Infectious Crystalline Keratopathy Caused by Alternaria
- Affiliations
-
- 1Department of Ophthalmology, Daegu Fatima Hospital, Daegu, Korea. dj_oph_2540@hanmail.net
- KMID: 2463363
- DOI: http://doi.org/10.3341/jkos.2019.60.11.1112
Abstract
- PURPOSE
To report a case of infectious crystalline keratopathy caused by Alternaria in the corneal center.
CASE SUMMARY
A 66-year-old male visited our clinic with right ocular pain and visual loss after corneal trauma caused by a foreign body hitting his right eye while performing farm work 1 month prior to his visit. The patient had no history of corneal surgery and long-term use of topical corticosteroid. A corneal epithelial defect and whitish snowflake margin infiltration around the corneal stroma were observed in the corneal center, but there was an absence of conjunctival injection and anterior segment inflammation. Cultures and a biopsy of the corneal scrapings revealed Alternaria species fungus. The patient was treated with 1% topical voriconazole and 0.5% moxifloxacin, together with oral voriconazole (400 mg/day). After 2 months of treatment, the disease was completely cured, with a minute corneal opacity.
CONCLUSIONS
We successfully treated a rare case of infectious crystalline keratopathy caused by Alternaria, which has not been previously reported in the Republic of Korea.
MeSH Terms
Figure
-
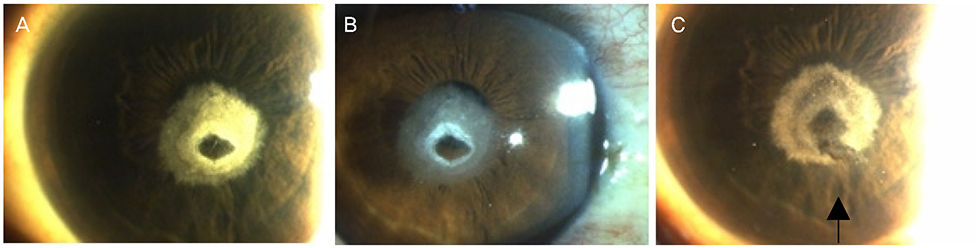
Figure 1 Slit-lamp photography of the right eye at the initial examination. (A) The right eye shows whitish snowflake-like margin of stromal infiltration. (B) Absence of corneal and anterior segment inflammation. (C) Corneal surface of the right eye after corneal biopsy (arrow).
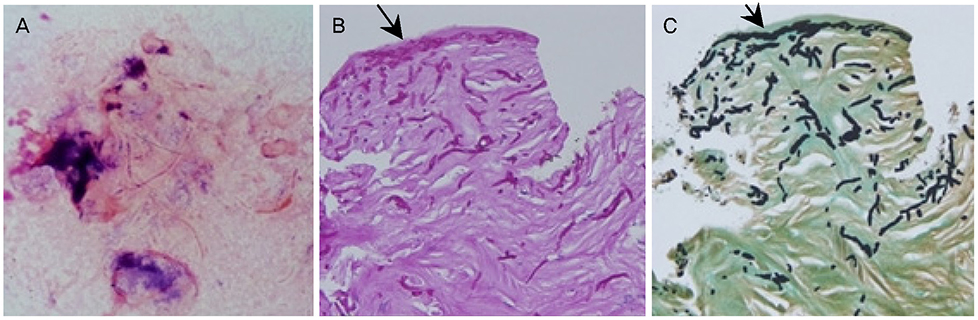
Figure 2 Pathology slides of the corneal tissue. (A) The KOH mount & Gram stain showed plenty of septate hyphae. (B) Corneal biopsy. The organisms stained positive with Periodic acid Schiff (PAS). PAS stain revealed the microbial colonies aggregated in the stroma (arrow). (C) Corneal biopsy. The organisms stained positive with Grocott's methenamine silver (GMS). GMS stain revealed the microbial colonies aggregated in the stroma (arrow). Original magnification (×200).
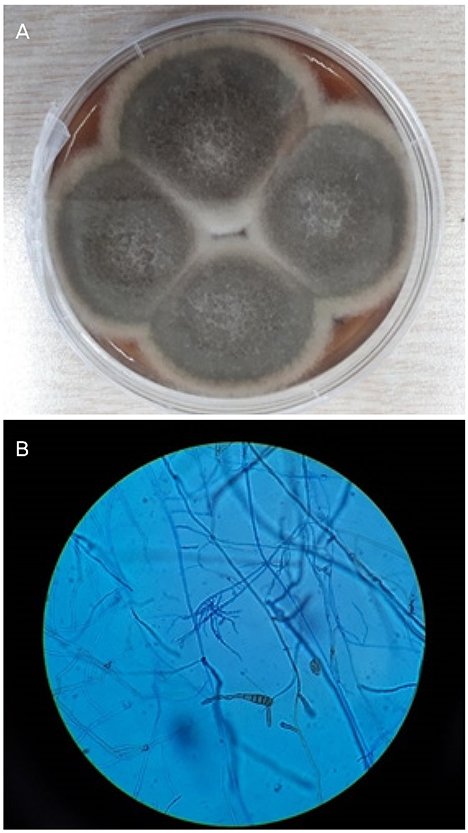
Figure 3 Photograph of Alternaria species cultured on Sabouraud dextrose agar plate (A), stained with lactophenol cotton blue (B). (A) Sabouraud dextrose agar plate Alternaria species showed typical darkly pigmented (dematiaceous) feathery-like light gray colony. (B) On staining with lactophenol cotton blue, branched acropetal chain and macroconidium were seen.
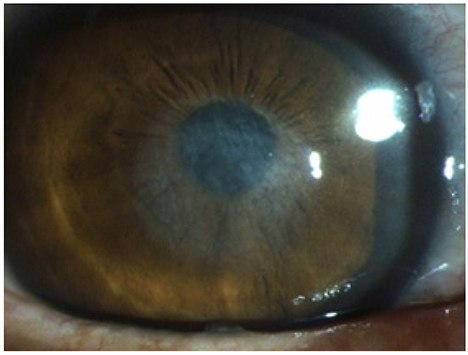
Figure 4 Slit-lamp photography of the right eye 2 months after treatment. The disease was completely cured, with a minute corneal opacity.
Reference
-
1. Stern GA. Infectious crystalline keratopathy. Int Ophthalmol Clin. 1993; 33:1–7.2. Porter AJ, Lee GA, Jun AS. Infectious crystalline keratopathy. Surv Ophthalmol. 2018; 63:480–499.3. Christakopoulos CE, Prause JU, Heegaard S. Infectious crystalline keratopathy histopathological characteristics. Acta Ophthalmol Scand. 2003; 81:659–661.4. Bispo PJM, Haas W, Gilmore MS. Biofilms in infections of the eye. Pathogens. 2015; 4:111–136.5. Hunts JH, Matoba AY, Osato MS, Font RL. Infectious crystalline keratopathy. the role of bacterial exopolysaccharide. Arch Ophthalmol. 1993; 111:528–530.6. Verma K, Vajpayee RB, Titiyal JS, et al. Post-LASIK infectious crystalline keratopathy caused by Alternaria. Cornea. 2005; 24:1018–1020.7. Gorovoy MS, Stern GA, Hood I, Allen C. Intrastromal noninflammatory bacterial colonization of a corneal graft. Arch Ophthalmol. 1983; 101:1749–1752.8. Meisler DM, Langston RHS, Naab TJ, et al. Infectious crystalline keratopathy. Am J Ophthalmol. 1984; 97:337–343.9. You IC, Kang IS, Yoon KC. Clinical aspect and prognosis of alternaria keratitis. J Korean Ophthalmol Soc. 2007; 48:478–484.10. Rhem MN, Wilhelmus KR, Font RL. Infectious crystalline keratopathy caused by Candida parapsilosis. Cornea. 1996; 15:543–545.11. Ainbinder DJ, Parmley VC, Mader TH, Nelson ML. Infectious crystalline keratopathy caused by Candida guilliermondii. Am J Ophthalmol. 1998; 125:723–725.12. Elder MJ, Matheson M, Stapleton F, Dart JK. Biofilm formation in infectious crystalline keratopathy due to Candida albicans. Cornea. 1996; 15:301–304.13. Pastor FJ, Guarro J. Alternaria infections: laboratory diagnosis and relevant clinical features. Clin Microbiol Infect. 2008; 14:734–746.14. Khan IJ, Hamada S, Rauz S. Infectious crystalline keratopathy treated with intrastromal antibiotics. Cornea. 2010; 29:1186–1188.15. Daneshvar H, MacInnis B, Hodge WG. Nd:YAG laser corneal disruption as adjuvant treatment for infectious crystalline keratopathy. Am J Ophthalmol. 2000; 129:800–801.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Occupational Asthma Caused by Alternaria Species
- Retinopathy and Keratopathy Associated with Chronic Tamoxifen Medication
- A Case of Crystalline Keratopathy in Monoclonal Gammopathy of Undetermined Significance (MGUS)
- Taxonomic Studies on Alternaria in Korea (1)
- First Report of Black Spot Disease Caused by Alternaria alternata on Sweet Persimmon Fruits
