J Orthod Dentofacial Orthop. 2010; 137:462–76. DOI: 10.1016/j.ajodo.2009.06.021. PMID: 20362905.12. Mostafa YA, Iskander KG, El-Mangoury NH. Iatrogenic pulpal reactions to orthodontic extrusion. Am J Orthod Dentofac Orthop. 1991; 99:30–4. DOI: 10.1016/S0889-5406(05)81677-4. PMID: 1986523.13. Steigman S, Michaeli Y. Experimental intrusion of rat incisors with continuous loads of varying magnitude. Am J Orthod. 1981; 80:429–36. DOI: 10.1016/0002-9416(81)90177-9. PMID: 6945811.14. Thilander B. Orthodontic tooth movement in periodontal therapy. Textbook of Clinical Periodontology. Copenhagen: Munksgaard;1989. p. 450–500.15. Alstad S, Zachrisson BU. Longitudinal study of periodontal condition associated with orthodontic treatment in adolescents. Am J Orthod. 1979; 76:277–86. DOI: 10.1016/0002-9416(79)90024-1. PMID: 290273.16. Re S, Corrente G, Abundo R, Cardaropoli D. Orthodontic treatment in periodontally compromised patients:12-year report. Int J Periodontics Restorative Dent. 2000; 20:31–9. PMID: 11203546.17. Burstone CJ, Goldberg AJ. Maximum forces and deflections from orthodontic appliances. Am J Orthod. 1983; 84:95–103. DOI: 10.1016/0002-9416(83)90173-2. PMID: 6576645.18. Burstone CR. Deep overbite correction by intrusion. Am J Orthod. 1977; 72:1–22. DOI: 10.1016/0002-9416(77)90121-X. PMID: 267433.19. Reitan K. Tissue rearrangement during retention of orthodontically rotated teeth. Angle Orthod. 1959; 29:105–13.20. Ericsson I, Thilander B. Orthodontic relapse in dentitions with reduced periodontal support:an experimental study in dogs. Eur J Orthod. 1980; 2:51–7. DOI: 10.1093/ejo/2.1.51. PMID: 6935058.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intrusion Of The Severe Extruded Maxillary Post.Teeth Using Post.Segmental Osteotomy And Orthodontic Treatment With Skeletal Anchorage System: Cases Report
- Nonextraction treatment of Class II division 2 in an adult patient using microimplant anchorage (MIA)
- Evaluation of changes in the maxillary alveolar bone after incisor intrusion
- A study on the treatment of anterior open bite with midpalatal miniscrews
- Orthodontic intrusion treatment of mandibular anterior teeth in a periodontal patient with hyperdivergent skeletal pattern: 8-year follow-up
