Clin Orthop Surg.
2019 Dec;11(4):466-473. 10.4055/cios.2019.11.4.466.
Alpha Angle as a Predictor of Impending Contralateral Slipped Capital Femoral Epiphysis in an Asian Population
- Affiliations
-
- 1Department of Orthopaedic Surgery, KK Women's and Children's Hospital, Singapore. chloe.chan@mohh.com.sg
- KMID: 2462542
- DOI: http://doi.org/10.4055/cios.2019.11.4.466
Abstract
- BACKGROUND
Prophylactic pinning of the uninvolved side after unilateral slipped capital femoral epiphysis (SCFE) is controversial. The alpha angle, a measurement of femoral head-neck aspherity, was proposed as a predictor of progression of contralateral SCFE with a treatment threshold of greater than 50.5°. The aim of this study was to evaluate its validity in our cohort of patients.
METHODS
A retrospective review of a 10-year series of patients who presented with unilateral SCFE was conducted. Minimum follow-up duration to identify contralateral progression was 18 months. Age, sex, ethnicity, and endocrinopathies were noted. Alpha angle measurements of the unaffected hip were performed by two independent observers. The average values of measurements were used for analysis. Univariate and multivariate logistic regression analyses were performed to identify predictors of contralateral progression. A receiver operating characteristic (ROC) curve was generated.
RESULTS
There were 43 patients with unilateral SCFE. Seven patients (16.3%) developed contralateral SCFE. There were 31 males (72.1%) and 12 females (27.9%). The mean duration from index surgery to contralateral fixation was 43.9 weeks (range, 16.2 to 77 weeks). The mean alpha angle was significantly higher in the patients with contralateral progression (mean, 50.7°; standard deviation [SD], 5.4°; range, 43.8° to 58.5°) than in the patients without progression (mean, 43.0°; SD, 4.2°; range, 33.0° to 52.5°; p < 0.001). The alpha angle was also identified as a statistically significant predictor of contralateral progression on multivariate analysis (p = 0.02). The intraclass correlation coefficient for interobserver reliability was moderately strong at 0.76 (95% confidence interval, 0.55 to 0.87). The area under the ROC curve was 0.88. The treatment threshold of 50.5° had a sensitivity of 0.43, specificity of 0.94, and number needed to treat (NNT) of 2.7. The ideal treatment threshold derived from the ROC curve was 49.0°, which had a sensitivity of 0.71, specificity of 0.89, and an NNT of 1.7.
CONCLUSIONS
Alpha angle is a potential predictor of contralateral hip involvement in children with SCFE who may benefit from prophylactic hip fixation. Results from our series suggest a treatment threshold be 49.0°. However, given the limited sample size and moderately strong interobserver reliability, larger studies are needed to validate our findings.
MeSH Terms
Figure
-
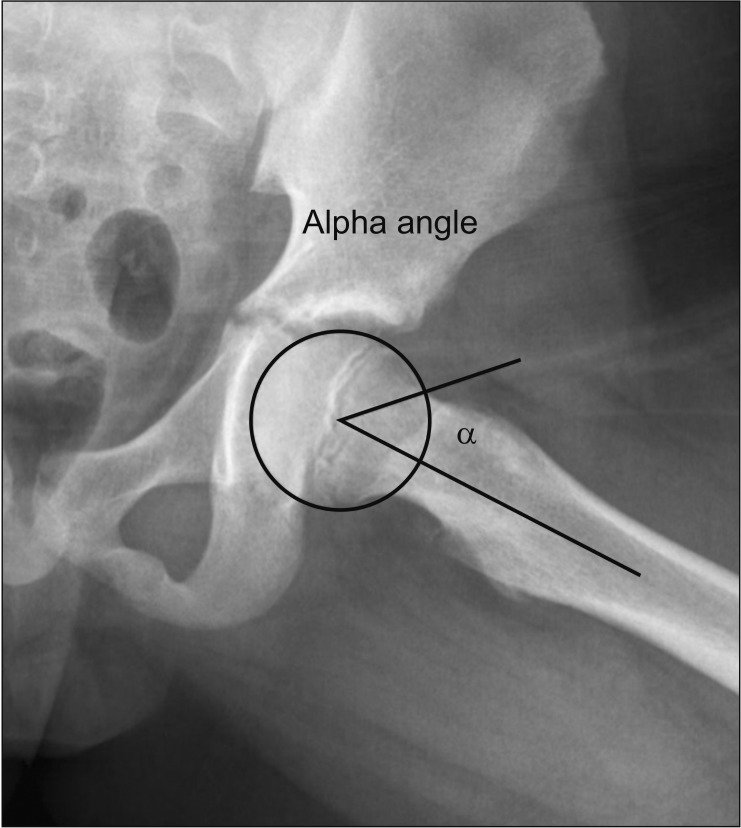
Fig. 1 Measurement of the alpha angle.
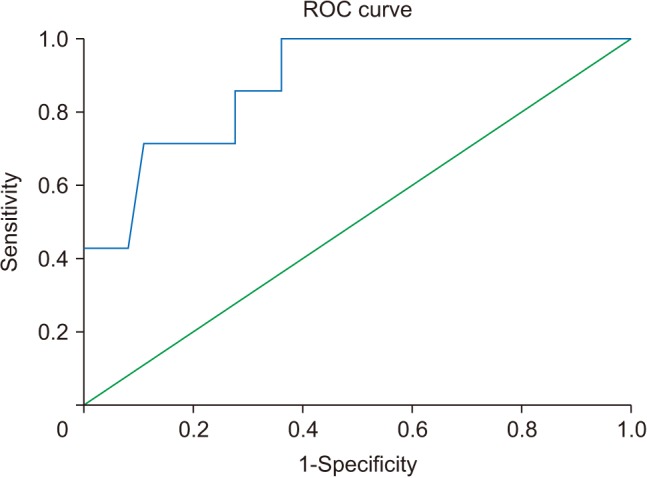
Fig. 2 The receiver operating characteristic (ROC) curve for alpha angle with respect to contralateral progression.
Reference
-
1. Loder RT. The demographics of slipped capital femoral epiphysis: an international multicenter study. Clin Orthop Relat Res. 1996; (322):8–27. PMID: 8542716.
Article2. Aronsson DD, Loder RT, Breur GJ, Weinstein SL. Slipped capital femoral epiphysis: current concepts. J Am Acad Orthop Surg. 2006; 14(12):666–679. PMID: 17077339.
Article3. Castro FP Jr, Bennett JT, Doulens K. Epidemiological perspective on prophylactic pinning in patients with unilateral slipped capital femoral epiphysis. J Pediatr Orthop. 2000; 20(6):745–748. PMID: 11097247.
Article4. Loder RT, Aronson DD, Greenfield ML. The epidemiology of bilateral slipped capital femoral epiphysis: a study of children in Michigan. J Bone Joint Surg Am. 1993; 75(8):1141–1147. PMID: 8354672.
Article5. Lim YJ, Lam KS, Lee EH. Review of the management outcome of slipped capital femoral epiphysis and the role of prophylactic contra-lateral pinning re-examined. Ann Acad Med Singapore. 2008; 37(3):184–187. PMID: 18392295.6. Bidwell TA, Susan Stott N. Sequential slipped capital femoral epiphyses: who is at risk for a second slip? ANZ J Surg. 2006; 76(11):973–976. PMID: 17054545.
Article7. Nasreddine AY, Heyworth BE, Zurakowski D, Kocher MS. A reduction in body mass index lowers risk for bilateral slipped capital femoral epiphysis. Clin Orthop Relat Res. 2013; 471(7):2137–2144. PMID: 23378238.
Article8. Popejoy D, Emara K, Birch J. Prediction of contralateral slipped capital femoral epiphysis using the modified Oxford bone age score. J Pediatr Orthop. 2012; 32(3):290–294. PMID: 22411336.
Article9. Loder RT, Hensinger RN. Slipped capital femoral epiphysis associated with renal failure osteodystrophy. J Pediatr Orthop. 1997; 17(2):205–211. PMID: 9075097.
Article10. Loder RT, Wittenberg B, DeSilva G. Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop. 1995; 15(3):349–356. PMID: 7790494.
Article11. Gelberman RH, Cohen MS, Shaw BA, Kasser JR, Griffin PP, Wilkinson RH. The association of femoral retroversion with slipped capital femoral epiphysis. J Bone Joint Surg Am. 1986; 68(7):1000–1007. PMID: 3745237.
Article12. Mirkopulos N, Weiner DS, Askew M. The evolving slope of the proximal femoral growth plate relationship to slipped capital femoral epiphysis. J Pediatr Orthop. 1988; 8(3):268–273. PMID: 3284904.
Article13. Phillips PM, Phadnis J, Willoughby R, Hunt L. Posterior sloping angle as a predictor of contralateral slip in slipped capital femoral epiphysis. J Bone Joint Surg Am. 2013; 95(2):146–150. PMID: 23324962.
Article14. Hagglund G. Pinning the slipped and contralateral hips in the treatment of slipped capital femoral epiphysis. J Child Orthop. 2017; 11(2):110–113. PMID: 28529658.
Article15. Sankar WN, Novais EN, Lee C, Al-Omari AA, Choi PD, Shore BJ. What are the risks of prophylactic pinning to prevent contralateral slipped capital femoral epiphysis? Clin Orthop Relat Res. 2013; 471(7):2118–2123. PMID: 23129473.
Article16. Kumm DA, Schmidt J, Eisenburger SH, Rutt J, Hackenbroch MH. Prophylactic dynamic screw fixation of the asymptomatic hip in slipped capital femoral epiphysis. J Pediatr Orthop. 1996; 16(2):249–253. PMID: 8742295.
Article17. Schultz WR, Weinstein JN, Weinstein SL, Smith BG. Prophylactic pinning of the contralateral hip in slipped capital femoral epiphysis: evaluation of long-term outcome for the contralateral hip with use of decision analysis. J Bone Joint Surg Am. 2002; 84(8):1305–1314. PMID: 12177258.18. Yildirim Y, Bautista S, Davidson RS. Chondrolysis, osteonecrosis, and slip severity in patients with subsequent contralateral slipped capital femoral epiphysis. J Bone Joint Surg Am. 2008; 90(3):485–492. PMID: 18310697.
Article19. Jerre R, Billing L, Hansson G, Karlsson J, Wallin J. Bilaterality in slipped capital femoral epiphysis: importance of a reliable radiographic method. J Pediatr Orthop B. 1996; 5(2):80–84. PMID: 8811535.20. Park S, Hsu JE, Rendon N, Wolfgruber H, Wells L. The utility of posterior sloping angle in predicting contralateral slipped capital femoral epiphysis. J Pediatr Orthop. 2010; 30(7):683–689. PMID: 20864853.
Article21. Mestriner MB, Verquietini CM, Waisberg G, Akkari M, Fukunaga ET, Santili C. Radiographic evaluation in epiphysiolysis: possible predictors of bilaterality? Acta Ortop Bras. 2012; 20(4):203–206. PMID: 24453602.22. Boyle MJ, Lirola JF, Hogue GD, Yen YM, Millis MB, Kim YJ. The alpha angle as a predictor of contralateral slipped capital femoral epiphysis. J Child Orthop. 2016; 10(3):201–207. PMID: 27052742.
Article23. Notzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br. 2002; 84(4):556–560. PMID: 12043778.24. Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005; 87(7):1012–1018. PMID: 15972923.25. Dudda M, Kim YJ, Zhang Y, et al. Morphologic differences between the hips of Chinese women and white women: could they account for the ethnic difference in the prevalence of hip osteoarthritis? Arthritis Rheum. 2011; 63(10):2992–2999. PMID: 21647861.
Article26. Erickson JB, Samora WP, Klingele KE. Treatment of chronic, stable slipped capital femoral epiphysis via surgical hip dislocation with combined osteochondroplasty and Imhauser osteotomy. J Child Orthop. 2017; 11(4):284–288. PMID: 28904634.
Article27. Sikora-Klak J, Bomar JD, Paik CN, Wenger DR, Upasani V. Comparison of surgical outcomes between a triplane proximal femoral osteotomy and the modified Dunn procedure for stable, moderate to severe slipped capital femoral epiphysis. J Pediatr Orthop. 2019; 39(7):339–346. PMID: 31305376.
Article28. Leunig M, Casillas MM, Hamlet M, et al. Slipped capital femoral epiphysis: early mechanical damage to the acetabular cartilage by a prominent femoral metaphysis. Acta Orthop Scand. 2000; 71(4):370–375. PMID: 11028885.
Article29. Lehmann TG, Engesaeter IO, Laborie LB, Lie SA, Rosendahl K, Engesaeter LB. Radiological findings that may indicate a prior silent slipped capital femoral epiphysis in a cohort of 2072 young adults. Bone Joint J. 2013; 95(4):452–458. PMID: 23539695.
Article30. Monazzam S, Bomar JD, Dwek JR, Hosalkar HS, Pennock AT. Development and prevalence of femoroacetabular impingement-associated morphology in a paediatric and adolescent population: a CT study of 225 patients. Bone Joint J. 2013; 95(5):598–604. PMID: 23632667.31. Gollwitzer H, Suren C, Struwind C, et al. The natural alpha angle of the femoral head-neck junction: a cross-sectional CT study in 1312 femurs. Bone Joint J. 2018; 100(5):570–578. PMID: 29701093.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Clinical Study of Slipped Capital Femoral epiphysis
- Pathologic Separation of Capital Femoral Epiphysis due to an Osteosarcoma
- Prognostic Factors in Slipped Capital Femoral Epiphysis
- Slipped Femoral Capital Epiphysis: Report of Two Cases
- Bilateral Subtrochanteric fracture After Pin Removal in Slipped Capital Femoral Epiphysis: A Case Report
